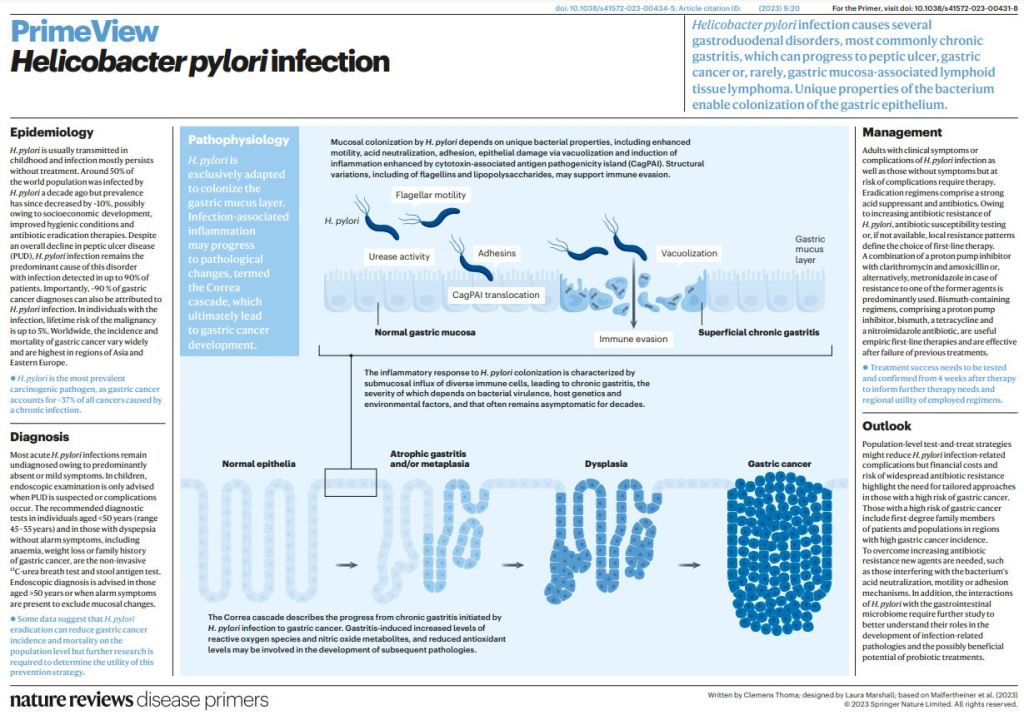
Helicobacter pylori infection causes chronic gastritis, which can progress to severe gastroduodenal pathologies, including peptic ulcer, gastric cancer and gastric mucosa-associated lymphoid tissue lymphoma. H. pylori is usually transmitted in childhood and persists for life if untreated. The infection affects around half of the population in the world but prevalence varies according to location and sanitation standards. H. pylori has unique properties to colonize gastric epithelium in an acidic environment.
The pathophysiology of H. pylori infection is dependent on complex bacterial virulence mechanisms and their interaction with the host immune system and environmental factors, resulting in distinct gastritis phenotypes that determine possible progression to different gastroduodenal pathologies. The causative role of H. pylori infection in gastric cancer development presents the opportunity for preventive screen-and-treat strategies. Invasive, endoscopy-based and non-invasive methods, including breath, stool and serological tests, are used in the diagnosis of H. pylori infection.
Their use depends on the specific individual patient history and local availability. H. pylori treatment consists of a strong acid suppressant in various combinations with antibiotics and/or bismuth. The dramatic increase in resistance to key antibiotics used in H. pylori eradication demands antibiotic susceptibility testing, surveillance of resistance and antibiotic stewardship.
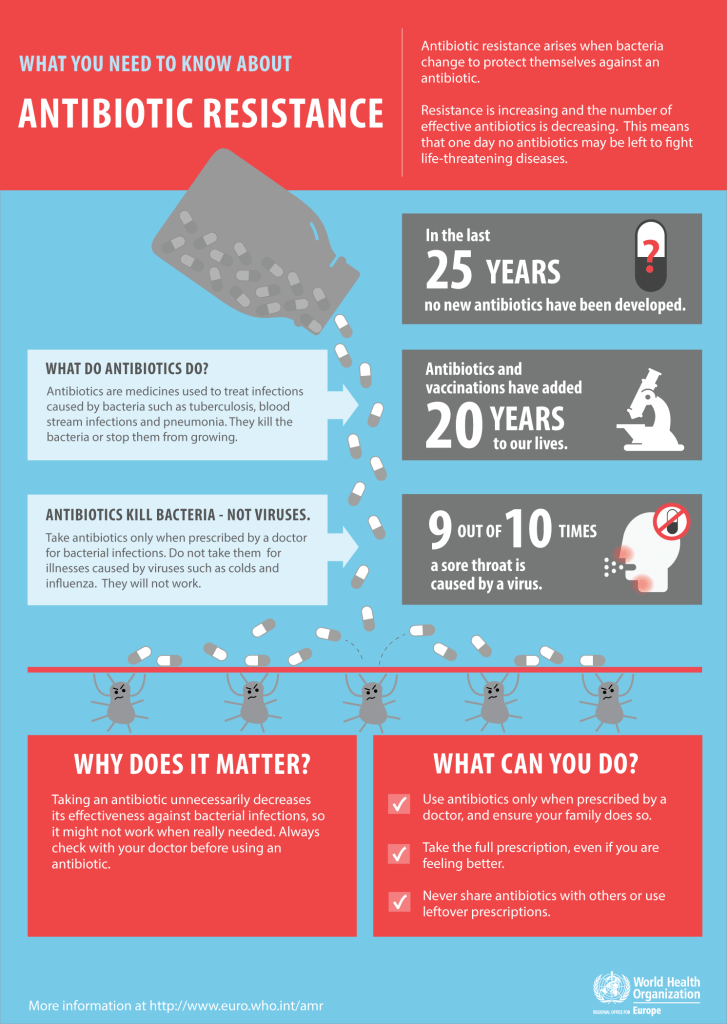
Each year in the US, more than two million individuals become sick with infections caused by antibiotic-resistant bacteria, and more than 23,000 die as a result of these infections. Antibiotic resistance happens when bacteria develop the ability to defeat the drugs designed to kill them.
Antibiotic resistance is a pressing public health issue, and together we can reduce this threat by optimizing antibiotic use and providing the best patient care. All stakeholders can play an important role in improving how antibiotics are used, to ensure that these drugs are available and effective when most needed.
NEJM Group (March 29, 2023) – In this Double Take video from the New England Journal of Medicine, Sam Telford and Robert Smith provide a clinical overview of the various tickborne diseases commonly encountered across the United States, including Lyme disease, babesiosis, and anaplasmosis, among others.
Starting with characteristics of ticks and their ability to act as disease vectors, the video reviews the clinical presentation of these infections, clues on physical examination, and laboratory tests to consider when encountering a patient with a potential tickborne infection.
Tick-borne diseases are transmitted through the bite of an infected tick. These include Lyme disease, Anaplasmosis, Ehrlichiosis, Babesiosis, Powassan (POW), Rocky Mountain Spotted Fever, and Tularemia. Ticks can be infected with bacteria, viruses, or parasites.
Pneumonia is an infection that inflames the air sacs in one or both lungs. The air sacs may fill with fluid or pus (purulent material), causing cough with phlegm or pus, fever, chills, and difficulty breathing. A variety of organisms, including bacteria, viruses and fungi, can cause pneumonia.
Mayo Clinic – Pneumonia can range in seriousness from mild to life-threatening. It is most serious for infants and young children, people older than age 65, and people with health problems or weakened immune systems.
Symptoms
The signs and symptoms of pneumonia vary from mild to severe, depending on factors such as the type of germ causing the infection, and your age and overall health. Mild signs and symptoms often are similar to those of a cold or flu, but they last longer.
Signs and symptoms of pneumonia may include:
Chest pain when you breathe or cough
Confusion or changes in mental awareness (in adults age 65 and older)
Cough, which may produce phlegm
Fatigue
Fever, sweating and shaking chills
Lower than normal body temperature (in adults older than age 65 and people with weak immune systems)
Nausea, vomiting or diarrhea
Shortness of breath
Newborns and infants may not show any sign of the infection. Or they may vomit, have a fever and cough, appear restless or tired and without energy, or have difficulty breathing and eating.
When to see a doctor
See your doctor if you have difficulty breathing, chest pain, persistent fever of 102 F (39 C) or higher, or persistent cough, especially if you’re coughing up pus.
It’s especially important that people in these high-risk groups see a doctor:
Adults older than age 65
Children younger than age 2 with signs and symptoms
People with an underlying health condition or weakened immune system
People receiving chemotherapy or taking medication that suppresses the immune system
For some older adults and people with heart failure or chronic lung problems, pneumonia can quickly become a life-threatening condition.
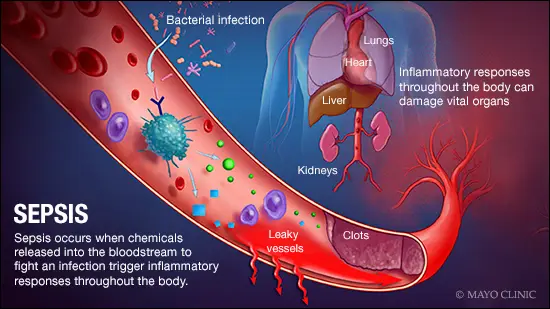
Sepsis occurs when the body’s response to an infection damages its own tissues. When these infection-fighting processes turn on the body, they cause organs to function poorly and abnormally.
As sepsis worsens, blood flow to vital organs, such as your brain, heart and kidneys, becomes impaired. Sepsis may cause abnormal blood clotting that results in small clots or burst blood vessels that damage or destroy tissues. If sepsis progresses to septic shock, blood pressure drops dramatically, which can lead to death.
Nearly 270,000 people in the U.S. die each year as a result of sepsis, and one-third of people who die in a hospital have sepsis, according to the Centers for Disease Control and Prevention.
Signs of sepsis
To be diagnosed with sepsis, you must have a probable or confirmed infection, and all of these signs:
Change in mental status.
Systolic blood pressure — the top number in a blood pressure reading — less than or equal to 100 millimeters of mercury, or mm Hg.
Respiratory rate higher than or equal to 22 breaths per minute.
Signs of progression to septic shock include:
The need for medication to maintain systolic blood pressure greater than or equal to 65 mm Hg.
High levels of lactic acid in your blood, which means that your cells aren’t using oxygen properly.
Treatment
Early, aggressive treatment increases the likelihood of recovery.
A number of medications are used to treat sepsis and septic shock, including antibiotics, corticosteroids, painkillers and sedatives. Supportive care, including oxygen and dialysis, and surgery to remove the source of the infection, also may be needed.
People who have sepsis require close monitoring and treatment in a hospital ICU. Lifesaving measures may be needed to stabilize breathing and heart function.
The hospital is a dangerous places to be, and the most common cause of death there is sepsis. Sepsis is an underappreciated killer, and it’s getting more common because people are aging, devices are more commonly implanted into the body, immunosuppressive treatment is being used more commonly, and hospital acquired infections are increasingly resistant to treatment.
Sepsis can be caused by an overwhelming infection with bacteria, but can also be caused by viruses, fungi, and severe trauma. Low blood pressure is a common problem, and is associated with change in mental status, and increased breathing rate in raising a red flag for sepsis. Endotoxins play an important, if confusing, role. Endotoxins derive from Gram negative bacteria, but the most common bacterium causing sepsis is the gram positive staphylococcus aureus. With sepsis, though,the gastrointestinal tract may become more leaky, and Gram negative organisms may thereby gain access to the blood stream.
A ccmmon test to detect sepsis is the serum lactate, which becomes elevated if oxygen utilization is diminished, such as in sepsis. There is also a direct test for endotoxin in the bloodstream, performed by using LAL, or Limulus amebocyte lysate. This substance, derived from the cells of the blood of the horseshoe crab, is very sensitive to endotoxins, and coagulates in its presence. This test is also used to detect endotoxins in Biological products and devices, making horseshoe crab is quite valuable.
Maintaining general health, keeping up on your immunizations, wishing your hands, keeping cuts and burns free from infection, ovoid smoking, controlling diabetes and avoiding hospitals whenever possible are useful preventative techniques.
We are immersed in a vast sea of tiny organisms, microbes, most of which are either helpful or neutral. There are a few bad actors that can harm people and are responsible for plagues of the past, such as the black death, cholera and influenza epidemics.
This whole picture changed in the late 30s with the advent of Sulfonamides, and especially Penicillin, the “magic bullet”. I was practicing medicine early in the days when antibiotics eliminated almost all infections.
In fact, at one time infections were thought to be a problem of the past. Unfortunately, overusage, chronic multiple infections, surgically implanted devices, immune suppression for cancer and autoimmune diseases have allowed bacteria, fungi and viruses to evolve resistance mechanisms.
At the present time there are a number of bacteria, such as staphylococci, actino bacteria, enterococci, and candida that are essentially untreatable. Even if they are somewhat treatable, second and third level antibiotics are so toxic that they can cause problems with the kidney, liver, or heart.
In later postings, I plan to consider specific organisms and the situations in which they operate. I will also eventually talk about efforts to create new antibiotics by harvesting genetic material from unusual places, even our oceans.
Lyme disease has infected more than 14% of the world’s population, according to a new study. “It’s significant,” says Dr. Bobbi Pritt, director of the Clinical Parasitology Laboratory at Mayo Clinic.
“If you look at the numbers and how it breaks down in regions across the United States, in some areas, that exceeds 50% seropositivity. That means people are walking around with antibodies in their blood that are detectable. That shows they’ve been exposed to Lyme disease at some point in their life,” says Dr. Pritt. “Now whether it was in the past and they’ve been successfully treated, or whether they have it right now, you can’t tell by that result, but it’s a marker of exposure.”
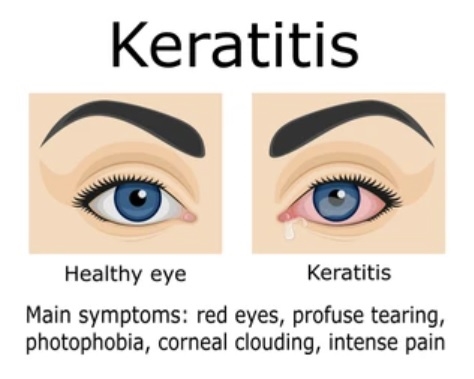
Herpetic Keratitis is a viral infection of the transparent, frontmost part of the eye, the cornea.
Herpes 1 or 2 when rubbed into the eye from a cold sore, or contacted from somebody else with herpes, will often affect the cornea. The use of corticosteroid eyedrops or ointment will allow the disease to spread faster.
The symptoms are pain and redness of the eye and are a medical emergency, needing prompt treatment by your doctor to prevent scarring and blindness.
Antiviral eyedrops, such as valacyclovir, are used to treat ophthalmic herpes.
A related condition is ophthalmic zoster, caused by the varicella zoster virus. The VZ virus will produce chickenpox in unimmunized people, go into dormancy in the nervous system, and then resurface, if immunity wanes, as shingles. If the shingles occurs in the ophthalmic division of the trigeminal nerve, affecting the skin near the eye, the cornea will often be involved. Ophthalmic zoster is also treated by antiviral eyedrops.
The varicella zoster virus is closely related to the herpes simplex virus, and is a member of the same nasty family of viruses.
Viral hepatitis is an infection that causes liver inflammation and damage. Inflammation is swelling that occurs when tissues of the body become injured or infected. Inflammation can damage organs. Researchers have discovered several different viruses link that cause hepatitis, including hepatitis A, B, C, D, and E.
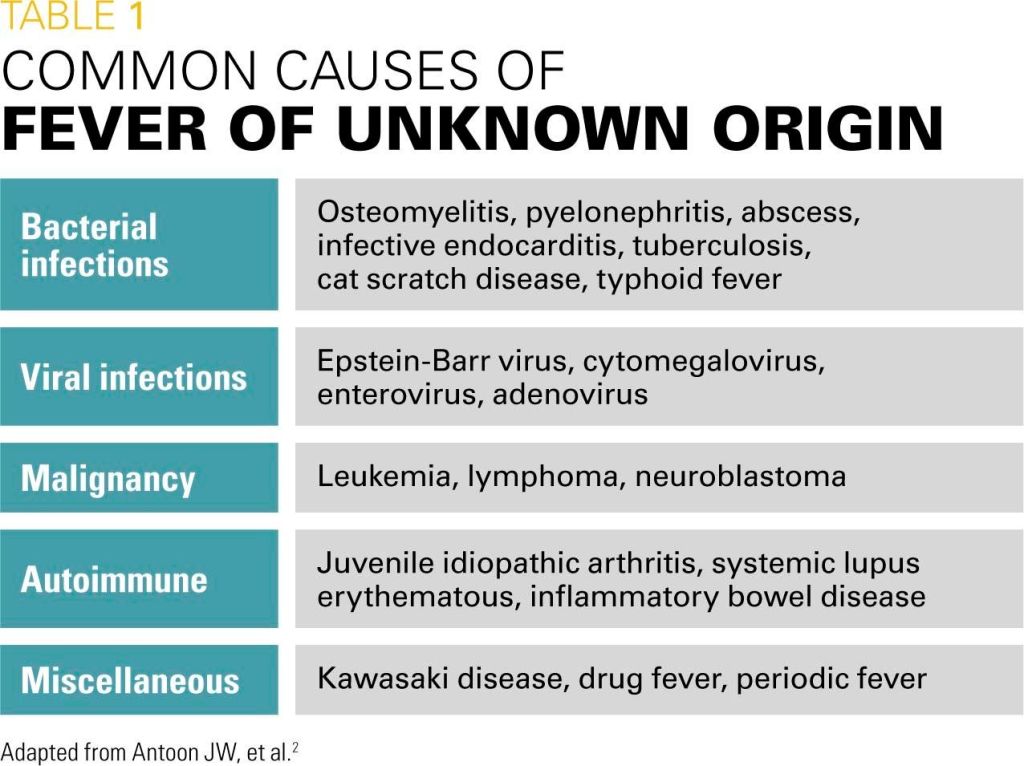
Fever is just one of the number of symptoms that accompany most infections such as Covid and influenza. When doctors can’t find a diagnosis for the fever, and it lasts for a few weeks, however, it is called fever of unknown origin, or FUO.
There are a bewildering number of illnesses that produce fever, and the mixture of these illnesses is different depending on geographic location, the type of hospital, and socioeconomic conditions.
Just like weight loss of unknown origin, or abdominal discomfort of unknown origin, fever without obvious cause is quite possibly be due to cancer in affluent America, and if you go in early you might have better outcomes with your treatment.
Fever has been known since earliest times, and was often considered a diagnosis on its own. In the past, the great majority of the fevers were infectious, and the outcome grave. In the mid 20th century, when I went to medical school, fevers were still mostly infectious. Antibiotics were the magic bullet, and were unfortunately overused. In underdeveloped countries, infections are still the most common cause, but in the developed world difficult to treat viral infections, autoimmune conditions, and cancer have been gaining in prominence.
When fever becomes excessive, and medication is needed, NSAIDS may be used, and works better on fever from infection than on fever from cancer. The take-home message for me is that if you use Naprosyn for a persistent fever, and isn’t effective, you might notify the doctor.
The motivation for me writing this article came from a very good posting in the New England Journal of medicine. They used a little humor, stating that modern FUO might be called “fever of too many origins”, what with all the indwelling catheters, implanted medical devices, shunts and long hospital stays. There is a separate category made for fever acquired in the hospital.
In people with AIDS, the evaluation is different depending on whether or not they are on treatment.
Tuberculosis is still a very common cause of fever.
Drugs are becoming increasingly responsible for troublesome fevers. In the early days of antibacterial therapy, sulfa was the only drug available, frequently caused fever. Now, sulfa is less used, and the penicillin derivatives are more common causes of fever.
If you have a fever, and have been traveling recently, be sure to tell the doctor. Your fever might be due to a tropical parasite such as malaria, particularly if you’ve been to West Africa.
Fever is an evolutionarily conserved body defense reaction and helps a person recover from an infection. The normal body temperature cycles according to the time of day; it is lowest first thing in the morning, and is higher later in the afternoon. The average body temperature used to be 37°C, or 98.6 F., but has been declining in recent decades, and is now about 36.5°C or 97.6°F. The use of electronic thermometers has cut down the amount of time needed to assess the body temperature, but added variability. I still prefer the old-fashioned thermometer.
Taking your temperature by whatever means you have available still remains a good idea when you don’t feel well.
—Dr. C.
Empowering Patients Through Education And Telemedicine






 Mayo Clinic – Pneumonia can range in seriousness from mild to life-threatening. It is most serious for infants and young children, people older than age 65, and people with health problems or weakened immune systems.
Mayo Clinic – Pneumonia can range in seriousness from mild to life-threatening. It is most serious for infants and young children, people older than age 65, and people with health problems or weakened immune systems.