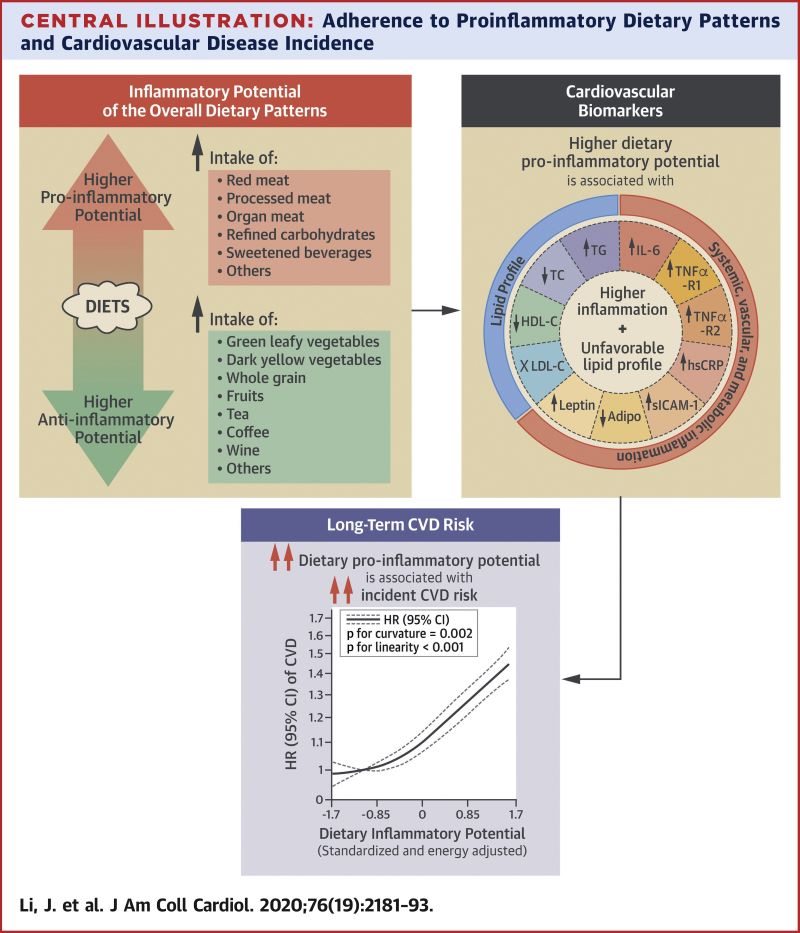
Dietary patterns with a higher proinflammatory potential were associated with higher CVD risk. Reducing the inflammatory potential of the diet may potentially provide an effective strategy for CVD prevention.
Background
Inflammation plays an important role in cardiovascular disease (CVD) development. Diet modulates inflammation; however, it remains unknown whether dietary patterns with higher inflammatory potential are associated with long-term CVD risk.
There may be few issues that unite Americans ahead of the 2020 election as do their concerns about the cost of prescription drugs.
A clear majority — 75% — of respondents to a July survey said the cost of prescription medicines would be among the factors likely to influence their votes this year, according to a report from Gallup and the nonprofit West Health. Gallup reported on results from 1,007 interviews conducted with adults between July 1 and July 24.
1. What are the 2020 presidential candidates saying they will do to lower drug prices?
Both President Donald Trump, a Republican, and former Vice President Joe Biden, a Democrat, have highlighted insulin costs in their discussions of the need to lower drug prices.
In a January interview with the New York Times editorial board, Biden noted the widespread discontent among Americans about sticker shock often experienced at pharmacies. He spoke of a need for the federal government to act to make medicines more affordable.
“This is a place where I find, whether you’re Republican or Democrat, you think you’re getting screwed on drug prices. And you are, in terms of everything from insulin to inhalers and a whole range of other things,” Biden said. “So, again, can I guarantee that it gets done? No, but I can tell you what, if anybody can get it done, I can, and I think there’s a consensus for it.”
2. Why doesn’t Medicare, the biggest U.S. purchaser of drugs, directly negotiate on drug prices?
Congress has taken different approaches in designing the terms under which the two largest federal health programs, Medicaid and Medicare, buy drugs.
Medicaid is a program run by states with federal contributions and oversight. It covers people with low incomes and disabilities. Almost 67 million people were enrolled in Medicaid as of May 2020, including about 29 million children. In 1990 Congress decided that drugmakers who want to have their products covered by Medicaid must give rebates to the government. The initial rebate is equal to 23.1% of the average manufacturer price (AMP) for most drugs, or the AMP minus the best price provided to most other private-sector payers, whichever is greater. An additional rebate kicks in when prices rise faster than general inflation.
3. What’s the deal with rebates and discounts?
There’s widespread frustration among lawmakers and policy analysts about the lack of clarity about the role of middlemen in the supply chain for medicines. Known as pharmacy benefit managers (PBMs), these businesses describe the aim of their business as making drugs more affordable for consumers. Insurers like Cigna and UnitedHealth operate some of the nation’s largest PBMs, as does pharmacy giant CVS Health, which also owns insurer Aetna.
“They will tell you their mission is to lower drug costs,” said Rep. Earl L. “Buddy” Carter, a Georgia Republican, a pharmacist and a critic of PBMs, in a speech on the House floor last year. “My question to you would be: How is that working out?”
4. What is the “distinctly American” phenomenon of specialty drugs?
Kesselheim also has written on what he terms “Specialty Drugs — A Distinctly American Phenomenon.” That’s the title of a 2020 paper in the New England Journal of Medicine Kesselheim authored with Huseyin Naci, an associate professor of health policy at the London School of Economics.
In this Perspective article, Kesselheim and Naci look at how the “specialty” designation morphed from its origin in the 1970s. It then referred to a need for extra steps for preparation and delivery of new injectable and infusion products.
5. How much does it cost to bring a new drug to market anyway?
The median cost for a medicine developed in recent years was $985 million, according to a study published in JAMA in March 2020, “Estimated Research and Development Investment Needed to Bring a New Medicine to Market, 2009-2018.”
“Rising drug prices have attracted public debate in the United States and abroad on fairness of drug pricing and revenues,” write the study’s authors: Olivier J. Wouters of the London School of Economics; Martin McKee of the London School of Hygiene and Tropical Medicine; and Jeroen Luyten of Leuven Institute for Healthcare Policy, KU Leuven, Belgium. “Central to this debate is the scale of research and development investment by companies that is required to bring new medicines to market.”
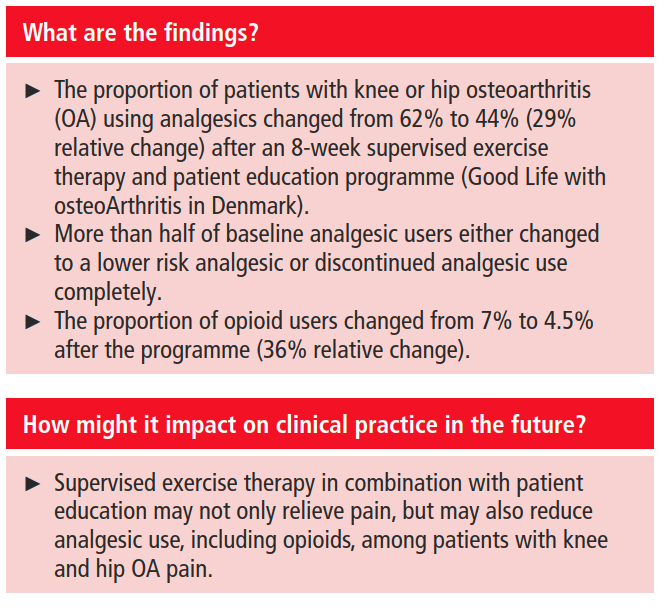
Conclusion Among patients with knee or hip OA using analgesics, more than half either discontinued analgesic use or shifted to lower risk analgesics following an 8-week structured exercise therapy and patient education programme (GLA:D). These data encourage randomised controlled trial evaluation of whether supervised exercise therapy, combined with patient education, can reduce analgesic use, including opioids, among patients with knee and hip OA pain.
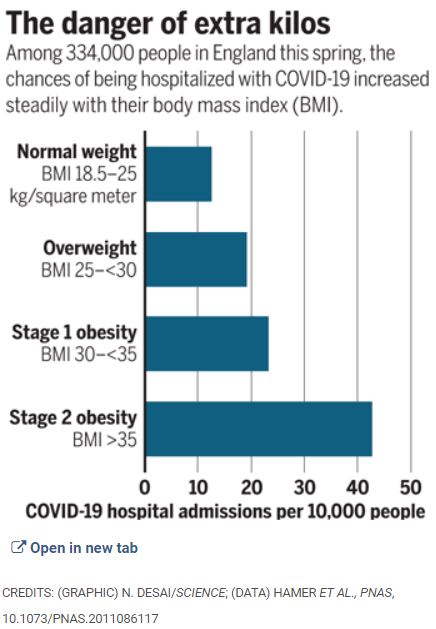
The Journal Science recently reported on nearly 77,000 patients hospitalized with Covid 19. 29% were overweight and 48% were Obese. A total of 77% of admissions for Covid were overweight or worse.
Overweight was defined as BMI of 25-29.9 Kg. per Square Meter, and Obese was defined as BMI of 30 or greater. Another way of stating the data is giving the rate of Hospital admissions per 10,000 People.
Normal Weight, BMI 18.5-25 kg. Per square Meter—12%
Overweight, BMI 25-29.9 per square a Meter———-19%
Obese, BMI 30-34.9 per square Meter——————-23%
Severe Obesity, more than 35 per square meter——-42%
BMI calculators are everywhere to be found on the internet. Put in your weight and height, and find your BMI displayed.
These are striking figures, the more so because of the LARGE SAMPLE, and the LINEAR Relationship; the greater the overweight, the greater the hospitalization rate.
Every way you look at it, obesity is hazardous. More hip and knee replacements, harder to exercise, find comfortable seats, more difficult to do surgery, more diabetes, heart attacks, stroke, Hypertension, Sleep apnea, worse immunity, and now, confirming previous suspicions, clearly higher risk of being hospitalized (and dying) with Covid.
I realize that nobody chooses to be Obese; in addition to the health problems, overweight people are Subjected to discrimination.
Obesity is notoriously hard to treat; one of the few, seldom mentioned medical truths is that Diets fail long term. Starting and maintaining a diet takes Herculean Will Power, which is in short supply in our overindulgent, overadvertised, and overfed society.
If I were morbidly Obese, I might opt for Bariatric Surgery, and try my best to hold the short term weight loss, since even with surgery the pounds tend to creep back on over time.
The best way to treat Obesity is to treat it as the Plague it is. CHILDHOOD OBESITY should be treated aggressively. Keep the Obese Child from becoming an obese adult, and maybe carry yourself along with the Family.
Better yet, Good SLEEP, DIET, and EXERCISE come as an interactive mutually reinforcing package deal. Prevention always beats treatment.
My article on ABDOMINAL FAT is suggested reading, and there is a link to the Infographic which Displays the above date in graphic form.
The Stanford researchers figured out how to regrow articular cartilage by first causing slight injury to the joint tissue, then using chemical signals to steer the growth of skeletal stem cells as the injuries heal. The work was published Aug. 17 in the journal Nature Medicine.
“Cartilage has practically zero regenerative potential in adulthood, so once it’s injured or gone, what we can do for patients has been very limited,” said assistant professor of surgery Charles K.F. Chan, PhD. “It’s extremely gratifying to find a way to help the body regrow this important tissue.”
STANFORD MEDICINE (Aug 17, 2020): Researchers at the Stanford University School of Medicine have discovered a way to regenerate, in mice and human tissue, the cushion of cartilage found in joints.
Loss of this slippery and shock-absorbing tissue layer, called articular cartilage, is responsible for many cases of joint pain and arthritis, which afflicts more than 55 million Americans. Nearly 1 in 4 adult Americans suffer from arthritis, and far more are burdened by joint pain and inflammation generally.
Stanford has come up with a Promising new approach to the surgical treatment of osteoarthritis. Unfortunately for the suffering public, this approach is still in the rodent experimental stage.
The pain of osteoarthritis is caused by the LOSS of the CARTILAGE which insulates the bone of the joints. The wonderful cartilage coating prevents the pain which would result from the rubbing of bone on bone. The best solution in osteoarthritis would be to replace the cartilage, and I have no doubt that this will be possible some day.
STEM CELLS is the theoretical method most commonly imagined when it comes to replacing lost tissue.. Brain cells, cardiac muscle cells, and pancreatic islet cells are some of the research areas. The development of stem cells from the cells of the Patient herself (iSCs) obviates the need for immunosuppression, which plagues allographs ( stem cells or organs from other humans).
Recently, in situ transformation of neighboring cells has been described, which sidesteps the need to introduce any cells. For instance the transformation of astrocytes (a type of brain cell) into neuronal stem cells of the dopamine lineage would be a great boon to Parkinson’s disease.
The Stanford method somewhat resembles this last-mentioned technique. An injury is created where the cartilage is desired. Like any injury, bleeding, clotting, and cell infiltration follows, destined to form a scar. However, the researchers added BMP-2, which in this milieu causes the pro-fibroblasts to head toward the bone (osteoblast) lineage. Since cartilage forms first in a tissue destined to be bone, they then added a VEGF antagonist, which interrupts the transformation in the desired cartilage stage. Both BMP-2 and anti-VEGF have already been approved for use, facilitating the development of this attractive therapy.
The researchers have even identified an excellent potential Patient Population: Osteoarthritis patients scheduled for surgical removal of the first metacarpal articulation with the wrist. They could do their procedure on this area, and if there is no benefit, They could just go ahead with the original plan of removal. The thumb happens to be one of my most painful arthritic areas.
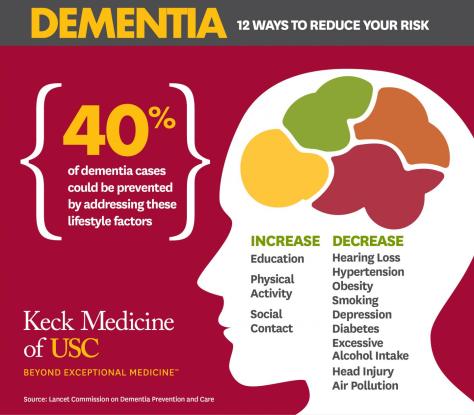
“We are learning that tactics to avoid dementia begin early and continue throughout life, so it’s never too early or too late to take action,” says commission member and AAIC presenter Lon Schneider, MD, co-director of the USC Alzheimer Disease Research Center‘s clinical core and professor of psychiatry and the behavioral sciences and neurology at the Keck School of Medicine of USC.
LOS ANGELES — Modifying 12 risk factors over a lifetime could delay or prevent 40% of dementia cases, according to an updated report by the Lancet Commission on dementia prevention, intervention and care presented at the Alzheimer’s Association International Conference (AAIC 2020).
Twenty-eight world-leading dementia experts added three new risk factors in the new report — excessive alcohol intake and head injury in mid-life and air pollution in later life. These are in addition to nine factors previously identified by the commission in 2017: less education early in life; mid-life hearing loss, hypertension and obesity; and smoking, depression, social isolation, physical inactivity and diabetes later in life (65 and up).
Schneider and commission members recommend that policymakers and individuals adopt the following interventions:
Aim to maintain systolic blood pressure of 130 mm Hg or less from the age of 40.
Encourage use of hearing aids for hearing loss and reduce hearing loss by protecting ears from high noise levels.
Reduce exposure to air pollution and second-hand tobacco smoke.
Prevent head injury (particularly by targeting high-risk occupations).
Limit alcohol intake to no more than 21 units per week (one unit of alcohol equals 10 ml or 8 g pure alcohol).
Stop smoking and support others to stop smoking.
Provide all children with primary and secondary education.
Lead an active life into mid-life and possibly later life.
Reduce obesity and the linked condition of diabetes.
Coffee has a long and colorful history. Billions of cups are consumed daily, and with such a large and passionate audience, I offer you a taste of the aura which abound on the subject of this popular drink.
The African story of happy animals galloping around at night after eating some red berries from bushes more than a thousand years is probably a myth. It wasn’t until 15th C. Yemen that the documented history of coffee begins.
The substance that was initially ingested wasn’t even a beverage, but was more like an evil-tasting paste. The reason that it endured was undoubtedly it’s stimulating quality.
The Muslim world proscribed alcoholic beverages, but coffee enabled the faithful to pray all night, and was welcome. The Time taken to bring the berries to market often resulted in spoilage. The cargo had to travel from Ethiopia to the port of MOCHA in Yemen, and by a long Voyage to middle eastern destinations.
With the blessings of the Ottoman Empire, however, roasting of the coffee berry was developed, and the resulting coffee bean was more stable. The market heated up, and plantings of C. arabica spread to JAVA and beyond. Eventually, the pleasures of Coffee reached Vienna,and by 1652, the first House dedicated to coffee drinking opened in London.
Coffee Houses spread, and soon catered to special groups like writers, Philosophers and Merchants. Lloyds of London started as a discussion group of traders who were privy to Embarking ships’ Bills of Lading, and enjoyed an economic advantage. Soon the different coffee houses excluded the general public.
The Tastes of the British drinking public was malleable, however. Just as disputes with France caused a switch from wine to gin, the East India Companies plethora of TEA eventually resulted in substantial displacement of coffee drinking by the english tea ritual.
The reverse happened in Revolutionary America. Beginning with the Boston Tea Party, coffee drinking became more popular. By the time of the Civil war, it was unthinkable for Confederate soldiers not to have their ration of coffee.
America is presently the country with the largest coffee consumption. However, the per Capita coffee consumption is higher in a dozen other countries, especially in Scandinavia. Those long, dark winters, with associated increase in seasonal depression meshes well with the STIMULATING VIRTUES OF COFFEE.
Yes, Coffee is stimulating, and its effect can, and often does become ADDICTIVE, as I discovered when I started my Medical Practice. I was drinking three cups of coffee a day and still was tired all of the time, since I was often up at night taking care of my asthmatic patients; I finally decided to quit drinking coffee, and after a full three weeks, started feeling better.
For me, coffee was NOT A SUBSTITUTE FOR SLEEP. I know of at least one Red Bull accolite that disagrees with me, and the NEJM article on the benefits of coffee would seem to support drinking more than one cup of coffee a day.
I currently take about 50 mg. Of caffeine by tablet about every 3-4 days when I am tired in the early afternoon, before 2:30 PM, so as to clear the drug from my system by bedtime. If I use it more frequently, I do not enjoy the same pleasant alertness that less frequent use affords.
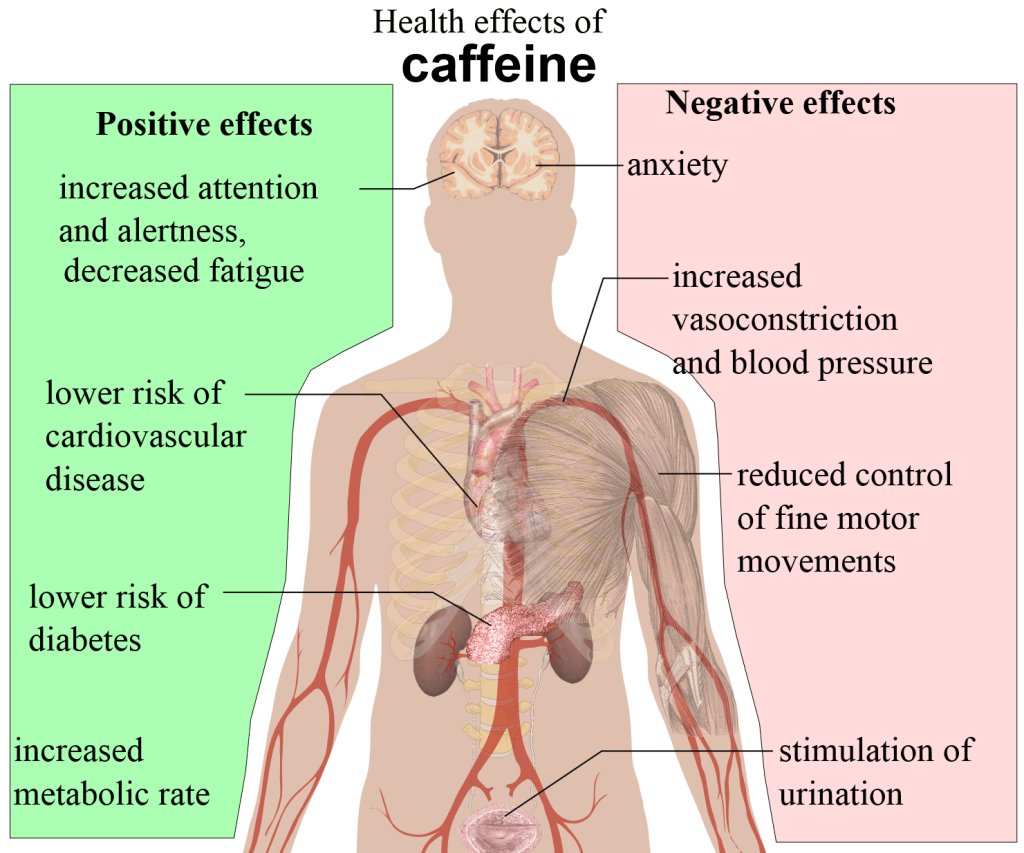
I currently drink a cup of green tea in the morning, which I believe delivers about 20 mg. Of caffeine and some other health benefits as well. Caffeine makes you more alert by competitively blocking the sedative action of Adenosine, which gradually accumulates in parallel with ATP depletion during the course of energy expenditure in the activities of the waking day.
Chemically, caffeine is trimethylxanthine, and is a cousin to the drug theophylline, which was the mainstay of asthma therapy for the first decade or so of my allergy practice. Before theophylline therapy was standardized, a strong jolt of coffee was often used for severe asthma.
Coffee apparently shares with Theophylline the inhibition of Phosphodiesterase, causing the heart to speed up, and lung airways to open. So enjoy your coffee, especially after reading about its health benefits in the recently posted NEJM article.
But be careful about drinking too much. There is rarely such a thing as a ’free lunch” in the worlds of economics and drugs. YES, CAFFEINE IS A DRUG, and the intoxicating aroma notwithstanding, please respect it as such.
“The findings of this study are promising and reinforce what we’ve seen in other studies — fasting diets are a viable option for people who want to lose weight, especially for people who do not want to count calories or find other diets to be fatiguing,” Varady said.
…participants in both daily fasting groups reduced calorie intake by about 550 calories each day simply by adhering to the schedule and lost about 3% of their body weight. The researchers also found that insulin resistance and oxidative stress levels were reduced among participants in the study groups when compared with the control group.
Two daily fasting diets, also known as time-restricted feeding diets, are effective for weight loss, according to a new study published by researchers from the University of Illinois at Chicago.
The study reported results from a clinical trial that compared a 4-hour time-restricted feeding diet and a 6-hour time-restricted feeding diet to a control group.
“This is the first human clinical trial to compare the effects of two popular forms of time-restricted feeding on body weight and cardiometabolic risk factors,” said Krista Varady, professor of nutrition at the UIC College of Applied Health Sciences and corresponding author of the story.
Time-restricted eating brought my weight down from 142 pounds to 136, which is close to what was found on the study; not much, but every pound counts. The improved insulin resistance was reassuring but I am surprised they didn’t find any effects on the HDL, LDL and triglycerides.
The most detailed study on time restricted eating and fasting in general was in the New England Journal of Medicine in December 26, 2019. That excellent article went into all kinds of metabolic pathways that are benefited by fasting.
Good sleep, diet and exercise can be very helpful.
We tested the hypothesis that apathy, but not depression, is associated with dementia in patients with SVD. We found that higher baseline apathy, as well as increasing apathy over time, were associated with an increased dementia risk. In contrast, neither baseline depression or change in depression was associated with dementia. The relationship between apathy and dementia remained after controlling for other well-established risk factors including age, education and cognition. Finally, adding apathy to models predicting dementia improved model fit. These results suggest that apathy may be a prodromal symptom of dementia in patients with SVD.
Cerebral small vessel disease (SVD) is the leading vascular cause of dementia and plays a major role in cognitive decline and mortality.1 2 SVD affects the small vessels of the brain, leading to damage in the subcortical grey and white matter.1 The resulting clinical presentation includes cognitive and neuropsychiatric symptoms.1
Apathy is a reduction in goal-directed behaviour, which is a common neuropsychiatric symptom in SVD.3 Importantly, apathy is dissociable from depression,3 4 another symptom in SVD for which low mood is a predominant manifestation.5 Although there is some symptomatic overlap between the two,6 research using diffusion imaging reported that apathy, but not depression, was associated with white matter network damage in SVD.3 Many of the white matter pathways underlying apathy overlap with those related to cognitive impairment, and accordingly apathy, rather than depression, has been associated with cognitive deficits in SVD.7 These results suggest that apathy and cognitive impairment are symptomatic of prodromal dementia in SVD.
In fact, research on actual cases, as well as models of the pandemic, indicate that between 10 and 20 percent of infected people are responsible for 80 percent of the coronavirus’s spread.
Researchers have identified several factors that make it easier for superspreading to happen. Some of them are environmental.
Poorly ventilated indoor areas seem especially conducive to the virus’s spread – A preliminary analysis of 110 COVID-19 cases in Japan found that the odds of transmitting the pathogen in a closed environment was more than 18 times greater than in an open-air space.
Places where large numbers of people congregate – As a group’s size increases, so does the risk of transmitting the virus to a wider cluster. A large group size also increases the chance that someone present will be infectious.
The longer a group stays in contact, the greater the likelihood that the virus will spread among them – The benchmark used for risk assessment in her contact-tracing work is 10 minutes of contact with an infectious person, though the CDC uses 15 minutes as a guideline.
Some activities seem to make it easier to spread respiratory gunk – Speech emits more particles than normal breathing. And emissions also increase as people speak louder. Singing emits even more particles, which may partially explain the superspreader event at the Washington State choir practice. Breathing hard during exercise might also help the spread of COVID-19.