Statins are a type of medication used to lower the level of bad cholesterol in the blood and reduce build-up in arteries that can cause a heart attack or stroke. This short animated video explains the importance of statins, how they work, and why your doctor may prescribe them.

DR. C’S MEDICINE CABINET: BENEFITS & RISKS OF ‘STATINS’
The STATIN medications are one of medicine’s greatest achievements, in my opinion. They REDUCE blood CHOLESTEROL and HEART ATTACKS in very low doses and have a good safety profile. They truly deserve to be the Best Selling class of drugs. 13 Nobel prizes have been awarded during the centuries of cholesterol research.
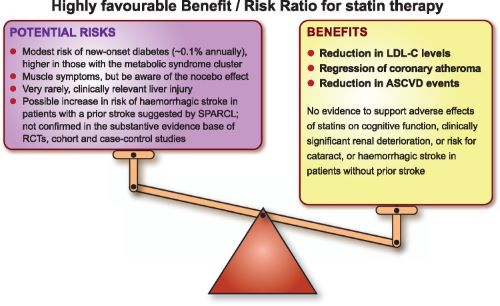
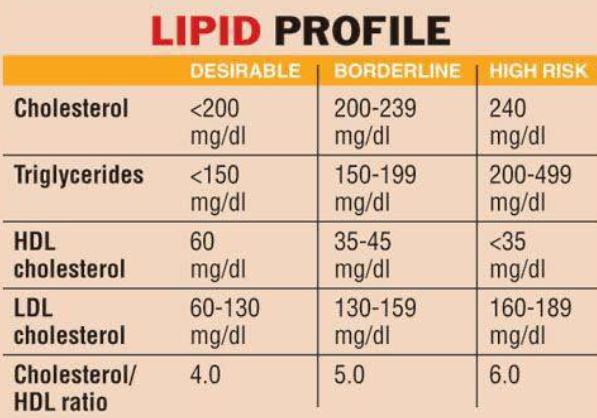
I have never had a heart attack, but do have some calcification in my Coronaries. Moreover, I have an untreated serum cholesterol level of 220 mg/dL. This is above the recommended level of 200 mg/dL, so I read up on the statins. The only concerning side effect from my viewpoint was MUSCLE PAIN.
I already have some muscle soreness from my exercise program, and did not want more, so I started at ½ of the 5 mg. dose of the statin suggested by my family doctor. This tiny dose of Rosuvastatin produced a dramatic 40 mg. Drop in my Cholesterol, and I am still hovering around the recommended level of 200 mg./dL. Instead of breaking the 5 mg. tablet in half, I now take 5 mg. every other day, since Rosuvastatin has a long half life.
One of my friends took a higher dose, and drove his cholesterol down to 100 Mg./dL. Apparently there is no serum level of cholesterol where further reduction fails to help.
Total cholesterol is divided into HDL and LDL components. My HDL, the “good” cholesterol, is thought to offset some of the cholesterol-plaque-causing effects of the LDL, or “bad” cholesterol. This makes me less than eager to raise my cholesterol and risk muscle pain.
My HIGH HDL is probably due to a combination of EXERCISE, FISH OIL and Genetics. Many of my friends “don’t tolerate” the statins, meaning that they developed muscle pain. Since they were taking the drug on faith, and not because of already-developed heart problems, they just don’t take the medication any more.
If your doctor has recommended one of the Statin drugs because of an elevated cholesterol, you might ask her to start at a lower dose. You can always work up to a higher dose if necessary. If you develop muscle pain at the higher dose, you can drop back to the dose you tolerated. Enjoy “Personalized” Medicine.
–Dr. C.

MEDICINE: ‘THREE CRITICAL BREAKTHROUGHS IN STROKE RESEARCH’ (YALE VIDEO)
Stroke is far more common than you might realize, affecting more than 795,000 people in the U.S. every year. It is a leading cause of death and long-term disability. Yet until now, treatment options have been limited, despite the prevalence and severity of stroke.
Not so long ago, doctors didn’t have much more to offer stroke victims than empathy, says Kevin Sheth, MD, Division Chief of Neurocritical Care and Emergency Neurology. “There wasn’t much you could do.” But that is changing. Recent breakthroughs offer new hope to patients and families. Beating the Clock Think of stroke as a plumbing problem in the brain. It occurs when there is a disruption of blood flow, either because of a vessel blockage (ischemic stroke) or rupture (hemorrhagic stroke).
In both cases, the interruption of blood flow starves brain cells of oxygen, causing them to become damaged and die. Delivering medical interventions early after a stroke can mean the difference between a full recovery and significant disability or death. Time matters. Unfortunately, stroke care often bottlenecks in the first stage: diagnosis. Sometimes, it’s a logistical issue; to identify the type, size, and location of a stroke requires MRI imaging, and the machinery itself can be difficult to access.
MRIs use powerful magnets to create detailed images of the body, which means they must be kept in bunker-type rooms, typically located in hospital basements. As a result, there is often a delay in getting MRI scans for stroke patients. Dr. Sheth collaborated with a group of doctors and engineers to develop a portable MRI machine. Though it captures the images doctors need to properly diagnose stroke, it uses a less powerful magnet. It is lightweight and can be easily wheeled to a patient’s bedside.
“It’s a paradigm shift – from taking a sick patient to the MRI to taking an MRI to a sick patient,” says Dr. Sheth. Stopping the Damage Once a stroke has been diagnosed, the work of mitigating the damage can begin. “Brain tissue is very vulnerable during the first hours after stroke,” says vascular neurologist Nils Petersen, MD. He and his team are using advanced neuro-monitoring technology to study how to manage a patient’s blood pressure in the very acute phase after a stroke.
Dr. Petersen’s research shows that optimal stroke treatment depends on personalization of blood pressure parameters. But calculating the ideal blood pressure for the minutes and hours after a patient has a stroke can be complicated. It depends on a variety of factors—it is not a one-size-fits-all scenario. Harnessing the Immune System Launching an inflammatory reaction is how the body responds to injury anywhere in the body – including the brain, following stroke. However, in this case, the resulting inflammation can sometimes cause even more damage.
But what if that immune response could be used to the patient’s advantage? “We’re trying to understand how we can harness the immune system’s knowledge about how to repair tissues after they’ve been injured,” says Lauren Sansing, MD, Academic Chief of the Division of Stroke and Vascular Neurology. Her team is working to understand the biological signals guiding the immune response to stroke.
That knowledge can then direct the development of targeted therapeutics for the treatment of stroke that minimize early injury and enhance recovery. “We want to be able to lead research efforts that change the lives of patients around the world,” says Dr. Sansing.
Learn about these developments and more in the video above.
For more information on aneurysms or #YaleMedicine, visit: https://www.yalemedicine.org/conditio…

PATIENT EDUCATION: THE “2020 WEEKLY CROSSWORD PUZZLE CHALLENGE” (DEC 7)

METABOLOMICS: NEW DIET STUDIES ARE IMPROVED WITH CELL METABOLISM DATA – “BLOOD & URINE DON’T LIE”


DR. C’S PODCAST: WEEKLY MEDICAL NEWS (DEC 6)
DR. C REVIEWS MAJOR HEALTH AND TELEMEDICAL NEWS FOR THE WEEK ENDING DECEMBER 6, 2020.

HEALTH: ‘AT-HOME COVID-19 TESTS’ – ON THE WAY (VIDEO)
OraSure Technologies has blazed a trail in at-home diagnostic tests. Now, the Pennsylvania-based biotech company is working to produce a quick, over-the-counter coronavirus test that consumers can take in the privacy of their home with results available in minutes. NPR’s Allison Aubrey reports.

THE DOCTORS 101 CHRONIC SYMPTOMS AND CONDITIONS #27: DELIRIUM
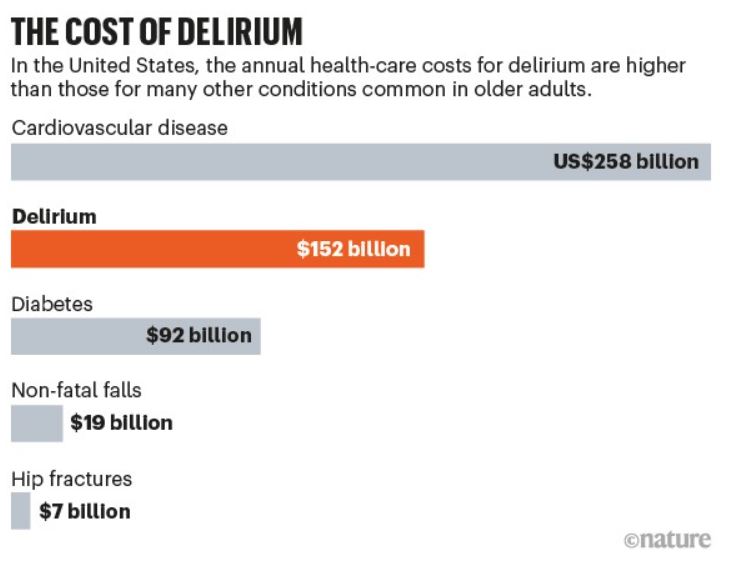
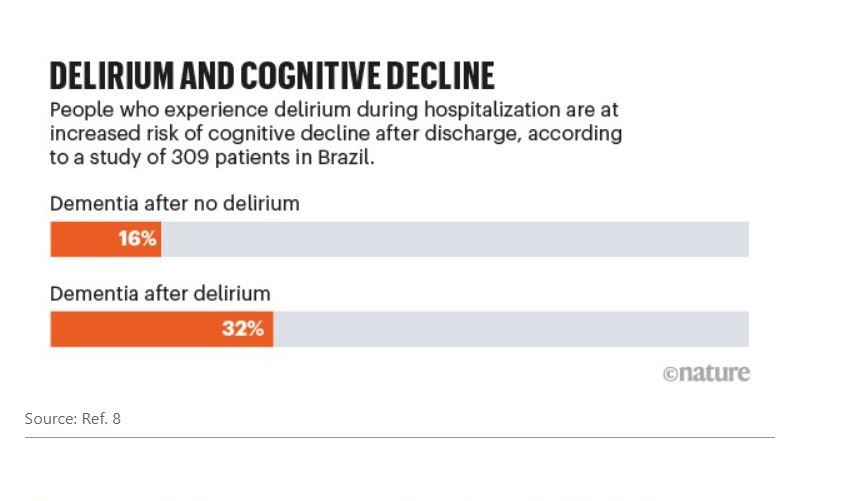
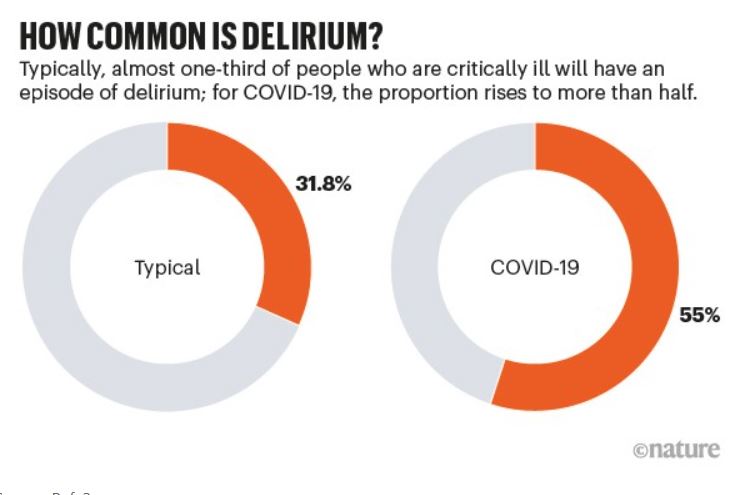
DELIRIUM is a rapidly-developing TEMPORARY DEMENTIA in response to almost any trauma, infection or stress, usually in a hospital setting, with its restrictive, isolating and disorienting environment.
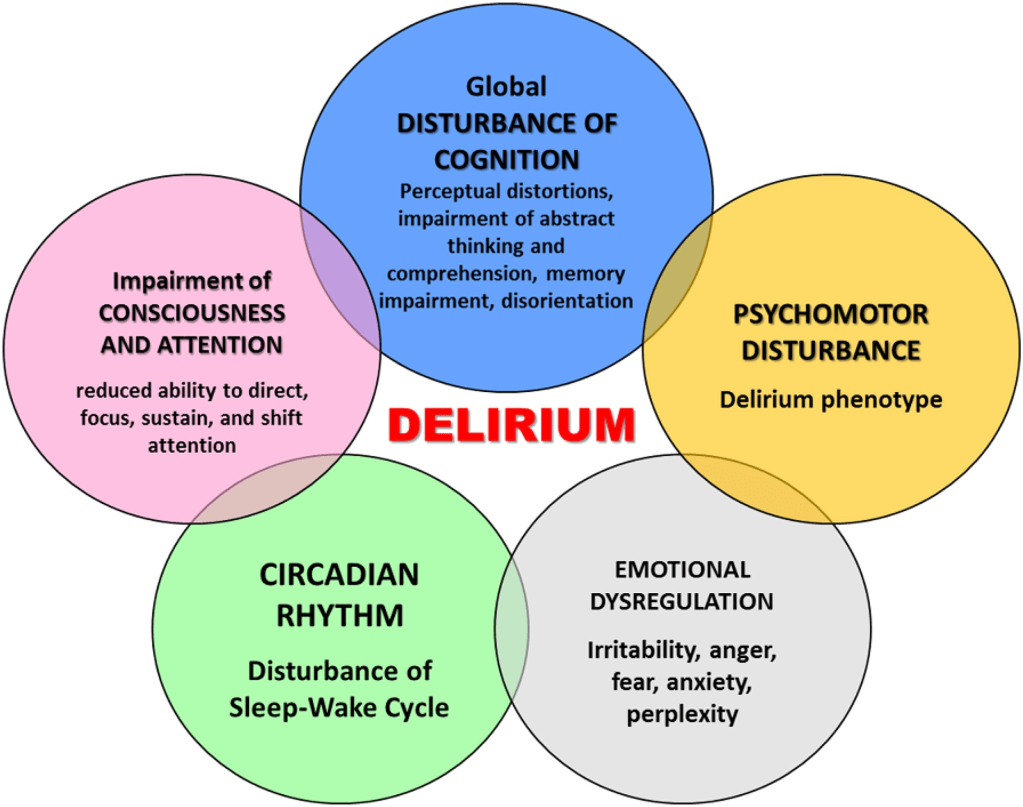
I had little appreciation of the frequency or economic hazard of Delirium before I encountered this infographic. I knew little about the causative mechanisms, and after reading about it, I still don’t know what is going on. But I do know one thing; I don’t want to become delirious and risk its ominous outcome. To improve my odds, I want to keep myself as healthy as possible.
To prevent loss of focus, cognition and memory, challenge the Brain as much as possible. To prevent or restrain infection, support the immune system with a healthy diet. To combat sleep disturbances, practice Sleep Hygiene. To maintain adequate oxygen and nutrient delivery to the Brain, support a healthy cardiovascular-pulmonary system with regular aerobic exercise.
These preventative steps will also postpone the FRAILTY on which delirium feeds. This fuzziness, which afflicts most conditions with PSYCHIATRIC OVERTONES, should not be surprising, since the human Brain, the location of Delirium, is the most complex entity in the known universe.
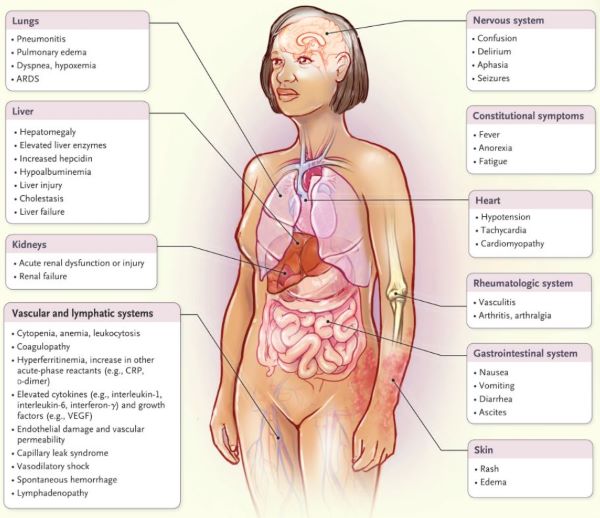
Medical Knowledge of Delirium is still at the descriptive stage, even though it has been a feature of human life since Ancient times. Causation? Excess or Deficiency of most neurotransmitters have been described. To paraphrase “cytokine storm”, which can incidentally cause Delirium, one could call the condition a “neurotransmitter storm”.
Treatment? If the Delirious Patient is on a Psychotropic medication, try stopping it. If not taking such medication, try starting it. The only universal green light is Good general supportive care with IV fluids, oxygen, nutrition, and psychological support, with gentle, regular attention. Please read the accompanying Mayo Clinic article for a more conventional discussion.