

March 2023: In this episode of the Heart podcast, Digital Media Editor, Professor James Rudd, is joined by Dr Chris Wilkinson from Hull York Medical School and the James Cook hospital, UK. They discuss the concept of frailty and why it’s an important concept in cardiology.
Tag Archives: BMJ

Neurology: What Are Cluster Headaches? (BMJ)
The prevalence of cluster headache is about one in 500. In people coming to a headache clinic, the prevalence is about 10%.
Cluster headaches are excruciating and incapacitating, and affect quality of life. Prompt diagnosis and treatment can make a big difference to the outcome – so it is vital that we get the diagnosis and management of this condition right.
In this BMJ Best Practice podcast on cluster headache, Kieran Walsh talks with Professor Amaal Starling, Associate Professor of Neurology at the Department of Neurology in the Mayo Clinic.
Further resources: clusterbusters.org/.

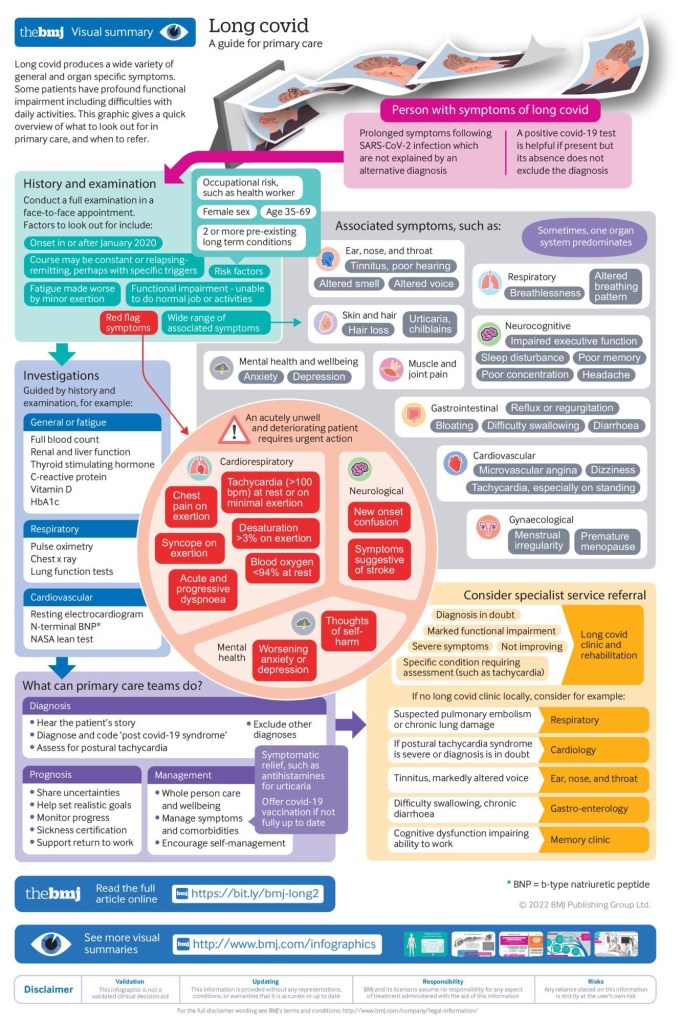
Infographic: History And Symptoms Of Long Covid

MEDICINE: ‘DIABETES’ – RISKS & DIAGNOSIS (BMJ PODCAST)
In this episode of the JIM Podcast, Editor-in-Chief Richard McCallum speaks with David Cistola of Texas Tech University Health Sciences Center El Paso about American Diabetes Month.

INFOGRAPHIC: EXERCISE FOR ‘CLAUDICATION’ (BMJ STUDY)
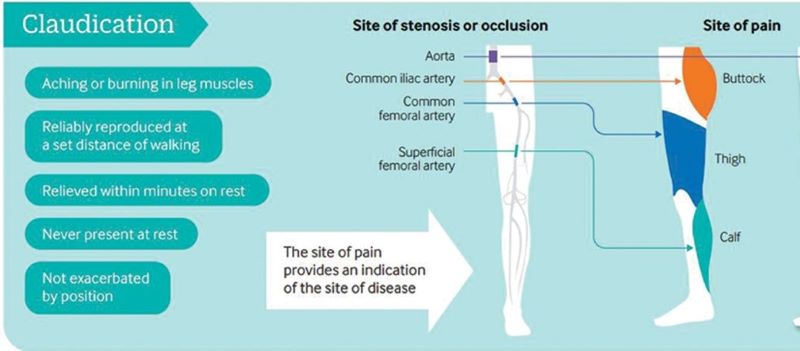
Exercise training is a safe, effective and low-cost intervention for improving walking ability in patients with IC. Additional benefits may include improvements in QoL, muscle strength and cardiorespiratory fitness. Clinical guidelines advocate supervised exercise training as a primary therapy for IC, with walking as the primary modality.
However, evidence is emerging for the role of various other modes of exercise including cycling and progressive resistance training to supplement walking training. In addition, there is emerging evidence for home-based exercise programmes. Revascularisation or drug treatment options should only be considered in patients if exercise training provides insufficient symptomatic relief.
Abstract
Peripheral artery disease (PAD) is caused by atherosclerotic narrowing of the arteries supplying the lower limbs often resulting in intermittent claudication, evident as pain or cramping while walking. Supervised exercise training elicits clinically meaningful benefits in walking ability and quality of life. Walking is the modality of exercise with the strongest evidence and is recommended in several national and international guidelines. Alternate forms of exercise such as upper- or lower-body cycling may be used, if required by certain patients, although there is less evidence for these types of programmes. The evidence for progressive resistance training is growing and patients can also engage in strength-based training alongside a walking programme. For those unable to attend a supervised class (strongest evidence), home-based or ‘self-facilitated’ exercise programmes are known to improve walking distance when compared to simple advice. All exercise programmes, independent of the mode of delivery, should be progressive and individually prescribed where possible, considering disease severity, comorbidities and initial exercise capacity. All patients should aim to accumulate at least 30 min of aerobic activity, at least three times a week, for at least 3 months, ideally in the form of walking exercise to near-maximal claudication pain.

TOP MEDICAL PODCASTS: ‘DIVERTICULAR DISEASE’ (BMJ)
Colonic diverticulosis refers to herniation of the mucosa and submucosa through the muscular layer of the colonic wall and may be the result of colonic smooth muscle over-activity. Diverticular disease may be defined as any clinical state caused by symptoms pertaining to colonic diverticula and includes a wide-ranging spectrum from asymptomatic to severe and complicated disease.
Mohamed Thaha, Senior Lecturer & Lead Consultant in Colorectal Surgery, National Bowel Research Centre, Barts and The London School of Medicine and Dentistry, tells us more.

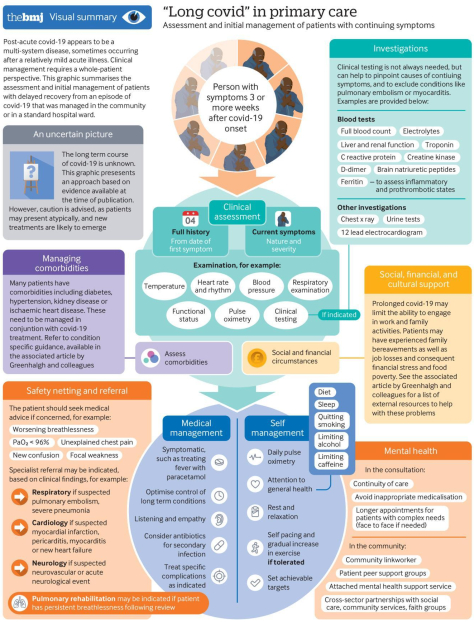
INFOGRAPHIC: PROLONGED COVID-19 SYMPTOMS – “A MULTI-SYSTEM DISEASE” (BMJ)

COMMENTARY
COVID 19 is a nasty disease, in case you hadn’t noticed. It is SNEAKY: you can catch it from a person who has no symptoms.
It is UNPREDICTABLE: you may develop no symptoms or Die from it. It can affect any part of your body, including HEART and BRAIN.
And now we hear that it can DRAG ON. The outstanding infographic, “a multi-systems disease, which is intended for PRIMARY CARE PROVIDERS, has a lot to offer patients, who can do a lot to Care for themselves:
- –They can get a THERMOMETER and a PULSE OXIMETER to watch their own temperatures and oxygen saturations
- –They can monitor their own COMORBIDITIES, like Diabetes and HYPERTENSION, which are common with severe Covid. In patients who get very ill .
- –They can watch their GENERAL HEALTH, including SLEEP and DIET (the exercise part is relegated to DOCTORS recommendations).
You should also RESTRICT Alcohol, Caffeine and it goes without saying CIGARETTE SMOKING. Of course PREVENTION, with DISTANCING, MASKING and being Outside, coupled with SLEEP, DIET and EXERCISE is always best.
–Dr. C.

COGNITION & BRAIN STUDIES: APATHY, NOT DEPRESSION, ASSOCIATED WITH DEMENTIA

We tested the hypothesis that apathy, but not depression, is associated with dementia in patients with SVD. We found that higher baseline apathy, as well as increasing apathy over time, were associated with an increased dementia risk. In contrast, neither baseline depression or change in depression was associated with dementia. The relationship between apathy and dementia remained after controlling for other well-established risk factors including age, education and cognition. Finally, adding apathy to models predicting dementia improved model fit. These results suggest that apathy may be a prodromal symptom of dementia in patients with SVD.
Cerebral small vessel disease (SVD) is the leading vascular cause of dementia and plays a major role in cognitive decline and mortality.1 2 SVD affects the small vessels of the brain, leading to damage in the subcortical grey and white matter.1 The resulting clinical presentation includes cognitive and neuropsychiatric symptoms.1
Apathy is a reduction in goal-directed behaviour, which is a common neuropsychiatric symptom in SVD.3 Importantly, apathy is dissociable from depression,3 4 another symptom in SVD for which low mood is a predominant manifestation.5 Although there is some symptomatic overlap between the two,6 research using diffusion imaging reported that apathy, but not depression, was associated with white matter network damage in SVD.3 Many of the white matter pathways underlying apathy overlap with those related to cognitive impairment, and accordingly apathy, rather than depression, has been associated with cognitive deficits in SVD.7 These results suggest that apathy and cognitive impairment are symptomatic of prodromal dementia in SVD.

MEDICAL PODCAST: “ASSESSING CHEST PAIN” (BMJ)

Chest pain is a common chief complaint. It may be caused by either benign or life-threatening aetiologies and is usually divided into cardiac and non-cardiac causes. James E. Brown, Professor and Chair, Wright State University Boonshoft School of Medicine, Kettering, Ohio, gives us an overview of assessing chest pain in the emergency setting.
COMMENTARY
Dr. James E Brown of the Wright State school Of medicine in Kettering Ohio gave a very interesting discussion of chest pain.
One interesting takeaway is the value of a very experienced clinician dealing with large volumes of emergency room patients. This would make telemedicine with an emergency room hub in a teaching center a very attractive platform.
The consultant doctor in the center has the advantage of his vast experience in rapidly narrowing down the heterogeneous list of different diagnoses that must be considered- the “differential diagnosis”.
Dr. Brown mentioned the “gestalt”, the incorporation of subjective features such as facial and voice cues which add to the objective parameters in patient evaluation. This of course would be amenable to telemedicine although other old-time clinical information like the changes in breath sounds would be more favorable to conventional in-person evaluation.
Ultrasound would More easily be done locally as well.
An interesting take away from this discussion is the value of The patient’s history and past laboratory data, so undervalued by rushed modern doctors. For instance, Electronic medical records (EMR) could provide past history or a previous electrocardiogram for comparison.
Dr. Brown favors the division of chest pain causes into cardiac and non-cardiac. It is easy to develop tunnel vision and look at the patient only as a possible coronary thrombosis. In fact it is better to Rapidly consider the non-cardiac causes that would demand immediate attention while waiting for the results of the Troponin-T test.
For instance pulmonary embolism, aortic dissection, tension pneumothorax, cardiac Tamponade should be considered.
These considerations should be running through the head of the clinician as the IV, EKG, and pulse oximetry are being set up.
In addition to the Troponin-T, bedside ultrasound, and Higher “slice count” CAT machines, and higher “Tesla” MRIs are becoming available major centers which could support small emergency rooms.
If there is One place where “the Flow” would be Appropriate it would be in the mind of the emergency room doctor evaluating acute chest pain.
I have a hard time imagining artificial intelligence endangering her job.
—Dr. C.

PODCAST: “MEDDIET” ALTERS GUT MICRIOBIOME IN OLDER PEOPLE, IMPROVES FRAILTY, COGNITION, INFLAMMATION
We observed that increased adherence to the MedDiet modulates specific components of the gut microbiota that were associated with a reduction in risk of frailty, improved cognitive function and reduced inflammatory status.
Dr Philip Smith, Digital and Education Editor of Gut and Consultant Gastroenterologist at the Royal Liverpool Hospital interviews Professor Paul O’Toole; who is Professor of Microbial Genomics, Head of School of Microbiology and Principal Investigator in APC Microbiome Ireland, an SFI funded centre at University College Cork, Ireland, on “Mediterranean diet intervention alters the gut microbiome in older people reducing frailty and improving health status: the NU-AGE 1-year dietary intervention across 5 European countries” published in paper copy in Gut in July 2020.
COMMENTARY
Diet is one of the 3 pillars ( or 4, if you don’t consider intellectual stimulation a form of exercise) of health. And there are 3 prime dimensions to diet: Quality, Quantity, and Timing. This excellent study addresses the Quality of the diet. Vegetables, fruits and whole grains are the foundation.
Dietary Fiber is the main difference between the healthful Mediterranean diet and the highly processed diet so common in America.
How can you be sure you are eating enough fiber? Read on.
On almost all cans and boxes, you will find a nutritional statement, by law. Assuming that the contents are “real food”, and preferably “organic”, look for the “fiber” in grams, and the “calories” in 100’s, and mentally divide the grams of fiber by 100s of calories, and you get a number. Let’s say that your fiber for the day totals “25” gms. and your calories for the day Totals 2500; that is “25” hundred calories. Divide the 25 grams by the 25 hundred calories, and you get “1”. Anything less than 1 is low in fiber.
25 grams of fiber is about the daily recommendation for fiber. 25 hundred calories is a ballpark figure for an average diet.
PORTION SIZE DOESN’T MATTER, since your dividend is a ratio.
The bacteria in your MICROBIOME feed on the fiber, and the higher and more diverse the fiber ( within reason. Hay is high in fiber) the healthier the food.
Blueberries are good for a fruit at 4-5 gms. of fiber per hundred calories. Broccoli is a good vegetable at 10 gms fiber per hundred calories, carrots about 3, and so on.
Sugar is the perfect “bad” food, at no fiber for as many calories as you can pack in. It makes you Want more, and “desensitizes” your taste buds to the natural sweetness of fruit, or even vegetables.
HIGH FIBER foods are MORE FILLING, leading you to eat less.
Civilization and Capitalism pushes too much food and too many calories at us. Overeating , obesity, and many of the modern illnesses is the result.
Generally, fresh fruits and vegetables are preferred, though cooking doesn’t do much harm, other than some vitamin loss that can be replaced.
Whole grain cereals have fiber in addition to other nutrients. Also, the complex carbohydrates in whole grains are released more slowly than wIth refined cereals. This floods your blood less rapidly with glucose, and elicits a Less precipitous insulin response. This results in a lower, healthier “glycemic Index”.
Vegetables, fruits Legumes, seeds, nuts and their oils are the mainstay of the Vegan diet, which is healthful If enough protein and essential fats are ingested.
Fish, eggs, milk and cheeses are other components of the Mediterranean diet.
I take many of my daily Vegetable and fruits and liquefy them in a food blender. Drinking my daily vegetables and fruits is a tasty and convenient way to improve my diet. I Savor individually those items I find most tasty, like nuts, apples, avocado, And fruit in season. This exercises my jaws, which is probably healthy.
YOUR MICROBIOME helps you in many ways that science is just beginning to understand. A healthy Microbiome is a DIVERSE Microbiome. FIBER is the food of the Microbiome, and a diversity in dietary fiber leads to a diverse Microbiome. A diverse, happy Microbiome produces many biological substances, like neurotransmitters, and probably communicates with the brain directly through the gut-brain Axis.
The Podcast on the 1 year Meddiet showed how directly a diet can BENEFIT HEALTH STATUS.
