Globally, more people die from cardiovascular disease every year than from any other cause. Read more.

Globally, more people die from cardiovascular disease every year than from any other cause. Read more.
May 16, 2023: Patients have many questions about how to lower cholesterol and what to do after a high cholesterol diagnosis.
Dr. Ashish Sarraju answers some of these common questions including why fasting before your test is important, what all of the different tests tell your doctor and what you can do to help your heart.

Care of patients with aortic diseases remains highly complex and requires the combined expertise of a multidisciplinary team of cardiovascular surgeons, neurologists, cardiac anesthesiologists, vascular surgeons, and specialized advanced practice providers.
April 4, 2023: Peripheral Artery Disease (PAD) is a chronic circulatory condition, which, if not treated, can lead to limb amputations. PAD affects nearly 20 million Americans. An estimated 200,000 people, disproportionately from minority communities, suffer avoidable amputations every year.
Peripheral artery disease (PAD) is plaque buildup in your leg arteries. Your leg arteries carry oxygen and nutrient-rich blood from your heart to your arms and legs. Other names for this are peripheral vascular disease or peripheral arterial disease.
Shaped like hollow tubes, arteries have a smooth lining that prevents blood from clotting and promotes steady blood flow. When you have peripheral artery disease, plaque (made of fat, cholesterol and other substances) forms gradually inside your artery walls. Slowly, this narrows your arteries. This plaque is also known as atherosclerosis.
Many plaque deposits are hard on the outside and soft on the inside. The hard surface can crack or tear, allowing platelets (disc-shaped particles in your blood that help it clot) to come to the area. Blood clots can form around the plaque, making your artery even narrower.
If plaque or a blood clot narrows or blocks your arteries, blood can’t get through to nourish organs and other tissues. This causes damage ― and eventually death (gangrene) ― to the tissues below the blockage. This happens most often in your toes and feet.
PAD can get worse faster in some people more than others. Many other factors matter, including where in your body the plaque forms and your overall health.
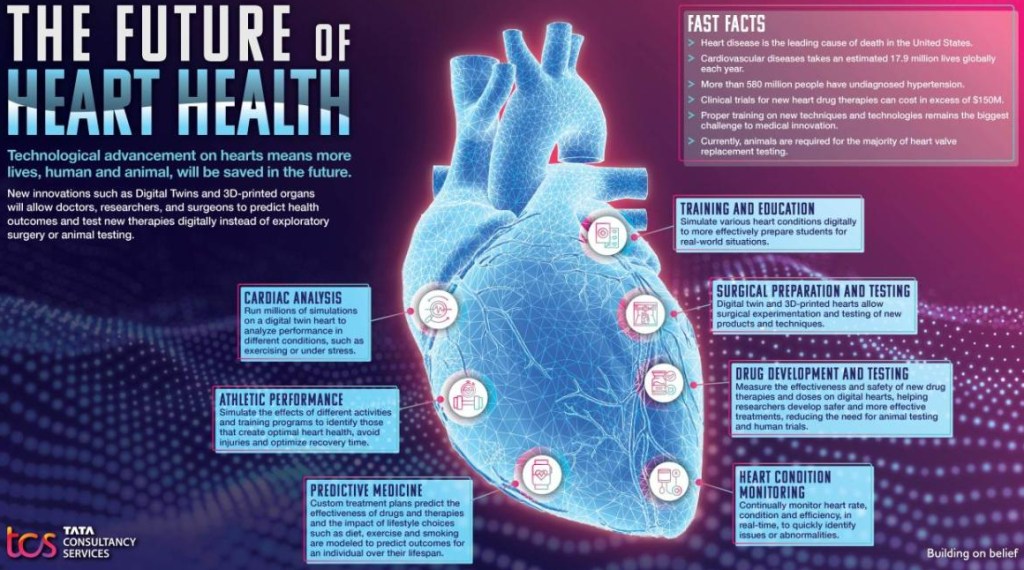
After a digital twin of a heart is created, researchers can go a step further and use 3D printing to create a physical version of a heart. This is then used to practice surgical techniques and test solutions such as new heart valves or drugs without ever touching an actual body.
March 2, 2023: Following National Heart Health Month in February, TCS futurists took a look at how a digital twin of the heart can save more lives – human and animal – in the future. From boosting athletic performance to developing predictive medicine, new advances in technology will help keep hearts healthier than ever.
TCS is on the leading edge of “Digital BioTwin” research, modeling human organs digitally to find new ways for researchers and doctors to test experimental drugs and surgical techniques without risk. With heart disease the leading cause of death in the U.S., it is more important than ever to innovate techniques to keep hearts healthy.
Using information from a MRI of someone’s heart, TCS can create a fully modeled human heart in cyberspace. By applying various historical and speculative data sets, doctors can see the impact of different conditions and situations such as beginning a long-term exercise program or quitting smoking. This approach to predictive medicine demonstrates the real impact of health choices to patients.
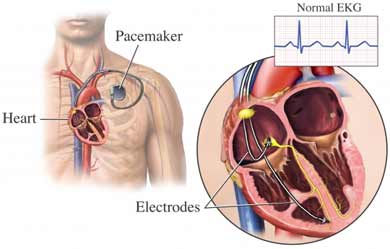
“The likelihood of needing a pacemaker increases with age,” says Dr. Sunil Kapur, a cardiologist at the Heart and Vascular Center at Harvard-affiliated Brigham and Women’s Hospital. “The good news is that today’s pacemakers have evolved from fixing irregular heartbeats to helping the heart maintain its normal function, which allows many men with certain heart conditions to stay active longer.”

A pacemaker monitors the heart’s rhythm and, when necessary, generates a painless electrical impulse that triggers a heartbeat.
The most common use for a pacemaker is when the heart beats too slowly or pauses, which triggers dizziness, shortness of breath, or fainting. (You should see your doctor immediately if you have any of these symptoms.) A pacemaker also can help your heart chambers beat in sync and improve blood flow if your heart isn’t pumping enough blood. In some cases, a pacemaker may be needed to treat a heartbeat that is too fast or irregular.
These issues can stem from problems with the heart’s electrical signaling, a heart defect, an enlarged or thick heart muscle, heart failure, or a heart attack.
Several tests can help your doctor determine if you need a pacemaker: an electrocardiogram, which measures the heart’s electrical activity; Holter monitoring, in which you wear a small device to track your heart’s rhythm; or an echocardiogram, which uses sound waves to produce images showing your heart’s size, structure, and motion.
The American Heart Association (AHA) recently revised its checklist for achieving optimal heart health, introducing its new Life’s Essential 8. The list replaces the AHA’s decade-old Life’s Simple 7.
Sleep health is the new addition to the cardiovascular health scoring tool, which now advises that adults get seven to nine hours per night. The organization updated four of the categories:
In this instructional video, Drs. Jane Leopold, Elliott Antman, William Sauer, and Paul Zei provide an overview of the classification and diagnosis of atrial fibrillation, management strategies, and mitigation of stroke risk with anticoagulation therapy.
Video timeline: 0:00 Pathophysiology and Symptoms 3:11 Stroke Risk, Anticoagulants, and Arrhythmia Control 6:32 Catheter Ablation 10:11 Post-Procedural Monitoring and Care
The video also focuses on the new rhythm-control strategy of catheter ablation therapy, with attention to the success rate, potential complications, postprocedural monitoring for recurrence of atrial fibrillation, and consideration of ongoing anticoagulation therapy in these patients. The New England Journal of Medicine is the world’s leading general medical journal.
Continuously published for over 200 years, the Journal publishes peer-reviewed research along with interactive clinical content for physicians, educators, and the global medical community at https://NEJM.org.
COMMENTARY:
This is a very good video well worth watching by general physicians and interested patients. There are several general and some specific comments I would like to make.
First, in my opinion, the best physician is none too good. In any operative or serious procedure, the decision to operate should be made by the patient in conjunction with a physician that does not do the operating. In my case, as a physician, I consulted an electrophysiologist.
Second, in my opinion, a good medicine is better than surgery. For atrial fibrillation, there has been no new medication treatment for decades. The main drugs are still amiodarone and Propafenone. The latter is less consistently effective, but has a better long-term safety profile; amiodarone often produces ‘floaters” in the eye, and Propafenone merely a bitter taste which you’ll get used to.
Third, it must be realized that catheter ablation is often not curative, especially as you get older, which was rather glossed over in this video. Ablation also requires a great deal of expensive equipment, which is constantly evolving, hence the importance of getting your ablation at a major center where it is done all the time. These major centers have less complications such as atrial wall perforation; Yes, you can rarely wind up worse off after any operation.
I am a physician, currently 90 years old. I developed atrial fibrillation of the persistent type when I was in my late 70s. I had a cardioversion to get me into sinus rhythm, and then tried Propafenone, which kept me in sinus rhythm for less than a month. My main motivation to get a radio frequency ablation was to stay off of anticoagulants. I had my ablation, and remained in sinus rhythm, and off anticoagulants, for three years. I could always tell when I went into atrial fibrillation from normal sinus rhythm because I produced a lot of urine and had to go to the bathroom all the time; atrial fibrillation causes release of a hormone called atrial naturetic peptide. I could also tell by taking my own pulse, which was quite irregular in comparison to my very regular sinus rhythm pulse, which ticked along with a rate in the high 50s. I had always thought my rate was low because I exercise a lot. Actually, my EKG shows a second-degree heart block which is probably partially responsible.
After three years, I returned to atrial fibrillation, and needed a another ablation. They found very few areas of abnormal electrical activity, and gave me a “touchup”, which lasted another two or three years after which I went back into atrial fibrillation. Probably as a result of my age, a fibrillated at a slow rate, and at least did not need any extra medication for rate control, although I did, of course, need to take a regular anticoagulant, in my case Eliquis.
In summary, atrial fibrillation is a common electrical storm in the upper chambers of the heart, causing a rapid, irregular beat. AF increases in frequency as you get older. In the video they mention the “substrate”, which is the structure of the atrium. In my own case, this was an enlarged atrium, and probably a tendency towards atrial fibrillation; my brother also has AF. The main complication is stagnation of blood in the atria, resulting in increased tendency toward stroke. Fibrillation therefore requires an anticoagulant.
There is some discussion about the irregular rate causing an inefficiency of cardiac action, contributing to heart failure, This is logical, but not clear cut statistically.
—Dr. C.
Cardiomyopathy is a disease of the heart muscle that makes it harder for the heart to pump blood to the rest of the body. Cardiomyopathy can lead to heart failure.

The main types of cardiomyopathy include dilated, hypertrophic and restrictive cardiomyopathy. Treatment — which might include medications, surgically implanted devices, heart surgery or, in severe cases, a heart transplant — depends on the type of cardiomyopathy and how serious it is.
There might be no signs or symptoms in the early stages of cardiomyopathy. But as the condition advances, signs and symptoms usually appear, including:
Signs and symptoms tend to get worse unless treated. In some people, the condition worsens quickly; in others, it might not worsen for a long time.