“While the pandemic will prove the value of virtual care in a crisis, it will also demonstrate the effectiveness for ongoing chronic care management,” she said. “This moment will have a lasting effect on the adoption of virtual care and accelerate the shift from in-person care to virtual first engagement for multiple conditions and use cases.”
While the need for remote care will not be as acute once the pandemic crisis subsides, demand for telehealth systems will likely remain high. Forrester now expects more than one billion virtual care visits this year, the vast majority of them related to COVID-19.
“…After the crisis subsides, there will be a patient population that will want to continue to receive care online for some things, like managing chronic conditions, follow-up visits after an inpatient stay, surgery or to discuss diagnostic results,” she said.
In this case, it will be important for healthcare providers to ensure that patients are aware of the availability of services.
From a Stanford Medicine article (April 27, 2020):
“Far from separating us from our patients, it is actually expanding on what we can do,” said Ryan Ribeira, MD, clinical assistant professor of emergency medicine at the Stanford School.
An iPad in a patient room at Stanford Health Care’s emergency department. Photo by Susan Coppa
Caring for patients remotely greatly reduces the use of protective equipment — an estimated 80-120 sets per day. The risk of exposure has also been minimized for physicians, nurses and other caregivers, particularly those who are pregnant, immune-compromised or otherwise at high risk of complications from COVID-19.
When the staff at Stanford Health Care’s Marc and Laura Andreessen Emergency Department started connecting with patients in isolation via iPad, they found an unexpected benefit: The approach offered a more personal, human-centered experience.
The iPad project moved from conception to implementation in just eight days, starting with a drive-through program in a Stanford Health Care garage: Patients remained in their cars while a physician assessed them by video from inside the emergency department.
To bring the program into patient rooms, technology specialists at Stanford Health Care ensured the tablets had necessary features, such as the ability to auto-answer calls. When a caregiver calls to check in, the patient receives a few rings as advance notice, then the iPad answers itself.
The iPad has also been paired with portable handheld ultrasound scanners that quickly plug in, eliminating the need for a bulky ultrasound cart that requires decontamination after every use. And patients participating in clinical research can consent via iPad.
From an EndocrinologyAdvisor online article (April 27, 2020):
“In the diabetes world where data from meter, pump, and sensor downloads are critical to management, telemedicine is an ideal way to interact with patients. The missing pieces are vital signs, especially blood pressure and weight, but often the patient can monitor these at home and provide trends. Diabetes experts can manage the majority of patients using the HbA1c test and other data the patient has recorded and downloaded to a website. These are easily accessible. I have had patients write down their glucose readings and fax the results as well.” Mark H. Schutta, MD, medical director of the Penn Rodebaugh Diabetes Center
In perhaps one of the most significant changes to occur in health care as a result of the coronavirus disease 2019 (COVID-19) pandemic, telemedicine has suddenly reached the widespread adoption many proponents have championed for years. Recognizing the necessity of telemedicine in light of the current crisis — both to address increased treatment needs and to prevent unnecessary in-person contact — some payors and state legislators have loosened certain restrictions regarding its use across clinical specialties.
If screening tools and self-checkers do not lead you to the care or information you are seeking, you can reach out directly to your doctor or health insurance company for options that can help connect you to a provider online. Understanding telehealth
Whether you’re looking for health care related to COVID-19 or something else, find out more about how to prepare for the visit. Preparing for a video visit
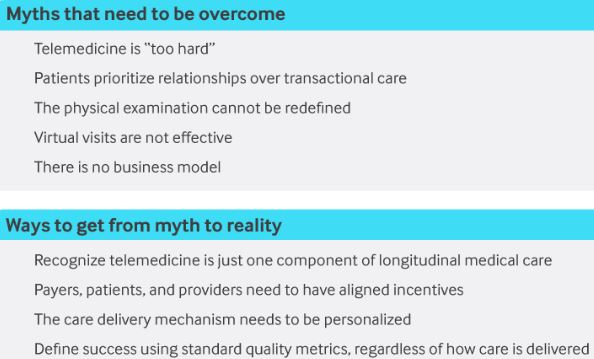
Until recently, there were several barriers preventing widespread adoption of telemedicine. The two broad themes were:
Providers, health systems, and payers were slow to embrace change
A failure to appreciate that telemedicine is not a new type of medicine, but rather simply a care delivery mechanism that can be utilized with some patients, some of the time, to provide high-quality care
Addressing the Telemedicine Myths
Myth 1: Telemedicine is “too hard.”
This was not true before Covid-19 and we have further demonstrated that it is not true now. Almost every provider and the great majority of patients in the U.S. already possess the technology needed to conduct a telemedicine visit — a smartphone, tablet, or computer.
It turns out that when fear of catching a potentially fatal disease strikes, telemedicine is no longer too hard.
Myth 2: Patients prioritize existing relationships with their provider over transactional episodic care.
Data argues otherwise: The majority of times, patients just want care. Falling primary care visits rates, coupled with growing emergency department and urgent care visit rates, suggests convenience as more important than an established relationship.
Myth 3. You cannot do a physical examination.
It turns out you can. A new 21st-century physical exam utilizing telemedicine emphasizes the importance of general appearance (sick or not sick, weight, distress), respiratory effort, and environmental factors including a visual assessment of the home that is not something that can be accomplished at an office visit.
The majority of times, patients just want care.
Myth 4: Virtual visits are less effective than in-person visits.
Focusing on the comparison in diagnostic accuracy between virtual and in-person visits sets up a false dichotomy. Focusing on actionable information is more important than diagnostic accuracy.2 Actionable information recognizes providers might not always make a diagnosis within a single visit, whether in-person or telemedicine.
Like every other new challenge, you have to try telemedicine to get comfortable with it.
Myth 5. There is not a payment model supporting telemedicine.
While it is true that the Centers for Medicare & Medicaid Services (pre-Covid-19) had limited reimbursement based upon site of service and geography, since the Covid-19 outbreak, to the credit of the federal government and commercial payers, telemedicine is now covered.
The BMJ’s new podcast aims to help doctors feel more connected, heard, and supported
“Deep breath in … and out. Again, deep breath in … and out.”
We tune in to patients’ breath sounds, seeking confirmation of a diagnosis—one more supporting piece of evidence to reassure anxious patients or to narrow the differential.
But since the SARS-CoV-2 pandemic arrived, saying “deep breath in” has been replaced by the need to take one ourselves: before looking at the morning news, before venturing out (or logging on) to work each morning, and before ringing the next patient on your list with the ominous note alongside their name: “fever and cough for a week, now feeling breathless.” Although chosen in what seems like a different era, the name for The BMJ’s new podcast for general practitioners—Deep Breath In—seems fitting for our troubled times.
Rebooting general practice
Before anyone in Wuhan fell ill, GPs had already been feeling the strain. In the UK, despite government promises of 5000 new practising GPs by 2020, there were 6.2% fewer full time equivalent GPs in 2019 than in 2015.1 Similarly, physicians in the US have been compensating for an estimated shortfall of some 14 500 primary care doctors since 2017.2 Recent attempts to take the strain off GPs in England by funding allied health professionals have faltered because of onerous new demands on fledgling primary care networks.3 Turning it off and switching it back on again is often the only thing that works when your computer grinds to a halt. Perhaps coronavirus will do the same for primary care.
Primary Care Physicians are a vanishing species [1]. This is unfortunate, since PCPs are the only doctors who attend the whole field of Medicine (have you ever asked an orthopedist about your cough?).
However, some of the slack is being taken up by Nurse Practitioners [2] and Physicians Assistants [3].
If you know a retired Internist or Family Practice Physician, be sure to cultivate a friendly relationship (and give them a hug when the Covid 19 epidemic cools off). They might be inclined to be that greatest of all Medical Resources- the Patient Advocate [4].
—Dr. C.
Empowering Patients Through Education And Telemedicine