The study investigated airway mucus and mucins in COVID-19 autopsy lungs and showed that both were elevated due to infection, especially during subacute and chronic stages of the disease.
Read more here: https://www.atsjournals.org/doi/10.11…

The study investigated airway mucus and mucins in COVID-19 autopsy lungs and showed that both were elevated due to infection, especially during subacute and chronic stages of the disease.
Read more here: https://www.atsjournals.org/doi/10.11…
Even mild COVID-19 is at least correlated with a startlingly wide spectrum of seemingly every illness. We need a much better taxonomy to address people’s suffering.

From The Atlantic, October 5, 2022:
The cases of long covid that turn up in news reports, the medical literature, and in the offices of doctors like me fall into a few rough (and sometimes overlapping) categories. The first seems most readily explainable: the combination of organ damage, often profound physical debilitation, and poor mental health inflicted by severe pneumonia and resultant critical illness.
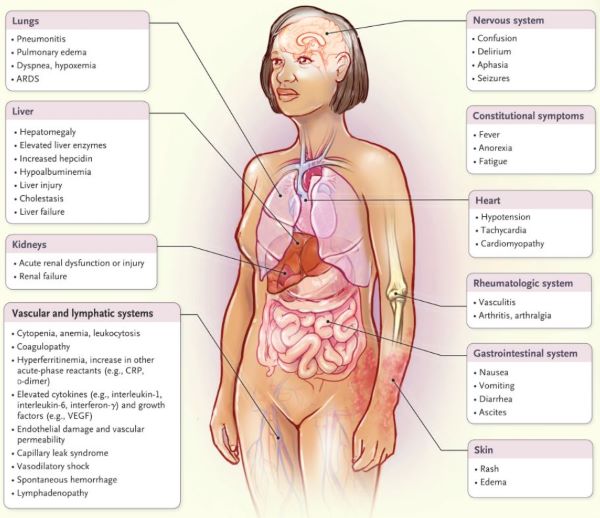
This serious long-term COVID-19 complication gets relatively little media attention despite its severity. The coronavirus can cause acute respiratory distress syndrome, the gravest form of pneumonia, which can in turn provoke a spiral of inflammation and injury that can end up taking down virtually every organ. I have seen many such complications in the ICU: failing hearts, collapsed lungs, failed kidneys, brain hemorrhages, limbs cut off from blood flow, and more. More than 7 million COVID-19 hospitalizations occurred in the United States before the Omicron wave, suggesting that millions could be left with damaged lungs or complications of critical illness. Whether these patients’ needs for care and rehabilitation are being adequately (and equitably) met is unclear: Ensuring that they are is an urgent priority.
The true disability cost of the COVID-19 pandemic is still unknown, but more and more studies are adding to the list of potential fallout from even mild COVID 19 infection.
In this episode of Coronapod we discuss a massive association study which links COVID-19 cases with an increase in the risk of developing type 2 diabetes. We delve into the numbers to ask how big the risk might be? Whether any casual relationship can be drawn from this association? And what might be in store from future research into COVID and chronic disease?
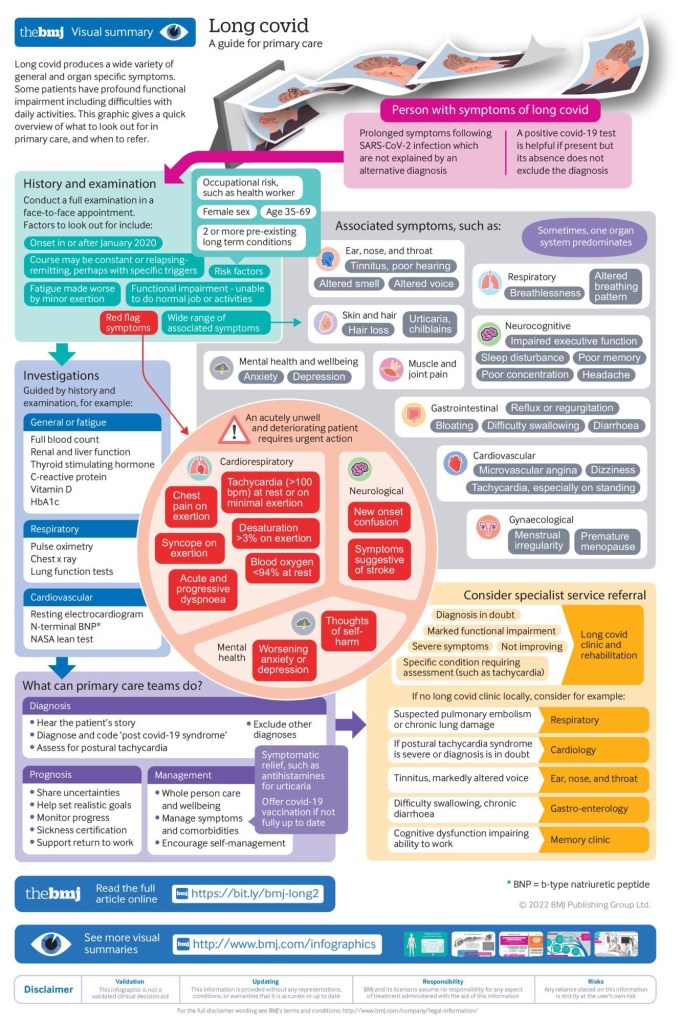
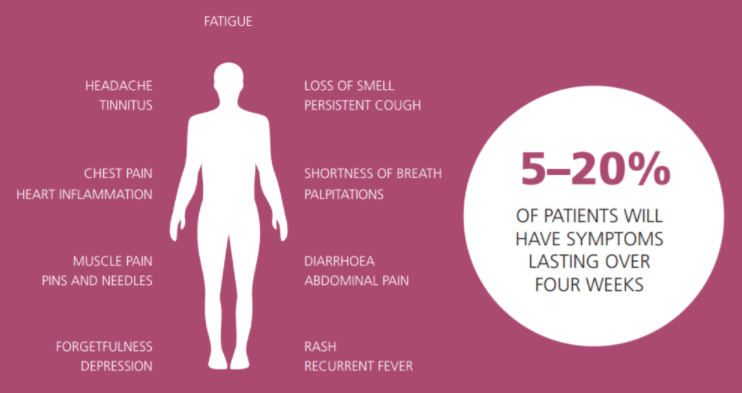
The risk of COVID-19 has been largely communicated only in terms of deaths and hospital capacity, with recovery and survival conflated with each other. Around one in three people with symptomatic COVID-19 still experience symptoms 12 weeks after onset (1). Long Covid can be experienced by all age groups and not only those with acute severe disease. The debilitating symptoms are wide-ranging, multisystemic, and predominantly fluctuating or relapsing. There is still much to understand about Long Covid, but what is not well understood should not be ignored.
Long Covid is likely the first illness in history that has been defined by patients through social media platforms such as Twitter and Facebook. People with Long Covid formed a movement that demanded recognition of what was happening to them. During the first wave of the pandemic in 2020, online testimonials of prolonged symptoms following severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection were the only source of reassurance to others with a similar experience, including this author (2). In the absence of any guidance or recognition about the possibility of a persistent illness, peer support is all that people with Long Covid had. Many previously healthy and active people described persistent symptoms of the acute illness that fluctuated, with new symptoms appearing weeks later. In many countries, most nonhospitalized people did not have lab confirmation of SARS-CoV-2 infection owing to lack of access to community testing, so their symptoms remained without a diagnosis.
By summer 2020, thousands were joining social media support groups. A common theme started to emerge: lack of recognition by the medical profession. Patients, including doctors, with Long Covid were consulting their health care providers, and their symptoms were commonly minimized, dismissed, or labeled as anxiety (3). A narrative emerged of people struggling to make sense of their symptoms and forming their own groups to understand and research what was happening to them in an international citizen science movement (4). The testimonials of people living with Long Covid demonstrated themes of stigma and discrimination.
COVID-19 is admittedly a pandemic and has caused much economic and social disruption in the world. Now we learn that it may not be over after a few of weeks of illness. LONG COVID is now an accepted syndrome.
You can tell because of the many clinics for handling it being set up by the NHS in England, and millions in research money being directed towards a solution.
The most disturbing thing to me is that infected but asymptomatic or mildly ill people may get this condition, and have one or more symptoms for a long time .Certainly, those more seriously ill develop long Covid symptoms more commonly.
Long Covid is taking its place with chronic fatigue syndrome, posttraumatic stress disorder and post ICU syndrome as poorly understood conditions. They may in fact be taking place simultaneously, even if they are not identical.
The cause can be due to continuing viral infection in older or immune compromised individuals. Vascular damage is another reason that could account for the widespread involvement of practically any organ system that doesn’t go away after a few weeks.
Structural damage to the alveoli of the lungs and other organs can also play a role, which would account for shortness of breath as a prominent persistent symptom. Although it has not been highlighted in the articles that I have read, auto immunity can also be playing a role in long Covid.
This would go along with The myocarditis rarely caused by the mRNA vaccines; perhaps some of the protein sequences of the spike proteins have similar shapes to some human tissues. Name a symptom, and you’ll probably find it listed among the 50 odd symptoms mentioned in the Wikipedia article on long Covid, which is appended to the end of this article.
The most prominent symptoms include extreme fatigue, mental fog, and shortness of breath. Treatment is mainly supportive and general. After ruminating on this condition, it’s going to be quite a while before Yours truly wants to breathe in other peoples air spaces; I plan to continue masking in public, distancing and avoiding large groups.
That being said, I am planning to go out to eat dinner tonight, and can hopefully be placed at the edge of the room. I will inquire as to the vaccination status of our waiter. The people at my table will all be doubly vaccinated, which is not complete assurance of safety, but will help make me feel relatively comfortable.
I also plan on getting a booster shot as soon as it is available. Hopefully, the vaccine incorporating the special mutations of the delta virus will be soon available. You don’t want to be infected by this nasty, promethian shape-shifter. Take care.
Read more

COMMENTARY
COVID 19 is a nasty disease, in case you hadn’t noticed. It is SNEAKY: you can catch it from a person who has no symptoms.
It is UNPREDICTABLE: you may develop no symptoms or Die from it. It can affect any part of your body, including HEART and BRAIN.
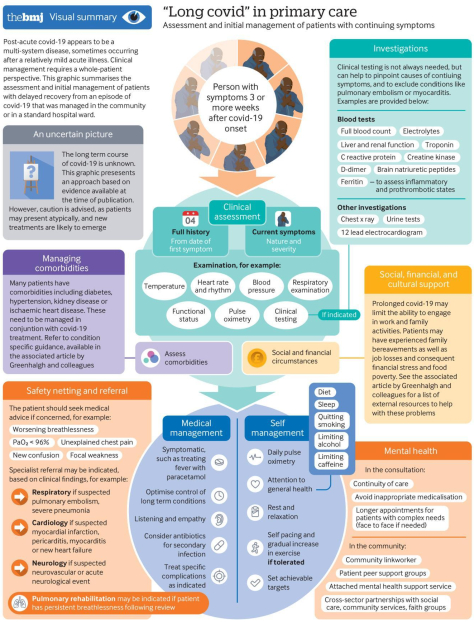
And now we hear that it can DRAG ON. The outstanding infographic, “a multi-systems disease, which is intended for PRIMARY CARE PROVIDERS, has a lot to offer patients, who can do a lot to Care for themselves:
You should also RESTRICT Alcohol, Caffeine and it goes without saying CIGARETTE SMOKING. Of course PREVENTION, with DISTANCING, MASKING and being Outside, coupled with SLEEP, DIET and EXERCISE is always best.