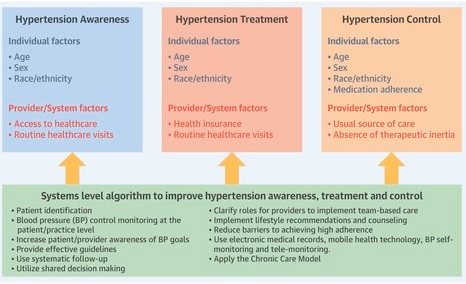
Systemic arterial hypertension is the most important modifiable risk factor for all-cause morbidity and mortality worldwide and is associated with an increased risk of cardiovascular disease (CVD).
Fewer than half of those with hypertension are aware of their condition, and many others are aware but not treated or inadequately treated, although successful treatment of hypertension reduces the global burden of disease and mortality. The aetiology of hypertension involves the complex interplay of environmental and pathophysiological factors that affect multiple systems, as well as genetic predisposition.
The evaluation of patients with hypertension includes accurate standardized blood pressure (BP) measurement, assessment of the patients’ predicted risk of atherosclerotic CVD and evidence of target-organ damage, and detection of secondary causes of hypertension and presence of comorbidities (such as CVD and kidney disease). Lifestyle changes, including dietary modifications and increased physical activity, are effective in lowering BP and preventing hypertension and its CVD sequelae.
Pharmacological therapy is very effective in lowering BP and in preventing CVD outcomes in most patients; first-line antihypertensive medications include angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, dihydropyridine calcium-channel blockers and thiazide diuretics.
Learning about hypertension can be intimidating. Leslie Thomas M.D., a nephrologist at Mayo Clinic, walks you through the facts, the questions, and the answers to help you better understand this condition.
Video timeline: 0:00 Introduction 0:39 What is hypertension? 1:13 Who gets hypertension? / Risk factors 2:18 Symptoms of hypertension 2:36 How is hypertension diagnosed? 3:14 Treatment options 3:51 Coping methods/ What now? 4:05 Ending
COMMENTARY:
Hypertension is an elevation of the blood pressure in the arteries. It is measured conventionally by blood pressure cuffs, although a catheter in the artery is more accurate. I’ve had my blood pressure taken countless numbers of times by nurses and doctors who sometimes put the cuff on my arm through a piece of clothing, making it less accurate. Sometimes it is taken by an automatic blood pressure cuff even in the doctors office. The automated cuff can be purchased for $20 or less for you to use it at home, but it’s accuracy is questionable when you have an irregular heartbeat with atrial fibrillation such as I do.
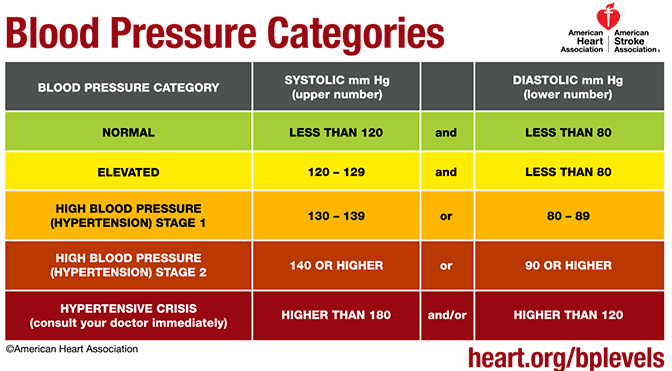
The blood pressure reading which is considered to be normal Is dropping. In the present video, following 2017 guidelines , they state that a systolic reading of more than 120 mmHg is elevated, and anything more than 130 is hypertension. It may be true that studies have been done to show that these slight elevations cause problems, but so can the drugs that are used to lower blood pressure; a cough can be caused by ACE inhibitors. Fatigue and fainting can be caused by an excessive dosage of any blood pressure medication.
Healthy diet, especially avoiding extra salt, Regular exercise and good sleep will go a long way towards keeping your blood pressure at 120 or below on the high reading (systolic), and 80 on the low reading (diastolic).
My systolic blood pressure varies between 120 and 140 systolic, and is usually around 60 diastolic. For a long time I thought the relatively low (diastolic) blood pressure was more important, since diastole is of greater duration than systole, but it has now been determined that the systolic blood pressure reading is the one to worry about. Calcification and lack of elasticities in the arteries as you get older can lead to higher systolic blood pressure.
It used to be thought that the normal systolic blood pressure was 100+ your age in years. Those days are gone, however, and greater life expectancy and health Is one result of carefully monitoring your blood pressure, and working hard to keep it down.
Please refer to the Mayo Clinic article to give you (much) more information.
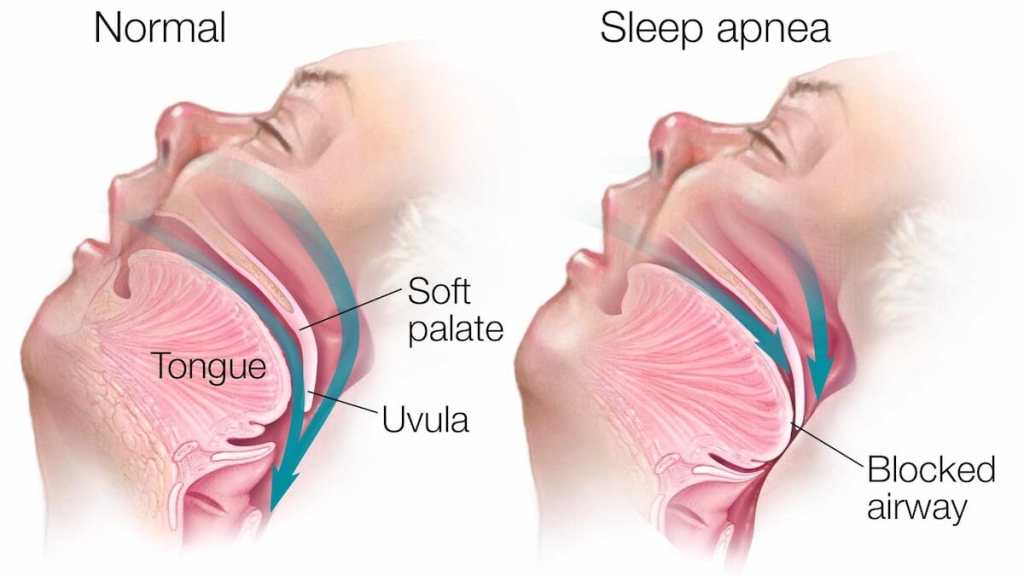
Sleep apnea and obesity are bound together as Charles dickens observed in his Pickwick papers. The Pickwickian syndrome is obesity associated with alveolar hypoventilation(insufficient breathing) with an increase in CO2 in the bloodstream which causes narcosis, or SLEEPINESS, in the daytime.
When I went in for my sleep apnea study, I noticed a number of double wide chairs available for the usual clientele there. OBESITY is one of the major risk factors for sleep apnea. Depositions at the base of the tongue and throat interfere with breathing, and causes snoring to the point of tracheal blockage and apnea at night.
Some people with normal “ BMI”, have sleep apnea. Sleep apnea can run in families, occur when you are older, or have a thick neck. So no matter what your weight, if you have daytime sleepiness after an apparently full night of sleep, you should be considered for a sleep study.
A SLEEP STUDY requires that you go into a sleep center overnight, get hooked up to an electroencephalogram machine, oxygen monitor, chest straps, and the like. This is the gold standard for a diagnosis of sleep apnea, but a recording pulse oximeter will let you know a lot less expensively if you have the critical problem, a drop in oxygen saturation. The type of sleep apnea I have been discussing so far is obstructive sleep apnea. Of course there are other types such as central, or complex sleep apnea.
Most sleep apnea responds to nasal CPAP, if you can tolerate it. My own sleep apnea was diagnosed as moderate, 15% central and 85% obstructive in type. I have a stuffy nose which I believe to be the main problem setting me up for sleep apnea, and I could not tolerate the positive nasal CPAP. There is also a dental apparatus that I tried unsuccessfully. I wound up sleeping on my side, and propping myself in that position with pillows .This seems to help me, but I still wake up several times a night, usually at the end of a 90 minute sleep cycle, and with a full bladder.
I sleep through better on days when I have had more physical or mental exercise. Avoiding a full stomach at bedtime is also helpful with both sleep apnea and GERD.
I do use Afrin on the left side of my nose, which is more obstructed. I restrict the use to every third day, although I have heard that you can use it every other day, alternating sides, if you have a stuffy nose that has resisted other treatments .I have also heard that using corticosteroid nasal sprays makes Afrin better tolerated. Be sure to get clearance with your doctor before trying this.
Hypertension places an extra load on the blood vessels and heart, and eventually causes them to become diseased. High Blood Pressure is therefore bad for the entire body, which depends on the blood vessels for delivering the nutrients and oxygen necessary for life.
Most hypertension happens from subtle changes in the body’s signalling systems, and often runs in families; This is called “essential hypertension”. Additionally, there are a number of diseases and conditions of which hypertension is a symptom. It is important to know if you have hypertension, and fortunately it is easy to discover.
A visit to the doctor, or even to the pharmacy will make a reading available, and if you are concerned, an automatic cuff is available for $20. A healthy lifestyle and weight Will help prevent and treat hypertension, as in so many other chronic conditions.
A variety of medications are available to treat hypertension, but ANY MEDICATION CAN PRODUCE SIDE EFFECTS. It is rare for an effective medication to produce only a single, desired effect on the body. I have never known a person who at some time did not experience some side effect from antihypertensive medications.
Be sure to maintain contact with your Doctor. The dose may be too high, causing episodes of LOW blood pressure with fainting. When I was in practice, any number of patients came to me with a chronic cough, which I “cured” by having their doctor replace their ACE Inhibitor with another medication.
Please read the accompanying Mayo Clinic article for a complete discussion of this important condition.
The number of older people, including those living with dementia, is rising, as younger age mortality declines. However, the age-specific incidence of dementia has fallen in many countries, probably because of improvements in education, nutrition, health care, and lifestyle changes.
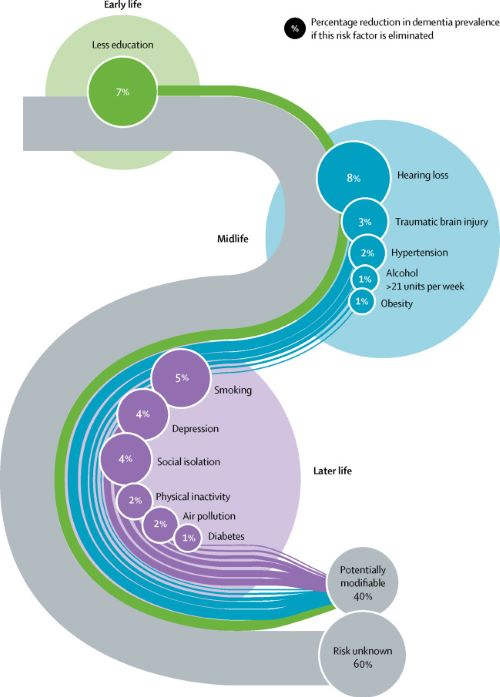
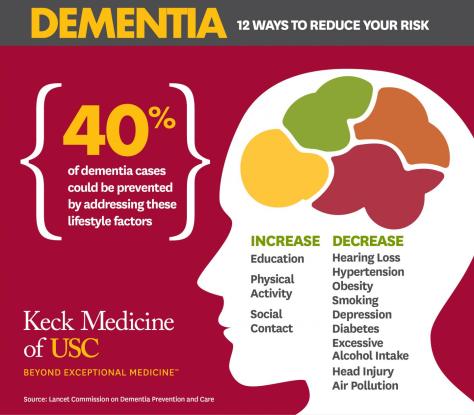
Overall, a growing body of evidence supports the nine potentially modifiable risk factors for dementia modelled by the 2017 Lancet Commission on dementia prevention, intervention, and care: less education, hypertension, hearing impairment, smoking, obesity, depression, physical inactivity, diabetes, and low social contact.
We now add three more risk factors for dementia with newer, convincing evidence. These factors are excessive alcohol consumption, traumatic brain injury, and air pollution. We have completed new reviews and meta-analyses and incorporated these into an updated 12 risk factor life-course model of dementia prevention. Together the 12 modifiable risk factors account for around 40% of worldwide dementias, which consequently could theoretically be prevented or delayed.
The potential for prevention is high and might be higher in low-income and middle-income countries (LMIC) where more dementias occur. Our new life-course model and evidence synthesis has paramount worldwide policy implications. It is never too early and never too late in the life course for dementia prevention. Early-life (younger than 45 years) risks, such as less education, affect cognitive reserve; midlife (45–65 years), and later-life (older than 65 years) risk factors influence reserve and triggering of neuropathological developments.
Culture, poverty, and inequality are key drivers of the need for change. Individuals who are most deprived need these changes the most and will derive the highest benefit.
Lancet’s 2017 Metanalysis mentions 9 Dementia risk factors. The 2020 Paper adds 3 additional factors. TRAUMATIC BRAIN INJURY, ALCOHOLISM, and AIR POLLUTION.
The inclusion of Trauma, with a 3% weighting, may be due to the increased awareness of TBE stemming from football injuries. The preventable 12 Factors are still in the minority. 60% of the factors are not preventable, since they are Genetically determined.
LESS EDUCATION, HEARING LOSS and SOCIAL ISOLATION, 3 of the original 9 factors,all lead to less brain stimulation, and can be unified under the idea of COGNITIVE RESERVE. If a person starts with less Cognition, it is reasonable to think he would be Demented sooner.
Together, less education, hearing loss, and social isolation account for almost Half of the correctable conditions. SMOKING is one of those things which impact almost every human disorder. It is amazing that cigarettes are still manufactured. In fact, their use is actually Increasing,especially the Far East, where they probably account for much of the escalating problem with Dementia in that region.
Our favorite causes, Sleep, Diet, and Exercise, apparently play only a minor role in Dementia. Sleep is completely dismissed in this report. The fact that both Sleeping less than the Ideal 7-8 hours, and more than that amount is thought to correlate with health problems is probably the main reason for the omission.
My own opinion is that people who are in poor health may need more sleep, and therefore sleep longer. My own sleep is interrupted 3-5 times per night, so it is not surprising that I need an hour extra to feel rested. Any less than 9-10 hours, and I need a nap, which in my opinion is a sign of insufficient nighttime sleep. Poor sleep may be a factor in metabolic syndrome, often leading to DIABETES, OBESITY, and HYPERTENSION, which are factors in Dementia, mentioned in the article as bit players.
PHYSICAL INACTIVITY is mentioned as a minor factor in Dementia, but exercise, studied as a treatment of dementia, was found to improve only strength. Diet is not mentioned, but does contribute to OBESITY, which is a minor factor. Dementia is a great emotional and economic burden, afflicting many otherwise happy families with misfortune.
The Lancet metanalysis is admirable. But don’t forget the healthy lifestyle emphasizing Sleep Diet and Exercise; and exercise includes cognitive exercise. Anything we can do to avoid dementia is worthwhile. –
The US Surgeon General’s office has released a report emphasizing the importance of making hypertension control a national public health priority. Vice Admiral Jerome Adams, MD, MPH, the 20th US Surgeon General, discusses the report’s background and recommendations.
“We are learning that tactics to avoid dementia begin early and continue throughout life, so it’s never too early or too late to take action,” says commission member and AAIC presenter Lon Schneider, MD, co-director of the USC Alzheimer Disease Research Center‘s clinical core and professor of psychiatry and the behavioral sciences and neurology at the Keck School of Medicine of USC.
LOS ANGELES — Modifying 12 risk factors over a lifetime could delay or prevent 40% of dementia cases, according to an updated report by the Lancet Commission on dementia prevention, intervention and care presented at the Alzheimer’s Association International Conference (AAIC 2020).
Twenty-eight world-leading dementia experts added three new risk factors in the new report — excessive alcohol intake and head injury in mid-life and air pollution in later life. These are in addition to nine factors previously identified by the commission in 2017: less education early in life; mid-life hearing loss, hypertension and obesity; and smoking, depression, social isolation, physical inactivity and diabetes later in life (65 and up).
Schneider and commission members recommend that policymakers and individuals adopt the following interventions:
Aim to maintain systolic blood pressure of 130 mm Hg or less from the age of 40.
Encourage use of hearing aids for hearing loss and reduce hearing loss by protecting ears from high noise levels.
Reduce exposure to air pollution and second-hand tobacco smoke.
Prevent head injury (particularly by targeting high-risk occupations).
Limit alcohol intake to no more than 21 units per week (one unit of alcohol equals 10 ml or 8 g pure alcohol).
Stop smoking and support others to stop smoking.
Provide all children with primary and secondary education.
Lead an active life into mid-life and possibly later life.
Reduce obesity and the linked condition of diabetes.
Headache has been with us since Neolithic times, and has caused enough distress to induce our ancestors to scrape holes in their skulls, perhaps to let out the causative Evil Spirits, or maybe a subdural hematoma.
When I was a practicing Allergist, i was sent many headache patients by other Doctors.This was, presumably, because the referring physician thought that their patients had “sinus” headaches. In fact, free standing headache does not commonly come from the sinuses.
Most headaches thought due to ‘sinuses” are in fact “vascular “ headaches. The theory of vascular headaches is that the average diet contains many chemicals that are active on blood vessels. Tyramine, degraded proteins and caffeine are examples. These chemicals, working on the blood vessels, cause irritation and pain. It follows,then, that avoidance of these chemicals would relieve the vascular headaches.
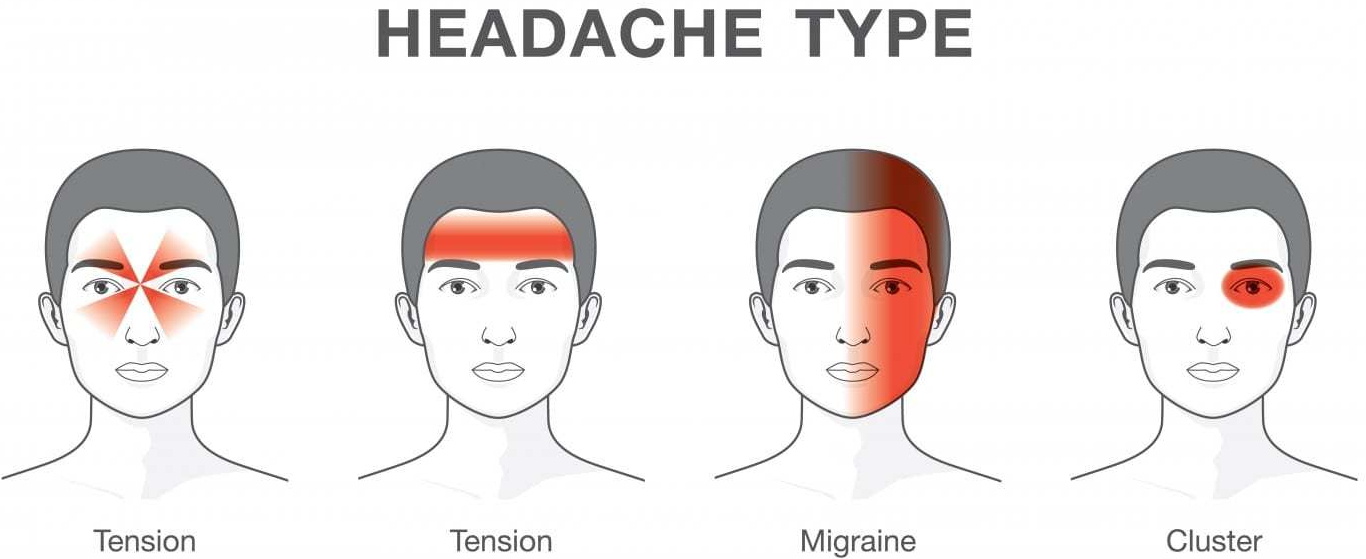
“Vascular headache”, and it’s severe cousin, Migraine headache, is now included under PRIMARY HEADACHE, which also includes Tension headache, and a variety of less common diagnoses. But it is still useful for Treatment, which is why I use the term.
My treatment was a fresh, “health food” diet which avoided preserved foods such as salami, sausages, sauerkraut, leftovers, cheeses, red wine and a variety of other foods likely to have degraded amino acids and Tyramine.
The “mold-free diet” was the published diet closest to listing the suspected foods. The benefit reported from the diet encouraged me to continue recommending it. Vascular headaches are essentially a mild variety of migraine headaches. The foods avoided in the “mold-free diet” are still, after several decades of progress still recognized as migraine triggers.
I encountered only one patient with BRAIN TUMOR in my practice. She had severe, unremitting, gradually increasing headaches over a 4 week period. I called a Neurologist, the type of doctor that treats most severe headaches, who informed me he had NEVER seen a patient with a brain tumor who presented with a headache only, so uncommon it is.
Tension Headaches are milder, and usually can be handled at home. These headaches are usually accompanied by tenderness in the muscles of the back of the neck, or in the temple region, and are brought on by stress.
Hypertension, if extremely high, can cause headache, and can be dangerous, but I never saw a case. Nor did I attend a patient with temporal arteritis, which can also be an emergency.
There are some “red flags” that indicate urgent need for evaluation:
New headache in older patient
New change in headache pattern, or progressively worsening headache
Signs and symptoms of illness ( fever, stiff neck, rash).
Headache triggered by cough or exertion.
Headache in pregnancy or postpartum period
First, worst Headache.
New headaches with AIDS, compromised immunity, or cancer.
Headaches accompanied by mental changes, weakness, or abnormal Neurological signs.
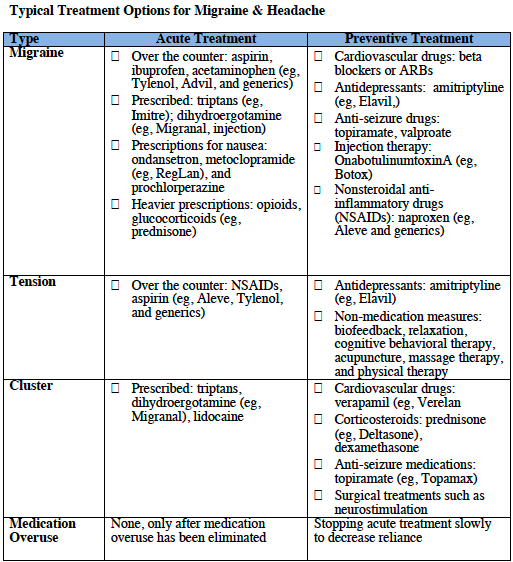
Selective medications are available for some headaches.
Preventative and abortive medications sometimes are helpful for migraine. Antidepressants, tryptans, beta blockers, and corticosteroids are medications best prescribed by specialists.
The tendency to use pain killers, especially narcotics, must be tempered. Frequent use can create additional problems, like ADDICTION. The CAUSE of the headache must be found, if possible, and specifically treated.
Of course, I did find patients with true SINUS HEADACHE, but the headache was accompanied by fever, tenderness over the sinuses, yellow nasal discharge, and other evidence of SINUSITIS, and went away when the infection was treated.
If you have a lot of headaches, and no “red flags” or “risk factors”, you might try a “mold free diet” for a few weeks. Your Nutrition and health would certainly not suffer. And you might have fewer headaches!
Please read the following article for a more complete discussion of this common and annoying problem.