NEJM Group (May 25, 2023) – Glucocorticoids can help mitigate the adverse consequences of pneumonia, but whether they can reduce mortality in severe community-acquired pneumonia is unknown. New research findings are summarized in a short video.
CONCLUSIONS
Among patients with severe community-acquired pneumonia being treated in the ICU, those who received hydrocortisone had a lower risk of death by day 28 than those who received placebo.
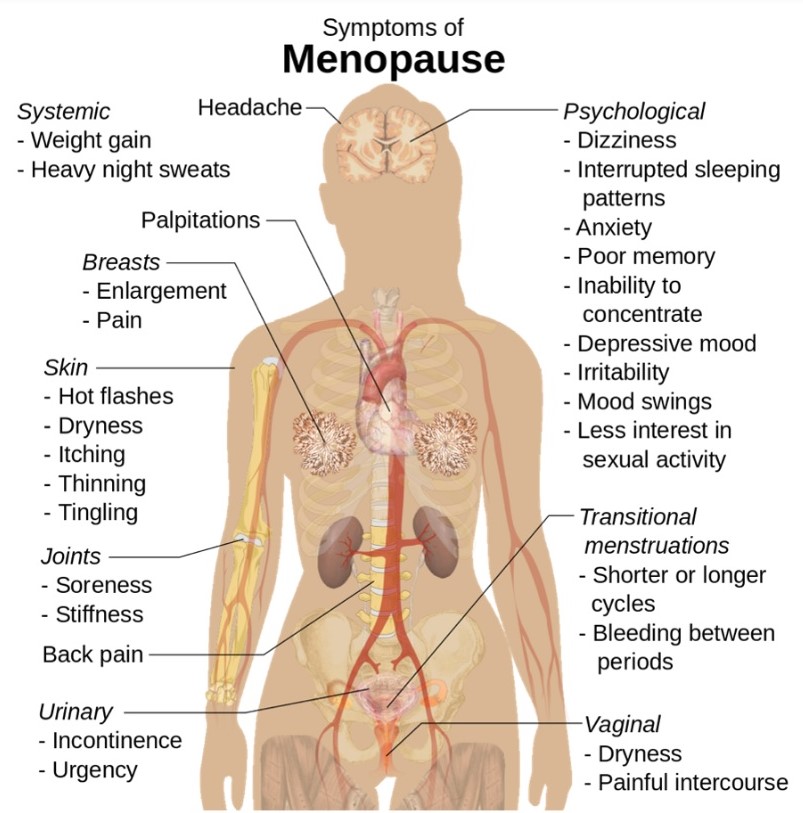
As levels of estrogen, a crucial chemical messenger, trend downward, women are at higher risk for severe depressive symptoms. Bone loss accelerates. In women who have a genetic risk for Alzheimer’s disease, the first plaques are thought to form in the brain during this period.
February 4, 2023
About 85 percent of women experience menopausal symptoms. Rebecca Thurston, a professor of psychiatry at the University of Pittsburgh who studies menopause, believes that, in general, menopausal women have been underserved — an oversight that she considers one of the great blind spots of medicine. “It suggests that we have a high cultural tolerance for women’s suffering,” Thurston says. “It’s not regarded as important.”
Even hormone therapy, the single best option that is available to women, has a history that reflects the medical culture’s challenges in keeping up with science; it also represents a lost opportunity to improve women’s lives.
The New York Times, Sunday magazine, posted an article by Susan Dominus entitled “the vicious cycle”, in which was a long discussion of the disease burden of menopause. It is well worth reading.
“Forever Feminine” was a book by Robert Wilson, in 1966, which promoted hormone treatment for “enjoyment of sex” in menopausal women. The use of estrogen skyrocketed.
Alarming research in 1975, which linked estrogen usage to endometrial cancer, halted the rise of the drug’s popularity.
Without hormonal treatment, the many symptoms of menopause were devalued and quietly suffered by women.
The medical profession has been slowly recovering from whiplash. New, better controlled research is being done and slowly a more nuanced approach is being taken. Women with a history of heart attack or stroke are still generally advised against hormonal therapy, but many others are being given birth control pills, which is a combination of estrogen and progesterone.
The average age of menopause is approximately 50 years of age, but symptoms can anticipate menopause by several years. An elevated FSH is the usual laboratory test to indicate perimenopause.
Early menopause can be associated with a decreased lifespan, increased likelihood of osteoporosis, cardiovascular disease and dementia, and is often treated with hormonal therapy. A delayed menopause is less likely to be treated with hormonal therapy, because of increased risk.
There are a lot of risk factors to be balanced against the symptoms involved, such as hot flashes and the entire panoplay of symptoms indicated in the infographic.
Some day, artificial intelligence will be used in order to make more explicit the benefits and risks involved. Until that time, the patient suffering from premenopausal or menopausal symptoms should find a Doctor Who would actually listen to her, a difficult task these days.
Hearing aids are not one-size-fits all. “While OTC devices may help many people with mild or moderate hearing loss, they might not be appropriate for all types of hearing loss,” says Dr. Naples.
Harvard Health Publishing – A change in FDA regulations has cleared the way for over-the-counter (OTC) hearing aids. What does this mean for you if you’re among the approximately 48 million Americans with some degree of hearing loss? We asked Dr. James Naples, assistant professor of otolaryngology/head and neck surgery at Harvard-affiliated Beth Israel Deaconess Medical Center, to help explain potential pros and cons.
The basics: Hearing aids versus amplification products
There are various types of hearing aids that largely work in the same way. Whether the style is behind the ear or in the ear canal, they amplify sounds to make them louder. They also help filter out certain types of noise. “All hearing aids use a combination of signal processing and directional microphones to filter out some unwanted noise and to improve our ability to hear sounds,” says Dr. Naples.
Don’t confuse prescription or OTC hearing aids with personal sound amplification products (PSAPs) sold at most drug stores. Such products merely amplify nearby sounds. They’re not tailored to an individual’s hearing loss, and aren’t regulated by the FDA or intended to treat hearing loss.
Humans and their mammalian cousins have lost the ability to regenerate the hair cells in the inner ear. In preindustrial society(how could they know?) people apparently didn’t lose hearing as they aged. However, in the Industrial Age, the prevalence of noise has been increasing along with our power consumption, and loss of hearing consequently occurs along with Aging.
High frequency loss is the most prominent, and this leads to inability to hear consonants, and have more difficulty with the voices of children and women which tend to be of a higher frequency. The ability of young people to hear high frequencies better than older people has led to various ringtones and songs favoring high frequencies, which the children can hear and older people cannot.
There are a number of things that can add to this hearing loss, such as chronic exposure to loud sounds (such as rock concerts), exposure to drugs that damage hearing, such as certain antibiotics and even aspirin. Otosclerosis and repeated middle ear infections can also accentuate the problem by interfering with sound conduction.
Ringing in the ears, tinnitus, is also associated with accelerated hearing loss.
I have had tinnitus for a long time, and at the age of 90, I have definite hearing loss. Even a couple of decades ago my high frequency loss was quite demonstrable by audiogram. I am resisting the temptation to get it corrected, since the louder sounds from the device would probably gradually reduce my baseline hearing ability. Also I am now forced to pay strict attention when listening to people. This may slow down the tendency of older people to have a greater difficulty in “decoding” the spoken word, due to decreased brain processing.
With the passage of a new law permitting people to access hearing aids without a prescription, the price of hearing aids is bound to go down, another reason for waiting.
If you are considering getting a hearing aid, an audiologist would prepare one that is tuned to your specific hearing loss.
In this instructional video, Drs. Jane Leopold, Elliott Antman, William Sauer, and Paul Zei provide an overview of the classification and diagnosis of atrial fibrillation, management strategies, and mitigation of stroke risk with anticoagulation therapy.
Video timeline:0:00 Pathophysiology and Symptoms 3:11 Stroke Risk, Anticoagulants, and Arrhythmia Control 6:32 Catheter Ablation 10:11 Post-Procedural Monitoring and Care
The video also focuses on the new rhythm-control strategy of catheter ablation therapy, with attention to the success rate, potential complications, postprocedural monitoring for recurrence of atrial fibrillation, and consideration of ongoing anticoagulation therapy in these patients. The New England Journal of Medicine is the world’s leading general medical journal.
Continuously published for over 200 years, the Journal publishes peer-reviewed research along with interactive clinical content for physicians, educators, and the global medical community at https://NEJM.org.
COMMENTARY:
This is a very good video well worth watching by general physicians and interested patients. There are several general and some specific comments I would like to make.
First, in my opinion, the best physician is none too good. In any operative or serious procedure, the decision to operate should be made by the patient in conjunction with a physician that does not do the operating. In my case, as a physician, I consulted an electrophysiologist.
Second, in my opinion, a good medicine is better than surgery. For atrial fibrillation, there has been no new medication treatment for decades. The main drugs are still amiodarone and Propafenone. The latter is less consistently effective, but has a better long-term safety profile; amiodarone often produces ‘floaters” in the eye, and Propafenone merely a bitter taste which you’ll get used to.
Third, it must be realized that catheter ablation is often not curative, especially as you get older, which was rather glossed over in this video. Ablation also requires a great deal of expensive equipment, which is constantly evolving, hence the importance of getting your ablation at a major center where it is done all the time. These major centers have less complications such as atrial wall perforation; Yes, you can rarely wind up worse off after any operation.
I am a physician, currently 90 years old. I developed atrial fibrillation of the persistent type when I was in my late 70s. I had a cardioversion to get me into sinus rhythm, and then tried Propafenone, which kept me in sinus rhythm for less than a month. My main motivation to get a radio frequency ablation was to stay off of anticoagulants. I had my ablation, and remained in sinus rhythm, and off anticoagulants, for three years. I could always tell when I went into atrial fibrillation from normal sinus rhythm because I produced a lot of urine and had to go to the bathroom all the time; atrial fibrillation causes release of a hormone called atrial naturetic peptide. I could also tell by taking my own pulse, which was quite irregular in comparison to my very regular sinus rhythm pulse, which ticked along with a rate in the high 50s. I had always thought my rate was low because I exercise a lot. Actually, my EKG shows a second-degree heart block which is probably partially responsible.
After three years, I returned to atrial fibrillation, and needed a another ablation. They found very few areas of abnormal electrical activity, and gave me a “touchup”, which lasted another two or three years after which I went back into atrial fibrillation. Probably as a result of my age, a fibrillated at a slow rate, and at least did not need any extra medication for rate control, although I did, of course, need to take a regular anticoagulant, in my case Eliquis.
In summary, atrial fibrillation is a common electrical storm in the upper chambers of the heart, causing a rapid, irregular beat. AF increases in frequency as you get older. In the video they mention the “substrate”, which is the structure of the atrium. In my own case, this was an enlarged atrium, and probably a tendency towards atrial fibrillation; my brother also has AF. The main complication is stagnation of blood in the atria, resulting in increased tendency toward stroke. Fibrillation therefore requires an anticoagulant.
There is some discussion about the irregular rate causing an inefficiency of cardiac action, contributing to heart failure, This is logical, but not clear cut statistically.
Learning about hypertension can be intimidating. Leslie Thomas M.D., a nephrologist at Mayo Clinic, walks you through the facts, the questions, and the answers to help you better understand this condition.
Video timeline: 0:00 Introduction 0:39 What is hypertension? 1:13 Who gets hypertension? / Risk factors 2:18 Symptoms of hypertension 2:36 How is hypertension diagnosed? 3:14 Treatment options 3:51 Coping methods/ What now? 4:05 Ending
COMMENTARY:
Hypertension is an elevation of the blood pressure in the arteries. It is measured conventionally by blood pressure cuffs, although a catheter in the artery is more accurate. I’ve had my blood pressure taken countless numbers of times by nurses and doctors who sometimes put the cuff on my arm through a piece of clothing, making it less accurate. Sometimes it is taken by an automatic blood pressure cuff even in the doctors office. The automated cuff can be purchased for $20 or less for you to use it at home, but it’s accuracy is questionable when you have an irregular heartbeat with atrial fibrillation such as I do.
The blood pressure reading which is considered to be normal Is dropping. In the present video, following 2017 guidelines , they state that a systolic reading of more than 120 mmHg is elevated, and anything more than 130 is hypertension. It may be true that studies have been done to show that these slight elevations cause problems, but so can the drugs that are used to lower blood pressure; a cough can be caused by ACE inhibitors. Fatigue and fainting can be caused by an excessive dosage of any blood pressure medication.
Healthy diet, especially avoiding extra salt, Regular exercise and good sleep will go a long way towards keeping your blood pressure at 120 or below on the high reading (systolic), and 80 on the low reading (diastolic).
My systolic blood pressure varies between 120 and 140 systolic, and is usually around 60 diastolic. For a long time I thought the relatively low (diastolic) blood pressure was more important, since diastole is of greater duration than systole, but it has now been determined that the systolic blood pressure reading is the one to worry about. Calcification and lack of elasticities in the arteries as you get older can lead to higher systolic blood pressure.
It used to be thought that the normal systolic blood pressure was 100+ your age in years. Those days are gone, however, and greater life expectancy and health Is one result of carefully monitoring your blood pressure, and working hard to keep it down.
Please refer to the Mayo Clinic article to give you (much) more information.
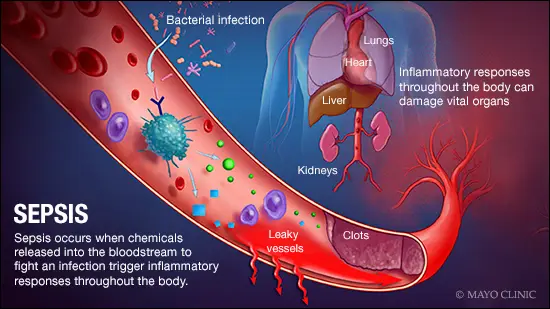
Sepsis occurs when the body’s response to an infection damages its own tissues. When these infection-fighting processes turn on the body, they cause organs to function poorly and abnormally.
As sepsis worsens, blood flow to vital organs, such as your brain, heart and kidneys, becomes impaired. Sepsis may cause abnormal blood clotting that results in small clots or burst blood vessels that damage or destroy tissues. If sepsis progresses to septic shock, blood pressure drops dramatically, which can lead to death.
Nearly 270,000 people in the U.S. die each year as a result of sepsis, and one-third of people who die in a hospital have sepsis, according to the Centers for Disease Control and Prevention.
Signs of sepsis
To be diagnosed with sepsis, you must have a probable or confirmed infection, and all of these signs:
Change in mental status.
Systolic blood pressure — the top number in a blood pressure reading — less than or equal to 100 millimeters of mercury, or mm Hg.
Respiratory rate higher than or equal to 22 breaths per minute.
Signs of progression to septic shock include:
The need for medication to maintain systolic blood pressure greater than or equal to 65 mm Hg.
High levels of lactic acid in your blood, which means that your cells aren’t using oxygen properly.
Treatment
Early, aggressive treatment increases the likelihood of recovery.
A number of medications are used to treat sepsis and septic shock, including antibiotics, corticosteroids, painkillers and sedatives. Supportive care, including oxygen and dialysis, and surgery to remove the source of the infection, also may be needed.
People who have sepsis require close monitoring and treatment in a hospital ICU. Lifesaving measures may be needed to stabilize breathing and heart function.
The hospital is a dangerous places to be, and the most common cause of death there is sepsis. Sepsis is an underappreciated killer, and it’s getting more common because people are aging, devices are more commonly implanted into the body, immunosuppressive treatment is being used more commonly, and hospital acquired infections are increasingly resistant to treatment.
Sepsis can be caused by an overwhelming infection with bacteria, but can also be caused by viruses, fungi, and severe trauma. Low blood pressure is a common problem, and is associated with change in mental status, and increased breathing rate in raising a red flag for sepsis. Endotoxins play an important, if confusing, role. Endotoxins derive from Gram negative bacteria, but the most common bacterium causing sepsis is the gram positive staphylococcus aureus. With sepsis, though,the gastrointestinal tract may become more leaky, and Gram negative organisms may thereby gain access to the blood stream.
A ccmmon test to detect sepsis is the serum lactate, which becomes elevated if oxygen utilization is diminished, such as in sepsis. There is also a direct test for endotoxin in the bloodstream, performed by using LAL, or Limulus amebocyte lysate. This substance, derived from the cells of the blood of the horseshoe crab, is very sensitive to endotoxins, and coagulates in its presence. This test is also used to detect endotoxins in Biological products and devices, making horseshoe crab is quite valuable.
Maintaining general health, keeping up on your immunizations, wishing your hands, keeping cuts and burns free from infection, ovoid smoking, controlling diabetes and avoiding hospitals whenever possible are useful preventative techniques.
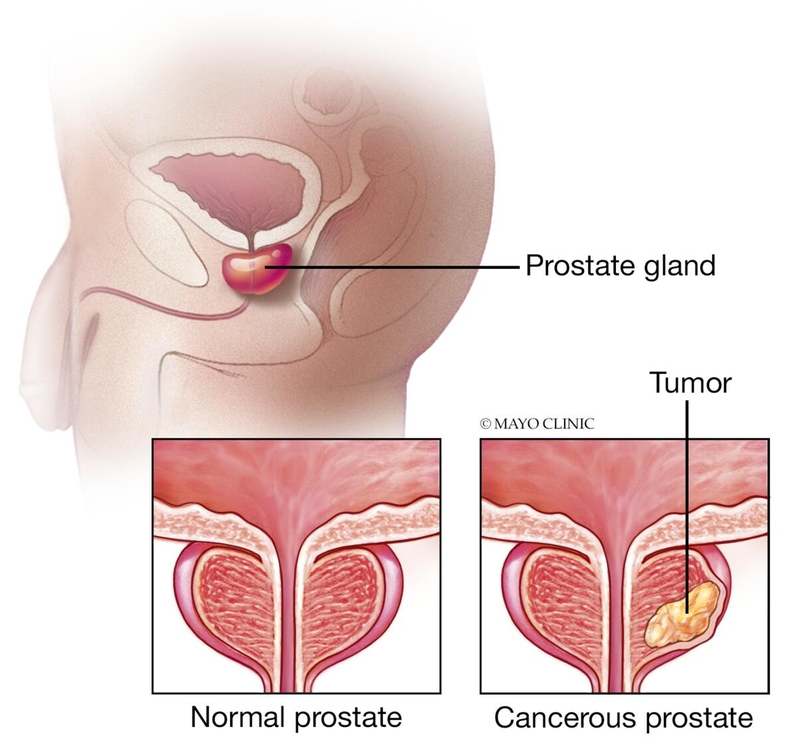
Prostate cancer is one of the most common types of cancer. Many prostate cancers grow slowly and are confined to the prostate gland, where they may not cause serious harm.
However, while some types of prostate cancer grow slowly and may need minimal or even no treatment, other types are aggressive and can spread quickly.
Prostate cancer that’s detected early — when it’s still confined to the prostate gland — has the best chance for successful treatment.
Prostate cancer may cause no signs or symptoms in its early stages. When it’s more advanced may cause signs and symptoms such as:
PSA screening will pick up prostate cancer very efficiently. However, it will also pick up slow growing cancer that might never be require treatment, and responding to the positive test could cause problems ranging from pain and convenience to erectile dysfunction and incontinence.
It takes 1000 men screened to produce one life-saving treatment for prostate cancer.
Risk reward analysis means that the younger you are, the more reasonable is a test, since you have many more years of potential life. The older you are, conversely, the less you have to gain. The problem is that most cancers are slow growing, and might never cause a problem, especially if you have only a few years left to live.
Most experts recommend a test when a man reaches the age of 45, but reserve annual testing for those who are at high risk, such as having a brother or father with aggressive prostate cancer.
When a man reaches the age of 70, most experts would decline to test.
Sometimes, emotional considerations present themselves; worry is very much a disease. For instance, the best man at my wedding stopped getting his PSA test about three years before he was diagnosed with fatal metastatic prostate cancer. I am inclined to continue getting my annual prostate test, and would worry if I didn’t.
A recent study in the journal Cancer reported that more than half of a group of men 75 years and older had PSA tests and biopsies.
As an interesting aside, the PSA test is the only test I have ever had rejected by Medicare, presumably because of this expert opinion factoring in the cost benefit analysis of using the test.
The vaccine, called Convidecia Air, changes the liquid form of the vaccine into an aerosol using a nebuilzer. The vaccine can then be inhaled through the mouth using the nebulizer machine. The needle-free vaccine “can effectively induce comprehensive immune protection in response to SARS-CoV-2 after just one breath,” Cansino said in a statement.
In July, Chinese scientists published a pre-print study showing that people who received one booster dose of Cansino’s inhaled vaccine after two doses of the inactivated jab from Chinese maker Sinovac developed more antibodies than people who received three Sinovac shots. Four weeks after receiving the inhaled booster, 92.5% of people had developed neutralizing antibodies for Omicron.
Those who got three doses on Sinovac’s jab did not demonstrate any neutralizing antibodies for Omicron, either four weeks or six months after getting a booster.
Spray vaccines will be our best chance to stop Covid.
However, there are two big problems that have to be solved.
The first problem is keeping up with the blitzkrieg mutation capacity that Covid has. Our best chance to do that is with the mRNA technology, which permits vaccine generation with minimal delay. However, mRNA vaccines are too fragile to be suitable for a nasal or oral spray. The particles would be destroyed before they could activate the mucosal immune system.
But it is still possible, using laboratory technology to convert this mRNA into peptides and proteins suitable for use as a spray. Using AI to generate three dimensional shapes, surely a stable molecule of suitable configuration and stability could be eventually generated.
The second appears to have been partially solved by the Chinese, according to the Fortune article, namely getting an injectable vaccine into a suitable form and dose to survive the bodies mucosal clearance mechanisms and enzymes, designed to keep foreign sprays and mists out of the body, in enough concentration to stimulate the mucosal immune system.
Our bodies have developed a parallel Defense system using a unique immunoglobulin, IGA, and special support cells. When stimulated, immunity bristles as a first line of defense to deny incoming viruses entrance to the body. This is what is needed to prevent infection from occurring in the first place, so extremely important for a highly infectious and potentially lethal virus such as Covid.
The Chinese, with their autocratic system, have a better chance of making everybody take this vaccine, even though it requires a cumbersome liquid nebulizer to generate the mist.
Better would be a handheld inhaler, and, hopefully, this is what some dozen pharmaceutical corporations, working on a nasal or inhaled vaccine , are aiming for.
Learning about insulin resistance, or prediabetes, can be intimidating. Eleanna De Filippis, M.D., Ph.D., an endocrinologist at Mayo Clinic, walks you through the facts, the questions, and the answers to help you better understand this condition.
Video timeline: 0:00 Introduction 0:41 What is insulin resistance? 1:32 Who gets insulin resistance? / Risk factors 2:38 Symptoms of insulin resistance 4:04 How is insulin resistance diagnosed? 4:34 Treatment options 5:21 Coping methods/ What now? 5:41 Ending
COMMENTARY:
The (developed) world just has too much food. Food producers race with each other to make It tastier, to advertise it widely, and make it available on demand. As a consequence of their success, at least 1/2 of the developed world is overweight and has decreased insulin sensitivity, prediabetes or diabetes. This leads to severe health consequences in the form of hypertension, arteriosclerosis, heart disease, brain disease, liver disease, and a variety of back and joint problems.
Mankind did not evolve in an environment of chronic nutritional oversupply, but rather it’s reverse. Mankind did not develop in a sedentary environment, but rather it’s reverse.
Insulin resistance is caused by overfilled energy stores (excess fat), increased inflammation from distended, dying fat cells, excess fatty acids and stresses to some of the important micro structures in our cells, such as mitochondria and endoplasmic reticulum, not to mention metabolic pathways such as the mTOR and Sirtuin systems.
Eating is a pleasure, and turning down food takes self-discipline, which is a pain, and is becoming increasingly unpopular. “Maybe a pill will come along to get rid of fat and prevent its accumulation”. but don’t count on it. The main hope for avoiding the danger of overnutrition is being discriminating about what and how much you eat.
Exercise is inconvenient and uncomfortable, but is the second necessity for a healthy life. Two of its many benefits is to increase adiponectin, which increases burning of the fatty acids which are so toxic to the body, and to increase insulin sensitivity, counteracting type two diabetes.
The third necessity is getting enough sleep.
Replay the old record. Diet, exercise and sleep, sleep diet and exercise.
Please excuse me, it’s time for my evening exercise.
Psoriasis is a skin disease that causes a rash with itchy, scaly patches, most commonly on the knees, elbows, trunk and scalp.
Psoriasis is a common, long-term (chronic) disease with no cure. It can be painful, interfere with sleep and make it hard to concentrate. The condition tends to go through cycles, flaring for a few weeks or months, then subsiding for a while. Common triggers in people with a genetic predisposition to psoriasis include infections, cuts or burns, and certain medications.
Treatments are available to help you manage symptoms. And you can try lifestyle habits and coping strategies to help you live better with psoriasis.
My practice was restricted to allergy, but I saw many patients with psoriasis. The red scaly patches made them think they had allergic dermatitis, eczema. Psoriasis on the arm is usually located on the elbow, and atopic dermatitis on the opposite side, in the flexural area. Thick, pitted fingernails are also common in psoriasis. It’s combination with arthritis is worrisome.
Psoriasis will usually develop first, and the psoriatic arthritis will follow years later, but 10% of the time the arthritis Is the first problem. This form of arthritis can be very painful, and cause deformities. It is often worse than rheumatoid arthritis, although does not affect as many joints, and is often asymmetrical. It inflames the area where tendons attach to the bone, which is one of the reasons that it can be more painful than rheumatoid arthritis.
Psoriasis is an autoimmune problem and can involve practically any organ in the body.
It is often associated with metabolic syndrome and diabetes.
Psoriatic arthritis does not have the rheumatoid serum markers that can help diagnose rheumatoid arthritis, and unless psoriasis is also present on the skin, it can be hard to diagnose.
Symptomatic treatment with NSAIDs, physical therapy, phototherapy and topical treatments can be helpful, but very expensive biologics are sometimes needed to help out methotrexate and other first line DMARDs (Disease modifying antirheumatic drugs).
This condition can be progressive. If you develop scaly red patches on your skin, be sure to check with the doctor about the possibility of psoriasis.
—Dr. C.
Empowering Patients Through Education And Telemedicine