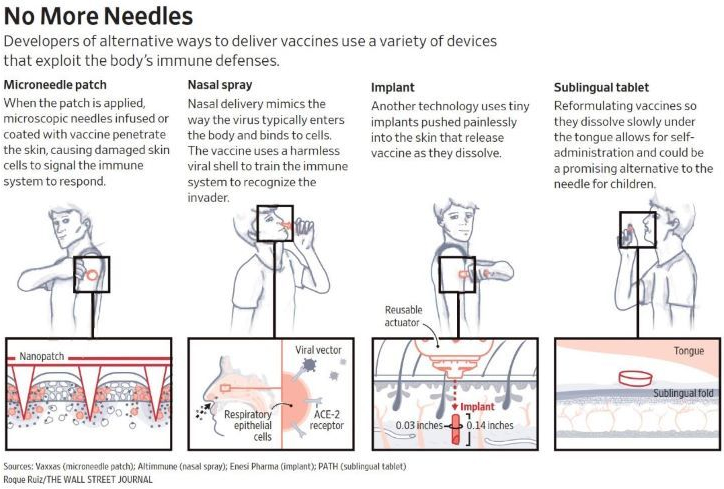
Technologies in development for delivering vaccines include Enesi’s dissolving implants, microneedle patches, electrical-pulse systems, nasal sprays and even pills.
Some firms are developing their own vaccines against Covid-19, while others are aiming to reformulate some of the dozens already in development or being rolled out world-wide. Some are sitting this pandemic out in the hope of being ready for the next one.
All are in the early to mid-stages of development and clinical testing, suggesting it might be months if not years before they come to market. Big pharmaceutical companies have so far shown limited interest.
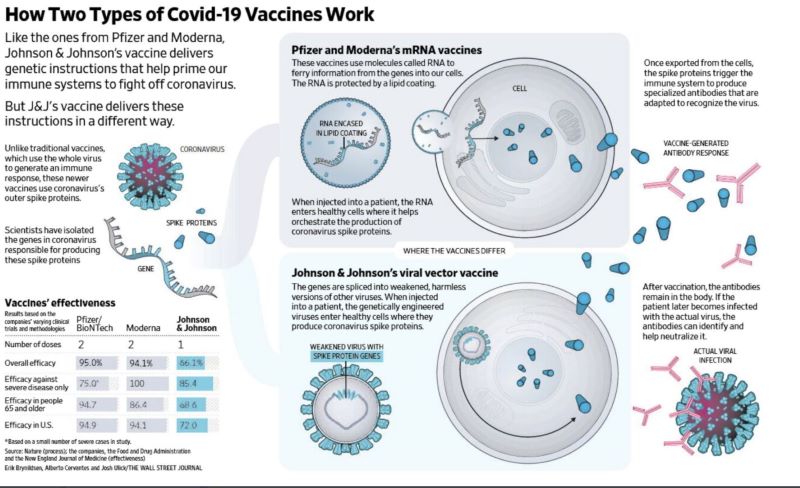
There are all sorts of different vaccines but many of them share specific types of ingredients. Josh Toussaint-Strauss talks to Professor Adam Finn to find out what is in most conventional vaccines, as well as what they do to our bodies when we take them – and why the mRNA Covid jabs from Pfizer/BioNTech, Oxford/AstraZeneca and Moderna work differently.
Enter the intranasal vaccine, which abandons the needle and syringe for a spray container that looks more like a nasal decongestant. With a quick spritz up the nose, intranasal vaccines are designed to bolster immune defenses in the mucosa, triggering production of an antibody known as immunoglobulin A, which can block infection. This overwhelming response, called sterilizing immunity, reduces the chance that people will pass on the virus.
The development of highly effective COVID vaccines in less than a year is an extraordinary triumph of science. But several coronavirus variants have emerged that could at least partly evade the immune response induced by the vaccines. These variants should serve as a warning against complacency—and encourage us to explore a different type of vaccination, delivered as a spray in the nose. Intranasal vaccines could provide an additional degree of protection, and help reduce the spread of the virus.
Pink urine! You can imagine my shock. What could it be? I exercise more than 1½ hours a day. Could it be myoglobin? I put beets in my daily osterizer “shake”: could the color be from the anthocyanins from beets?
I took a urine specimen to the lab, and the color turned out to be from Hemoglobin, the most likely cause all along. There were lots of red blood cells in my urine and the test strip was strongly positive for Hemoglobin. I called a urologist, who said I needed a Urine culture for infection, and a “CT Urogram”, to check for cancer, kidney stones and other problems.
You should always check with your doctor with Hematuria, and I am no exception. My Urology appointment was in 1 week. I got a urine culture, Cell cytology (for cancer), a CT Urogram, and a urine culture before the visit. I wanted to save time by scheduling a Cystoscopy at the time of the first visit, but couldn’t arrange it.
I went for the appointment. They took a blood pressure, but didn’t check my urine, which I thought was negligent. I had been regularly checking my urine for blood by a test strip, and it was negative. The appointment lasted only minutes. My old urologist always checked my urine on every visit, regardless of whether it was a regular check or to consult for a problem. If I were a Urologist, you can be sure I would have my microscope ready, have the nurse collect the urine, spin it down, and put the sediment under the microscope for me to check.
When I was in medical practice as an allergist, I would have my nurse check any sputum the patient produced smeared on a slide, stained and dried. Microscopic examination of urine and sputum takes only seconds and yields lots of information. In my opinion, 50 years of Insurance surveillance and governmental regulations, including restrictions on lab work done in the doctor’s office and Hippa privacy laws, have handicapped Doctors and are partly responsible for the costly, dysfunctional system that is modern medicine.
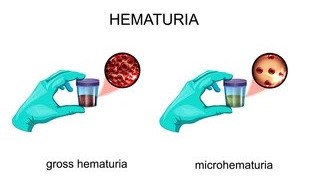
Sorry for the Sermons. Visible blood in the urine-Gross Hematuria- requires that you see your Doctor and find the cause of that blood. Please see the 2 appended Mayo Clinic articles for more detail.
Colorectal cancer is comprised of colon cancer and rectal cancer, which originate in the lower portion of the large intestine and into the rectum. As with other cancers, screening for early detection should not be delayed. “The vast majority of the time, we don’t know exactly what causes any specific cancer,” says Dr. Jeremy Jones, a Mayo Clinic oncologist. “But there are a number of factors that can increase the risk of developing colon or rectal cancer.” Dr. Jones says one risk factor is increasing age. However, he adds that over the last 30 years younger patients have seen a 50% increased risk of developing colon and rectal cancers. In this Mayo Clinic Q&A podcast, Dr. Jones talks about risk factors, symptoms, treatment, health care disparities and the latest in colorectal cancer research. ____________________________________________
As highly transmissible coronavirus variants sweep across the world, scientists are racing to understand why these new versions of the virus are spreading faster, and what this could mean for vaccine efforts. New research says the key may be the spike protein, which gives the coronavirus its unmistakable shape. Illustration: Nick Collingwood/WSJ
Empowering Patients Through Education And Telemedicine