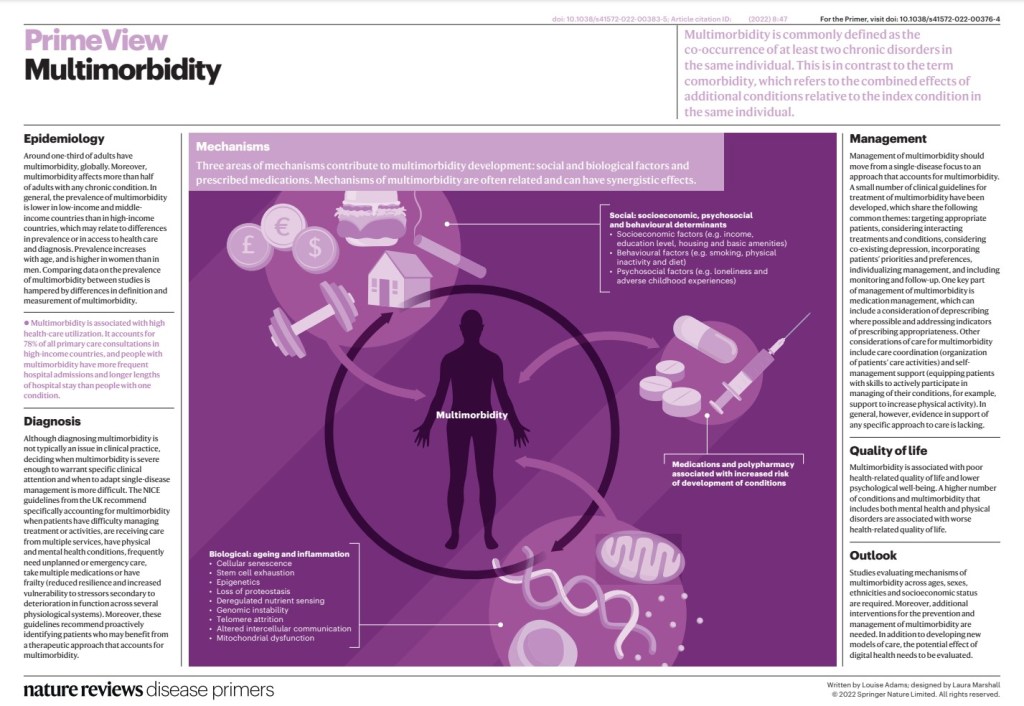
People with multimorbidity (two or more coexisting conditions in an individual) are more likely to die prematurely, be admitted to hospital and have an increased length of stay than people with a single chronic condition.
Multimorbidity is also associated with poorer function and health-related quality of life (HRQOL), depression and intake of multiple drugs (polypharmacy) and greater socioeconomic costs. Most health care is designed to treat individual conditions rather than providing comprehensive, person-centreed care, which often leads to fragmented and sometimes contradictory care for people with multimorbidity and increases their treatment burden. Moreover, treating one condition at a time is inefficient and unsatisfactory for both people with multimorbidity and their health-care providers.
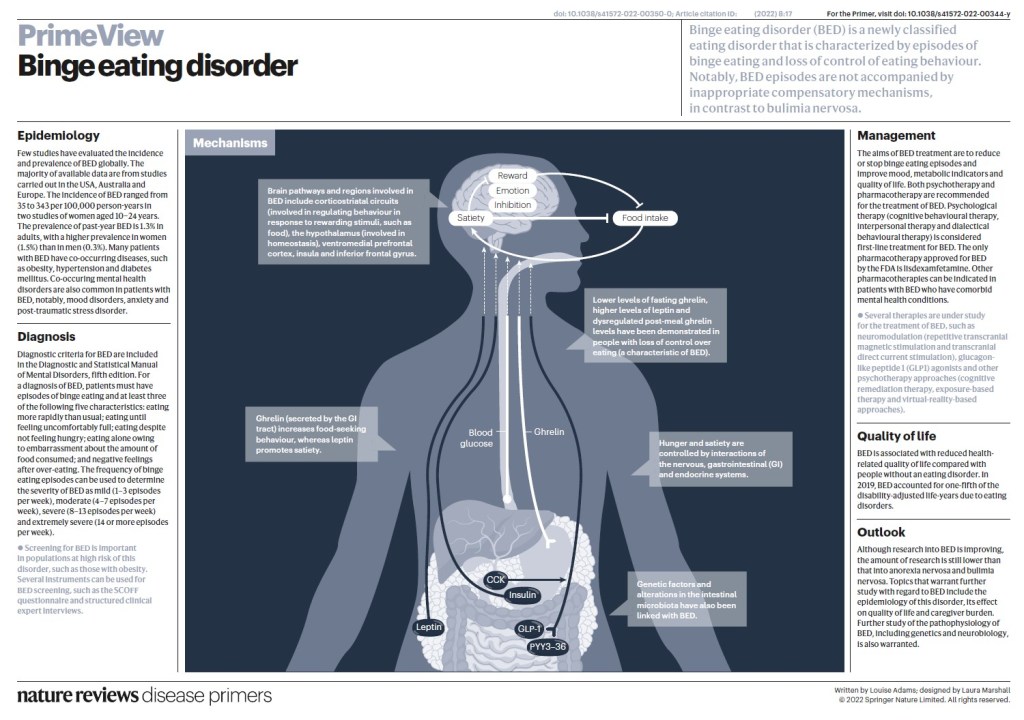
Most people with binge-eating disorder are overweight or obese, but you may be at a normal weight. Behavioral and emotional signs and symptoms of binge-eating disorder include:
Eating unusually large amounts of food in a specific amount of time, such as over a two-hour period
Feeling that your eating behavior is out of control
Eating even when you’re full or not hungry
Eating rapidly during binge episodes
Eating until you’re uncomfortably full
Frequently eating alone or in secret
Feeling depressed, disgusted, ashamed, guilty or upset about your eating
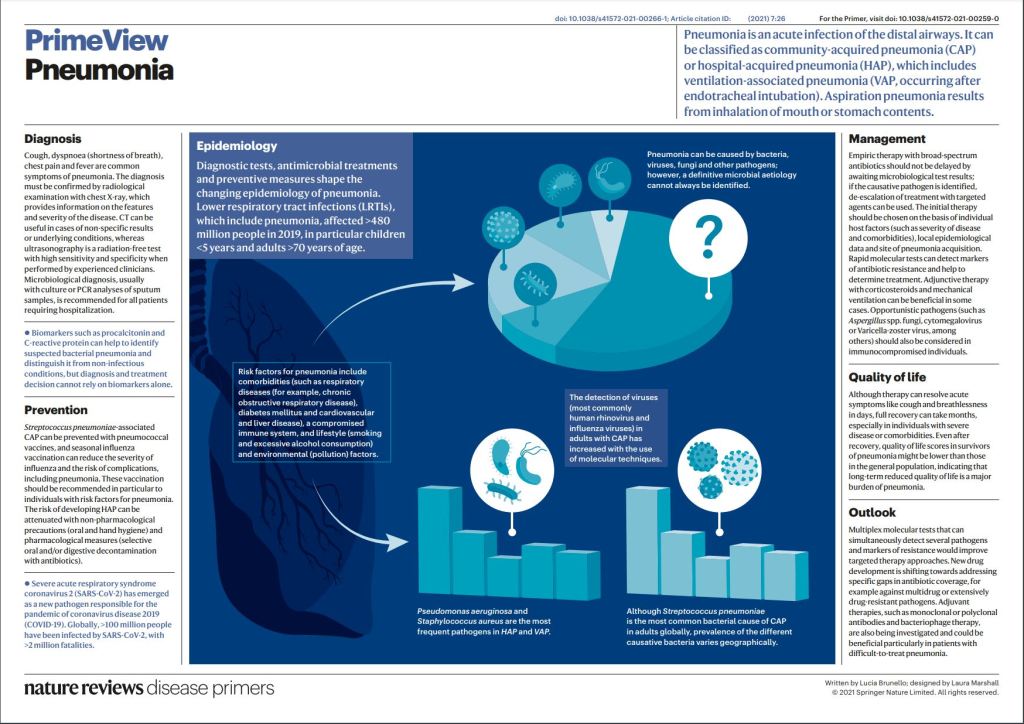
Pneumonia is a common acute respiratory infection that affects the alveoli and distal airways; it is a major health problem and associated with high morbidity and short-term and long-term mortality in all age groups worldwide. Pneumonia is broadly divided into community-acquired pneumonia or hospital-acquired pneumonia.
A large variety of microorganisms can cause pneumonia, including bacteria, respiratory viruses and fungi, and there are great geographical variations in their prevalence. Pneumonia occurs more commonly in susceptible individuals, including children of <5 years of age and older adults with prior chronic conditions. Development of the disease largely depends on the host immune response, with pathogen characteristics having a less prominent role. Individuals with pneumonia often present with respiratory and systemic symptoms, and diagnosis is based on both clinical presentation and radiological findings.
It is crucial to identify the causative pathogens, as delayed and inadequate antimicrobial therapy can lead to poor outcomes. New antibiotic and non-antibiotic therapies, in addition to rapid and accurate diagnostic tests that can detect pathogens and antibiotic resistance will improve the management of pneumonia.
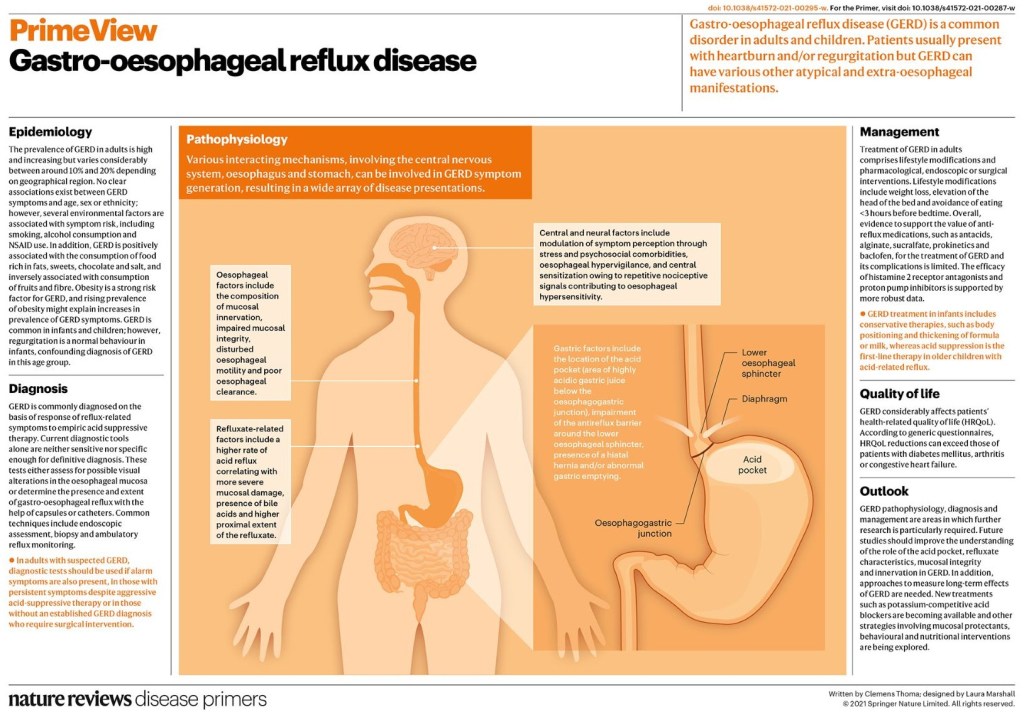
Gastro-oesophageal reflux disease (GERD) is a common disorder in adults and children. The global prevalence of GERD is high and increasing. Non-erosive reflux disease is the most common phenotype of GERD. Heartburn and regurgitation are considered classic symptoms but GERD may present with various atypical and extra-oesophageal manifestations. The pathophysiology of GERD is multifactorial and different mechanisms may result in GERD symptoms, including gastric composition and motility, anti-reflux barrier, refluxate characteristics, clearance mechanisms, mucosal integrity and symptom perception.
In clinical practice, the diagnosis of GERD is commonly established on the basis of response to anti-reflux treatment; however, a more accurate diagnosis requires testing that includes upper gastrointestinal tract endoscopy and reflux monitoring. New techniques and new reflux testing parameters help to better phenotype the condition. In children, the diagnosis of GERD is primarily based on history and physical examination and treatment vary with age.
Treatment in adults includes a combination of lifestyle modifications with pharmacological, endoscopic or surgical intervention. In refractory GERD, optimization of proton-pump inhibitor treatment should be attempted before a series of diagnostic tests to assess the patient’s phenotype.
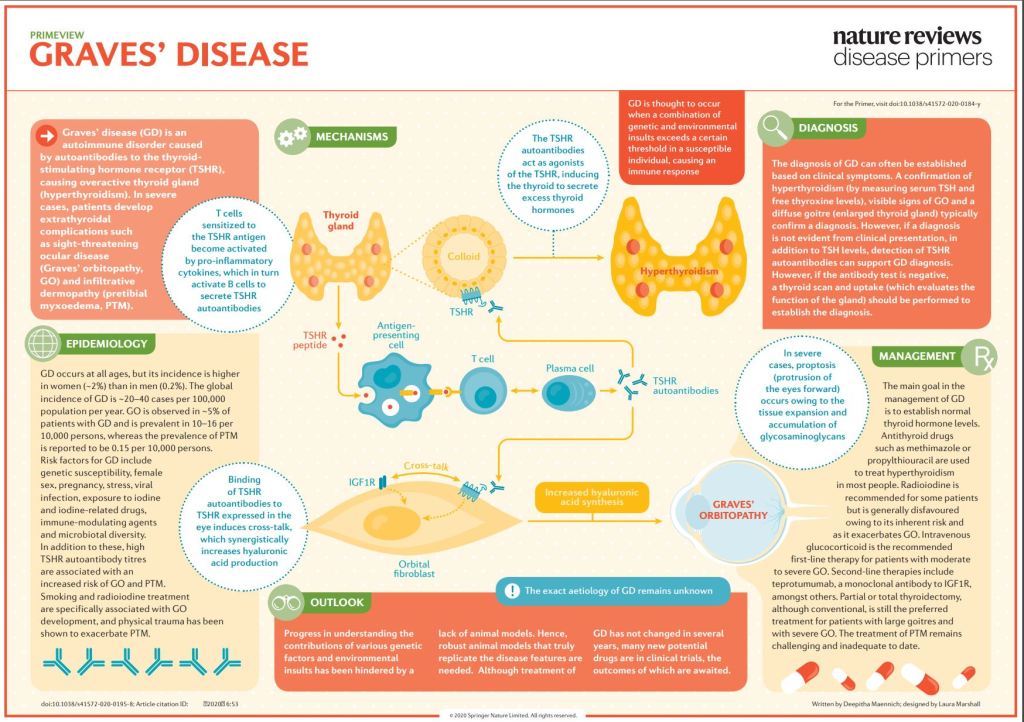
Graves’ disease is an immune system disorder that results in the overproduction of thyroid hormones (hyperthyroidism). Although a number of disorders may result in hyperthyroidism, Graves’ disease is a common cause.
Thyroid hormones affect many body systems, so signs and symptoms of Graves’ disease can be wide ranging. Although Graves’ disease may affect anyone, it’s more common among women and in people younger than age 40.
The primary treatment goals are to reduce the amount of thyroid hormones that the body produces and lessen the severity of symptoms.
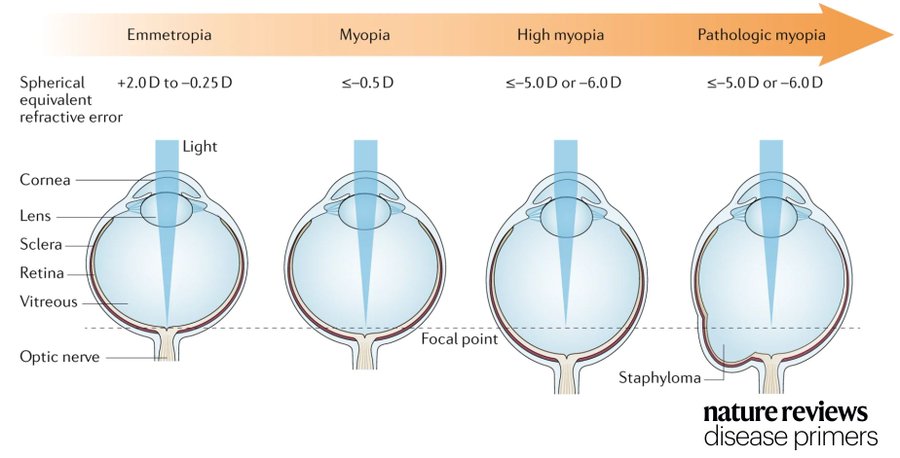
Myopia, also known as short-sightedness or near-sightedness, is a very common condition that typically starts in childhood. Severe forms of myopia (pathologic myopia) are associated with a risk of other associated ophthalmic problems. This disorder affects all populations and is reaching epidemic proportions in East Asia, although there are differences in prevalence between countries.
Myopia is caused by both environmental and genetic risk factors. A range of myopia management and control strategies are available that can treat this condition, but it is clear that understanding the factors involved in delaying myopia onset and slowing its progression will be key to reducing the rapid rise in its global prevalence.
To achieve this goal, improved data collection using wearable technology, in combination with collection and assessment of data on demographic, genetic and environmental risk factors and with artificial intelligence are needed. Improved public health strategies focusing on early detection or prevention combined with additional effective therapeutic interventions to limit myopia progression are also needed.
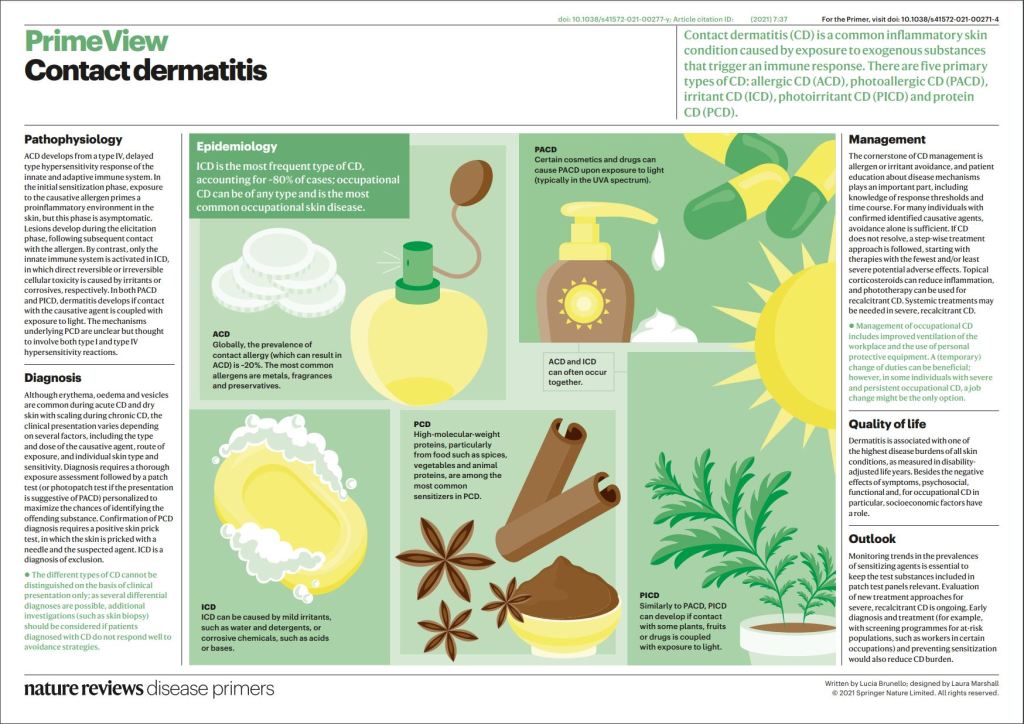
Contact dermatitis (CD) is among the most common inflammatory dermatological conditions and includes allergic CD, photoallergic CD, irritant CD, photoirritant CD (also called phototoxic CD) and protein CD. Occupational CD can be of any type and is the most prevalent occupational skin disease. Each CD type is characterized by different immunological mechanisms and/or requisite exposures. Clinical manifestations of CD vary widely and multiple subtypes may occur simultaneously. The diagnosis relies on clinical presentation, thorough exposure assessment and evaluation with techniques such as patch testing and skin-prick testing. Management is based on patient education, avoidance strategies of specific substances, and topical treatments; in severe or recalcitrant cases, which can negatively affect the quality of life of patients, systemic medications may be needed.
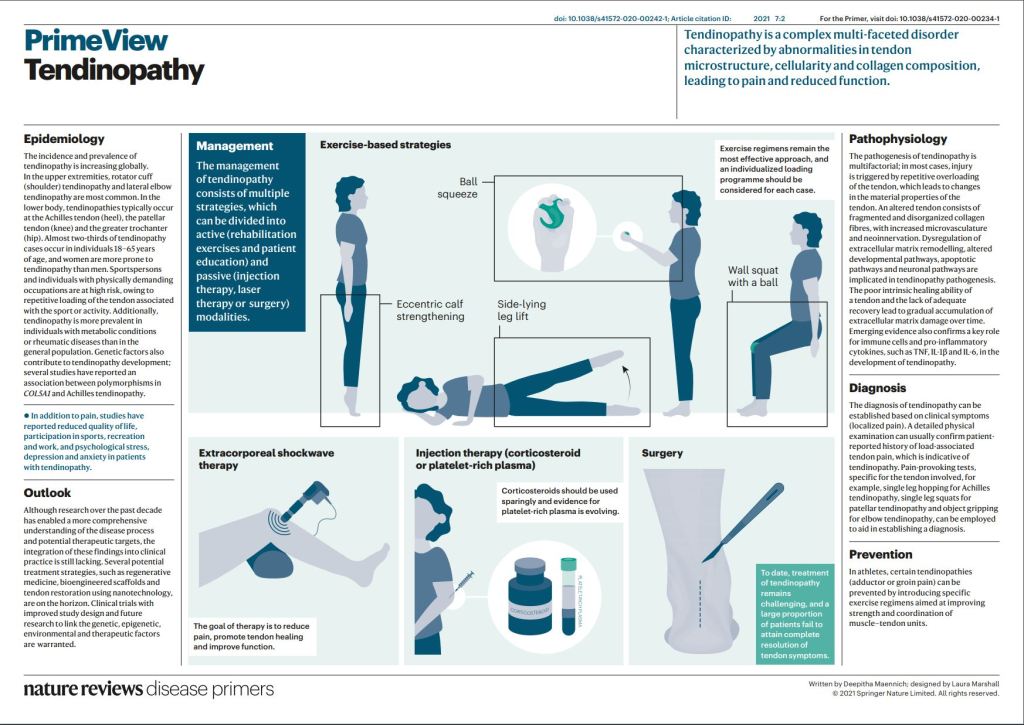
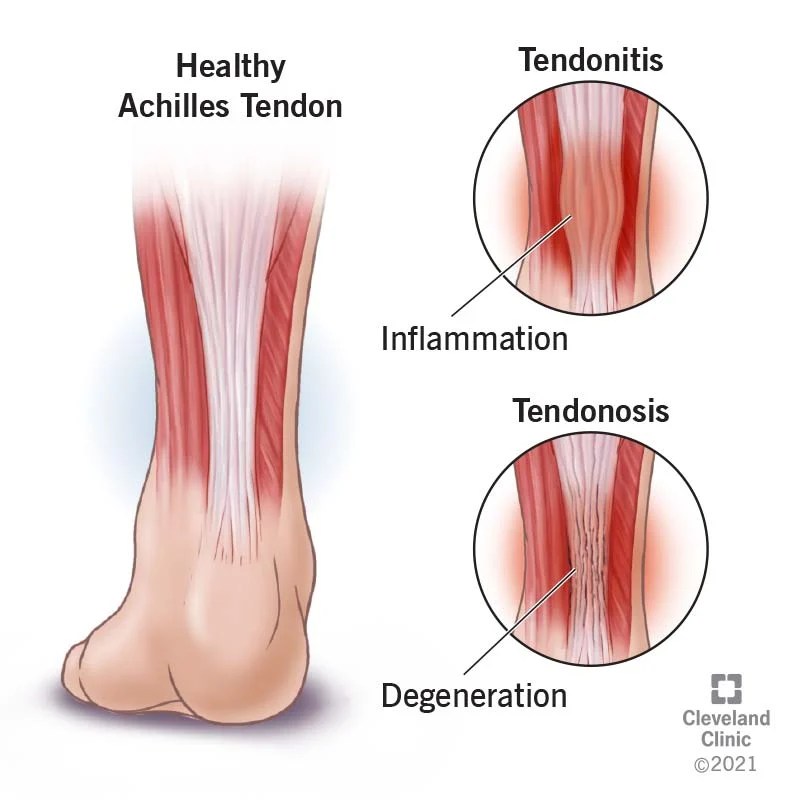
Tendinopathy is the broad term for any tendon condition that causes pain and swelling. Your tendons are rope-like tissues in your body that attach muscle to bone. When your muscles tighten and relax, your tendons and bones move. One example of a tendon is your Achilles tendon, which attaches your calf muscle to your heel bone and causes ankle movement. If you have pain and/or swelling in that area, you might have Achilles tendinopathy.
The pain from tendinopathy can interfere with your daily life. For example, it can keep you from playing sports and from doing housework. So, if you have pain or swelling, make sure to contact your healthcare provider for help.
Psoriasis is a skin disease that causes a rash with itchy, scaly patches, most commonly on the knees, elbows, trunk and scalp.
Psoriasis is a common, long-term (chronic) disease with no cure. It can be painful, interfere with sleep and make it hard to concentrate. The condition tends to go through cycles, flaring for a few weeks or months, then subsiding for a while. Common triggers in people with a genetic predisposition to psoriasis include infections, cuts or burns, and certain medications.
Treatments are available to help you manage symptoms. And you can try lifestyle habits and coping strategies to help you live better with psoriasis.
My practice was restricted to allergy, but I saw many patients with psoriasis. The red scaly patches made them think they had allergic dermatitis, eczema. Psoriasis on the arm is usually located on the elbow, and atopic dermatitis on the opposite side, in the flexural area. Thick, pitted fingernails are also common in psoriasis. It’s combination with arthritis is worrisome.
Psoriasis will usually develop first, and the psoriatic arthritis will follow years later, but 10% of the time the arthritis Is the first problem. This form of arthritis can be very painful, and cause deformities. It is often worse than rheumatoid arthritis, although does not affect as many joints, and is often asymmetrical. It inflames the area where tendons attach to the bone, which is one of the reasons that it can be more painful than rheumatoid arthritis.
Psoriasis is an autoimmune problem and can involve practically any organ in the body.
It is often associated with metabolic syndrome and diabetes.
Psoriatic arthritis does not have the rheumatoid serum markers that can help diagnose rheumatoid arthritis, and unless psoriasis is also present on the skin, it can be hard to diagnose.
Symptomatic treatment with NSAIDs, physical therapy, phototherapy and topical treatments can be helpful, but very expensive biologics are sometimes needed to help out methotrexate and other first line DMARDs (Disease modifying antirheumatic drugs).
This condition can be progressive. If you develop scaly red patches on your skin, be sure to check with the doctor about the possibility of psoriasis.
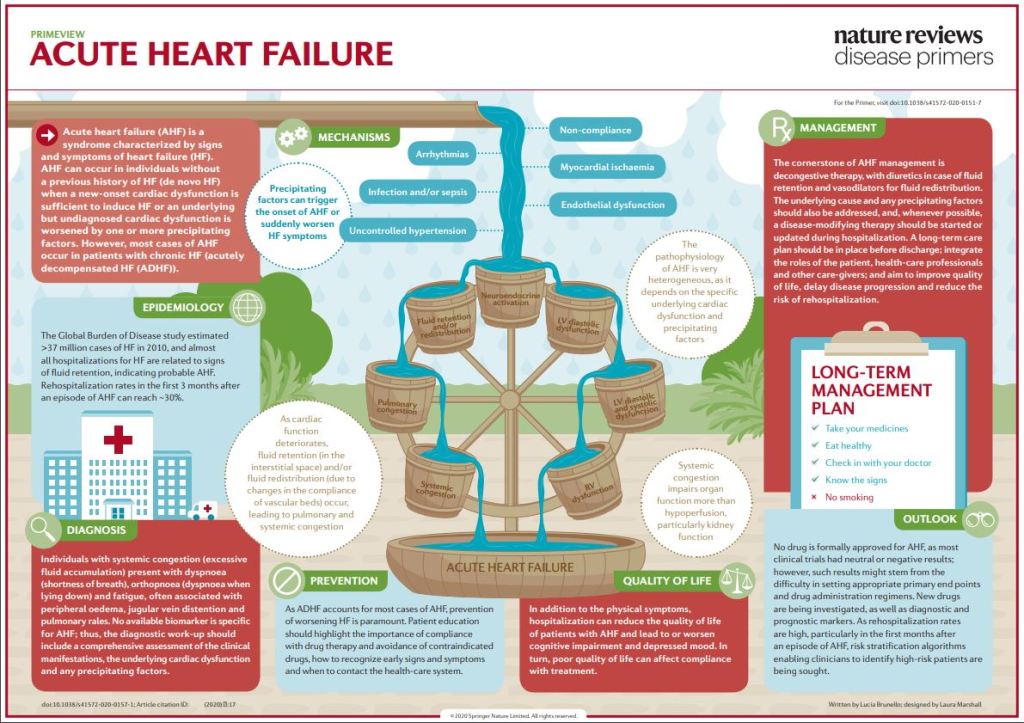
Acute heart failure (AHF) is a syndrome defined as the new onset (de novo heart failure (HF)) or worsening (acutely decompensated heart failure (ADHF)) of symptoms and signs of HF, mostly related to systemic congestion. In the presence of an underlying structural or functional cardiac dysfunction (whether chronic in ADHF or undiagnosed in de novo HF), one or more precipitating factors can induce AHF, although sometimes de novo HF can result directly from the onset of a new cardiac dysfunction, most frequently an acute coronary syndrome.
Despite leading to similar clinical presentations, the underlying cardiac disease and precipitating factors may vary greatly and, therefore, the pathophysiology of AHF is highly heterogeneous. Left ventricular diastolic or systolic dysfunction results in increased preload and afterload, which in turn lead to pulmonary congestion. Fluid retention and redistribution result in systemic congestion, eventually causing organ dysfunction due to hypoperfusion. Current treatment of AHF is mostly symptomatic, centred on decongestive drugs, at best tailored according to the initial haemodynamic status with little regard to the underlying pathophysiological particularities.
As a consequence, AHF is still associated with high mortality and hospital readmission rates. There is an unmet need for increased individualization of in-hospital management, including treatments targeting the causative factors, and continuation of treatment after hospital discharge to improve long-term outcomes.
COMMENTARY:
High frequency sound (ultrasound) bounces off of tissues, like an echo, and allows an electronic look at the heart. Doppler echocardiography is the doctors method of choice for evaluating a heart failure. One of the most important numbers determined by this method is the EJECTION FRACTION, which is a measure of heart efficiency. If the ejection fraction is low, let’s say below 45%, the heart is pumping out only 45% of its volume with each stroke, which means it must work harder to produce the same amount of circulation. The normal is about 60%.
This is the basis of SYSTOLIC Heart failure.
The test can also tell about blood coming into the heart; the early part of the blood entering is usually 80% of the total. If it drops, let’s say below 50%, it means the heart is stiff and resists blood coming in, which is the basis of DIASTOLIC heart failure.
FACES Is an acronym-mnemonic for the symptoms of heart failure. F is for FATIGUE.
A is for ACTIVITY LIMITATION. C is for CONGESTION in the lungs. E is for EDEMA, or swelling, usually of the ankles and legs. S is for SHORTNESS of BREATH.
If you want to remember a bit about heart failure, think about echoes and faces. If your Doctor orders an ultrasound with Doppler, be sure to ask about your ejection fraction and percent of blood that enters early, before the “atrial kick”. Being informed is always a good thing.
To be honest, I have never encountered a person who was given a Doppler echocardiogram and could tell me what his ejection fraction was, but I am eternally hopeful.
—Dr. C.
Empowering Patients Through Education And Telemedicine