“We are learning that tactics to avoid dementia begin early and continue throughout life, so it’s never too early or too late to take action,” says commission member and AAIC presenter Lon Schneider, MD, co-director of the USC Alzheimer Disease Research Center‘s clinical core and professor of psychiatry and the behavioral sciences and neurology at the Keck School of Medicine of USC.
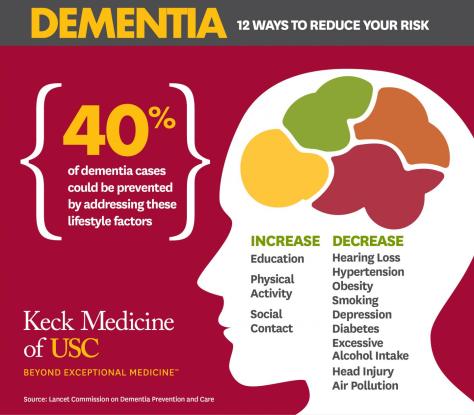
LOS ANGELES — Modifying 12 risk factors over a lifetime could delay or prevent 40% of dementia cases, according to an updated report by the Lancet Commission on dementia prevention, intervention and care presented at the Alzheimer’s Association International Conference (AAIC 2020).
Twenty-eight world-leading dementia experts added three new risk factors in the new report — excessive alcohol intake and head injury in mid-life and air pollution in later life. These are in addition to nine factors previously identified by the commission in 2017: less education early in life; mid-life hearing loss, hypertension and obesity; and smoking, depression, social isolation, physical inactivity and diabetes later in life (65 and up).
Schneider and commission members recommend that policymakers and individuals adopt the following interventions:
Aim to maintain systolic blood pressure of 130 mm Hg or less from the age of 40.
Encourage use of hearing aids for hearing loss and reduce hearing loss by protecting ears from high noise levels.
Reduce exposure to air pollution and second-hand tobacco smoke.
Prevent head injury (particularly by targeting high-risk occupations).
Limit alcohol intake to no more than 21 units per week (one unit of alcohol equals 10 ml or 8 g pure alcohol).
Stop smoking and support others to stop smoking.
Provide all children with primary and secondary education.
Lead an active life into mid-life and possibly later life.
Reduce obesity and the linked condition of diabetes.
Headache has been with us since Neolithic times, and has caused enough distress to induce our ancestors to scrape holes in their skulls, perhaps to let out the causative Evil Spirits, or maybe a subdural hematoma.
When I was a practicing Allergist, i was sent many headache patients by other Doctors.This was, presumably, because the referring physician thought that their patients had “sinus” headaches. In fact, free standing headache does not commonly come from the sinuses.
Most headaches thought due to ‘sinuses” are in fact “vascular “ headaches. The theory of vascular headaches is that the average diet contains many chemicals that are active on blood vessels. Tyramine, degraded proteins and caffeine are examples. These chemicals, working on the blood vessels, cause irritation and pain. It follows,then, that avoidance of these chemicals would relieve the vascular headaches.
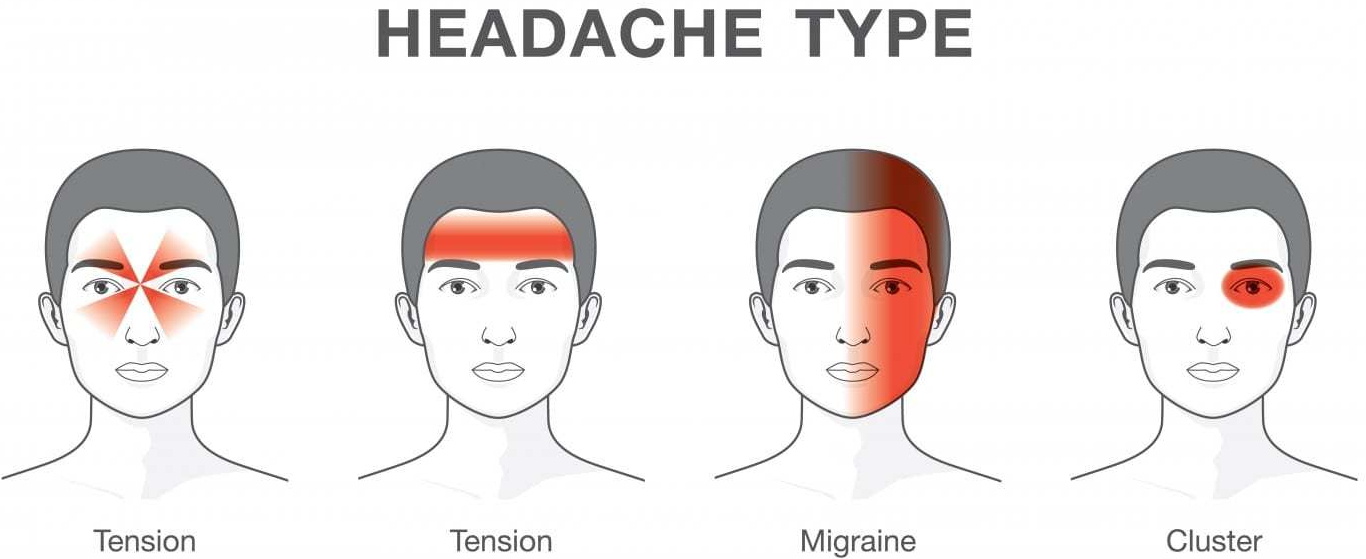
“Vascular headache”, and it’s severe cousin, Migraine headache, is now included under PRIMARY HEADACHE, which also includes Tension headache, and a variety of less common diagnoses. But it is still useful for Treatment, which is why I use the term.
My treatment was a fresh, “health food” diet which avoided preserved foods such as salami, sausages, sauerkraut, leftovers, cheeses, red wine and a variety of other foods likely to have degraded amino acids and Tyramine.
The “mold-free diet” was the published diet closest to listing the suspected foods. The benefit reported from the diet encouraged me to continue recommending it. Vascular headaches are essentially a mild variety of migraine headaches. The foods avoided in the “mold-free diet” are still, after several decades of progress still recognized as migraine triggers.
I encountered only one patient with BRAIN TUMOR in my practice. She had severe, unremitting, gradually increasing headaches over a 4 week period. I called a Neurologist, the type of doctor that treats most severe headaches, who informed me he had NEVER seen a patient with a brain tumor who presented with a headache only, so uncommon it is.
Tension Headaches are milder, and usually can be handled at home. These headaches are usually accompanied by tenderness in the muscles of the back of the neck, or in the temple region, and are brought on by stress.
Hypertension, if extremely high, can cause headache, and can be dangerous, but I never saw a case. Nor did I attend a patient with temporal arteritis, which can also be an emergency.
There are some “red flags” that indicate urgent need for evaluation:
New headache in older patient
New change in headache pattern, or progressively worsening headache
Signs and symptoms of illness ( fever, stiff neck, rash).
Headache triggered by cough or exertion.
Headache in pregnancy or postpartum period
First, worst Headache.
New headaches with AIDS, compromised immunity, or cancer.
Headaches accompanied by mental changes, weakness, or abnormal Neurological signs.
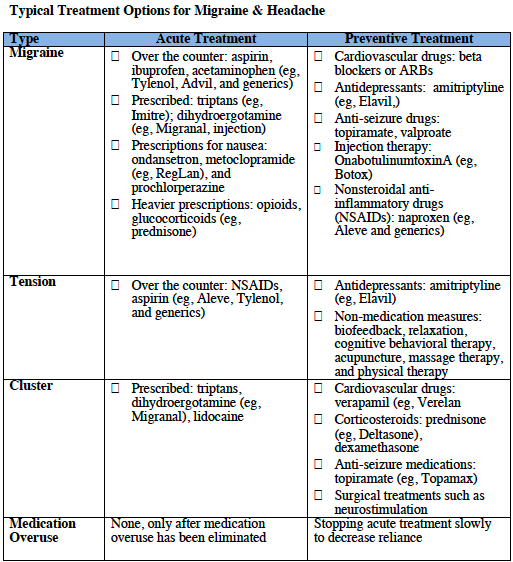
Selective medications are available for some headaches.
Preventative and abortive medications sometimes are helpful for migraine. Antidepressants, tryptans, beta blockers, and corticosteroids are medications best prescribed by specialists.
The tendency to use pain killers, especially narcotics, must be tempered. Frequent use can create additional problems, like ADDICTION. The CAUSE of the headache must be found, if possible, and specifically treated.
Of course, I did find patients with true SINUS HEADACHE, but the headache was accompanied by fever, tenderness over the sinuses, yellow nasal discharge, and other evidence of SINUSITIS, and went away when the infection was treated.
If you have a lot of headaches, and no “red flags” or “risk factors”, you might try a “mold free diet” for a few weeks. Your Nutrition and health would certainly not suffer. And you might have fewer headaches!
Please read the following article for a more complete discussion of this common and annoying problem.
Coffee has a long and colorful history. Billions of cups are consumed daily, and with such a large and passionate audience, I offer you a taste of the aura which abound on the subject of this popular drink.
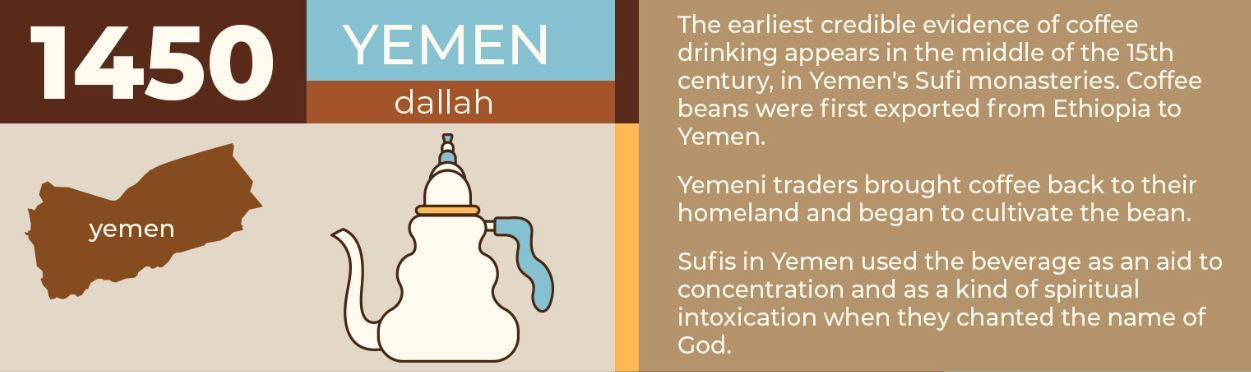
The African story of happy animals galloping around at night after eating some red berries from bushes more than a thousand years is probably a myth. It wasn’t until 15th C. Yemen that the documented history of coffee begins.
The substance that was initially ingested wasn’t even a beverage, but was more like an evil-tasting paste. The reason that it endured was undoubtedly it’s stimulating quality.
The Muslim world proscribed alcoholic beverages, but coffee enabled the faithful to pray all night, and was welcome. The Time taken to bring the berries to market often resulted in spoilage. The cargo had to travel from Ethiopia to the port of MOCHA in Yemen, and by a long Voyage to middle eastern destinations.
With the blessings of the Ottoman Empire, however, roasting of the coffee berry was developed, and the resulting coffee bean was more stable. The market heated up, and plantings of C. arabica spread to JAVA and beyond. Eventually, the pleasures of Coffee reached Vienna,and by 1652, the first House dedicated to coffee drinking opened in London.
Coffee Houses spread, and soon catered to special groups like writers, Philosophers and Merchants. Lloyds of London started as a discussion group of traders who were privy to Embarking ships’ Bills of Lading, and enjoyed an economic advantage. Soon the different coffee houses excluded the general public.
The Tastes of the British drinking public was malleable, however. Just as disputes with France caused a switch from wine to gin, the East India Companies plethora of TEA eventually resulted in substantial displacement of coffee drinking by the english tea ritual.
The reverse happened in Revolutionary America. Beginning with the Boston Tea Party, coffee drinking became more popular. By the time of the Civil war, it was unthinkable for Confederate soldiers not to have their ration of coffee.
America is presently the country with the largest coffee consumption. However, the per Capita coffee consumption is higher in a dozen other countries, especially in Scandinavia. Those long, dark winters, with associated increase in seasonal depression meshes well with the STIMULATING VIRTUES OF COFFEE.
Yes, Coffee is stimulating, and its effect can, and often does become ADDICTIVE, as I discovered when I started my Medical Practice. I was drinking three cups of coffee a day and still was tired all of the time, since I was often up at night taking care of my asthmatic patients; I finally decided to quit drinking coffee, and after a full three weeks, started feeling better.
For me, coffee was NOT A SUBSTITUTE FOR SLEEP. I know of at least one Red Bull accolite that disagrees with me, and the NEJM article on the benefits of coffee would seem to support drinking more than one cup of coffee a day.
I currently take about 50 mg. Of caffeine by tablet about every 3-4 days when I am tired in the early afternoon, before 2:30 PM, so as to clear the drug from my system by bedtime. If I use it more frequently, I do not enjoy the same pleasant alertness that less frequent use affords.
I currently drink a cup of green tea in the morning, which I believe delivers about 20 mg. Of caffeine and some other health benefits as well. Caffeine makes you more alert by competitively blocking the sedative action of Adenosine, which gradually accumulates in parallel with ATP depletion during the course of energy expenditure in the activities of the waking day.
Chemically, caffeine is trimethylxanthine, and is a cousin to the drug theophylline, which was the mainstay of asthma therapy for the first decade or so of my allergy practice. Before theophylline therapy was standardized, a strong jolt of coffee was often used for severe asthma.
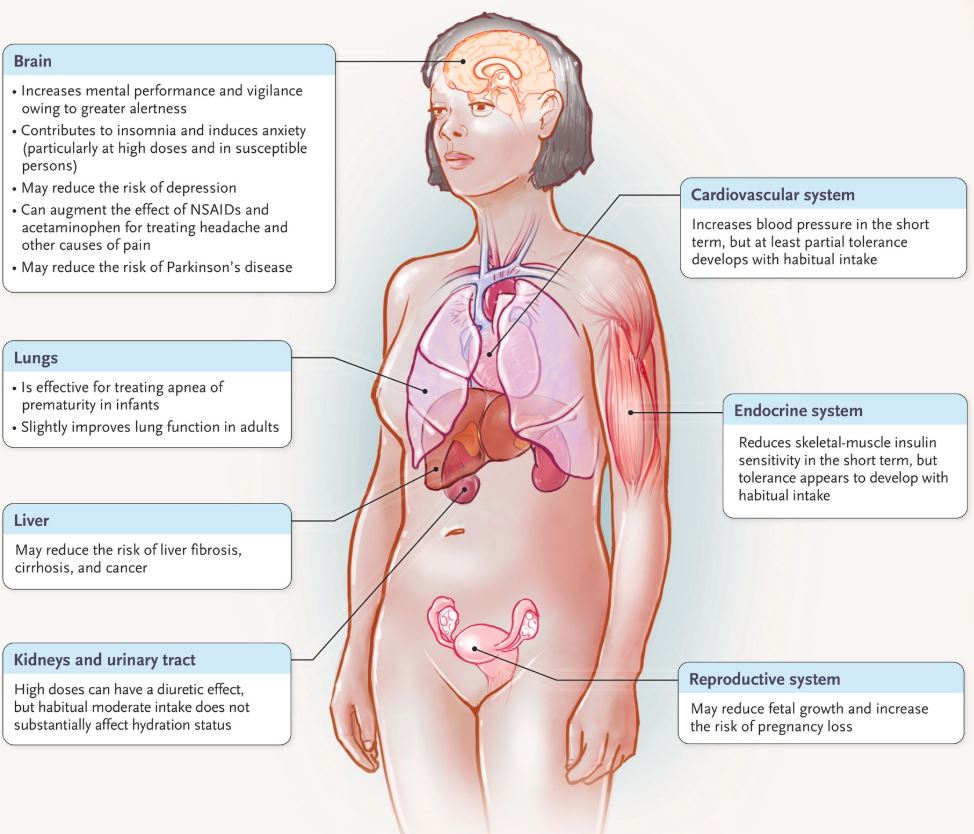
Coffee apparently shares with Theophylline the inhibition of Phosphodiesterase, causing the heart to speed up, and lung airways to open. So enjoy your coffee, especially after reading about its health benefits in the recently posted NEJM article.
But be careful about drinking too much. There is rarely such a thing as a ’free lunch” in the worlds of economics and drugs. YES, CAFFEINE IS A DRUG, and the intoxicating aroma notwithstanding, please respect it as such.
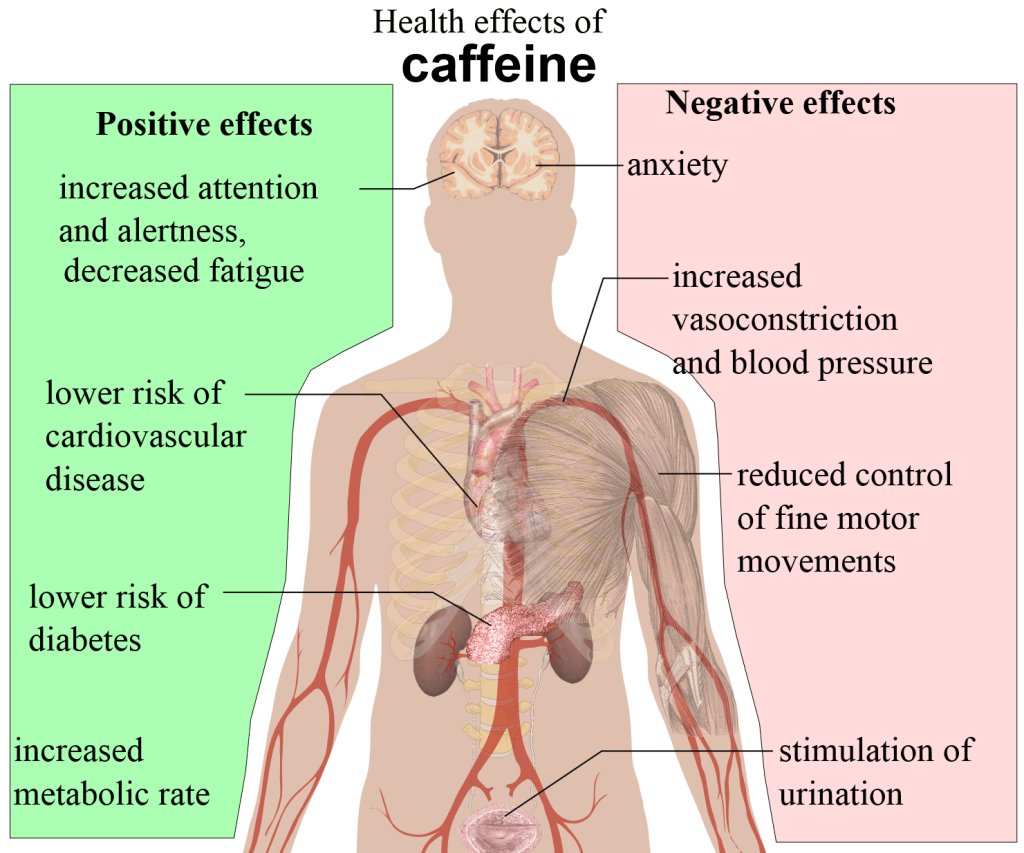
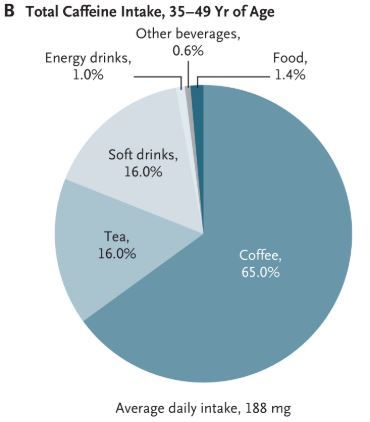
NEW ENGLAND JOURNAL OF MEDICINE (JULY 23, 2020): A large body of evidence suggests that consumption of caffeinated coffee, the main source of caffeine intake in adults in the United States, does not increase the risk of cardiovascular diseases and cancers. In fact, consumption of 3 to 5 standard cups of coffee daily has been consistently associated with a reduced risk of several chronic diseases.
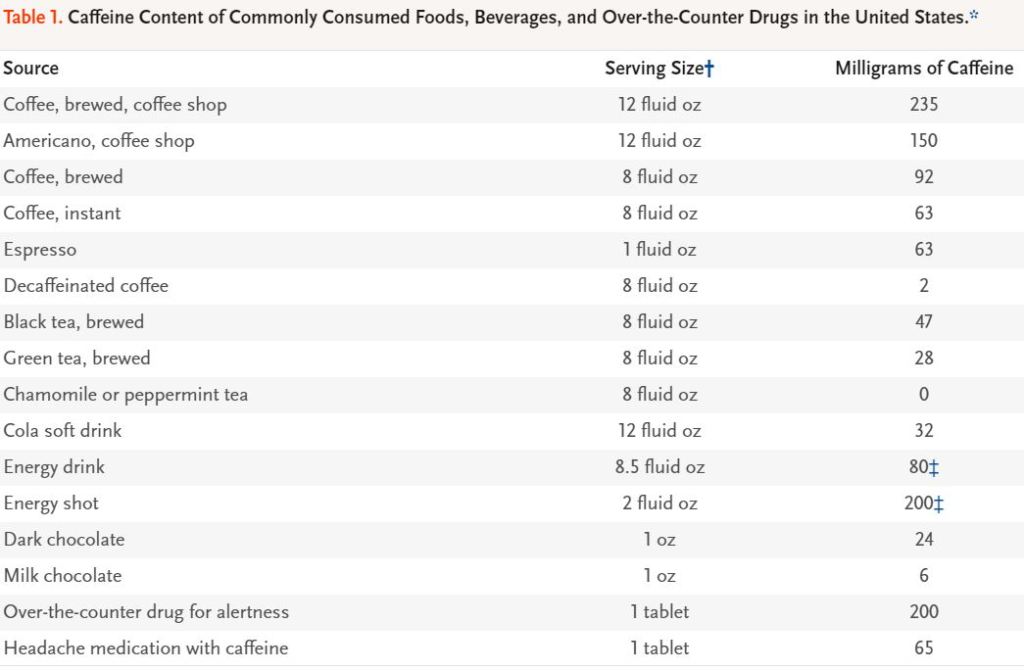
Coffee and tea have been consumed for hundreds of years and have become an important part of cultural traditions and social life.5 In addition, people use coffee beverages to increase wakefulness and work productivity. The caffeine content of commonly used sources of caffeine is shown in Table 1. For a typical serving, the caffeine content is highest in coffee, energy drinks, and caffeine tablets; intermediate in tea; and lowest in soft drinks. In the United States, 85% of adults consume caffeine daily,6 and average caffeine intake is 135 mg per day, which is equivalent to about 1.5 standard cups of coffee (with a standard cup defined as 8 fluid oz [235 ml]).7 Coffee is the predominant source of caffeine ingested by adults, whereas soft drinks and tea are more important sources of caffeine ingested by adolescents,
Our Nervous system is much more than consciousness and free will. Our neural networks automatically go about the job of keeping us alive without entering our awareness- unless it fails to perform.
This is true of our intestinal system, and especially our cardiovascular system. We would not have time for anything else if we had to consciously take each breath, command each heart beat, and for this discussion, open up (dilate) the blood vessels to our brain, and constrict the blood vessels in our legs whenever we stand up.
Our brains demand a constant supply of Oxygen and Glucose in order to perform their complex duties. Between 20% and 40% of the 100 Watts of energy our bodies consume is in our brains.
Whenever we stand up, the force of gravity “wants” to force our blood to our legs and away from our head. Unless that tendency is counteracted, our brains would be deprived of essential factors, and we would all have orthostatic (upright position) hypotension every time we stand up.
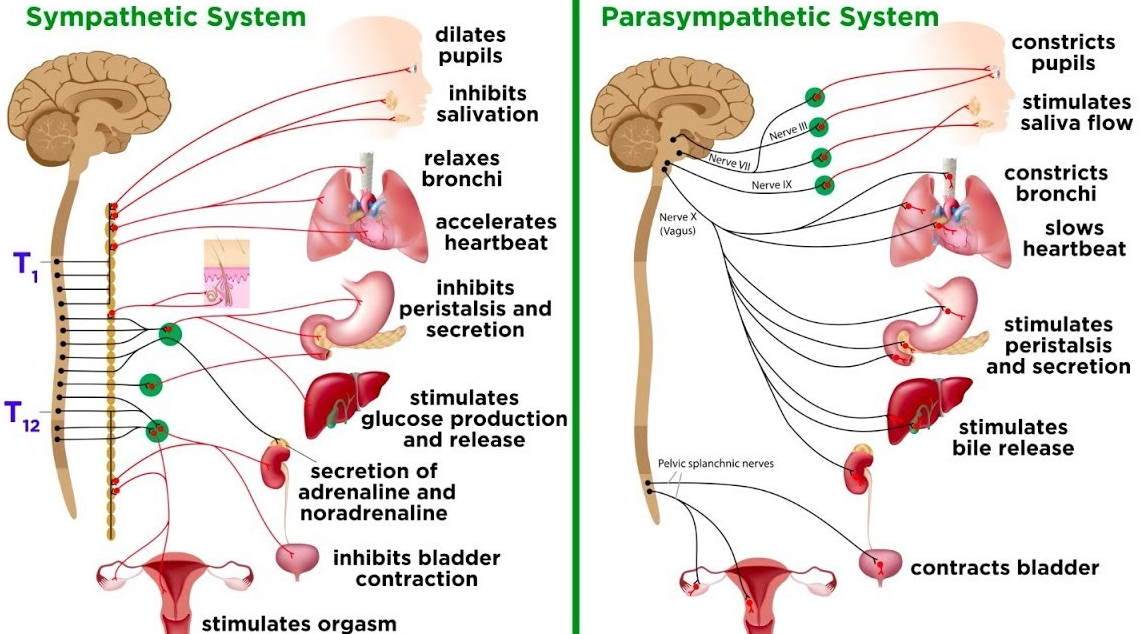
Normally, when the blood pressure drops from ANY CAUSE, receptors near the base of the heart and great vessels signal the sympathetic branch of the autonomic nervous system to cause a speeding up of the heart and a dilation of the blood vessels in the brain. This compensates for the drop in blood pressure, which is determined by the blood flow and resistance to that flow.
The sympathetic nervous system is a reaction to STRESS, to a “flight or fight” decision. In the short term, it is beneficial, or adaptive. You may know the feeling, heart racing, cold hands (due to constriction of blood vessels), breathing rate increases, and sweating.
The asthmatic feels this from a shot of adrenalin, which delivers the sympathetic reaction to the whole body through the blood stream. The musculature of the bronchial tubes are relaxed, improving breathing, and improving the asthma.
What is adaptive in the short haul may be deleterious if it continues, felt as Anxiety if it lasts too long.
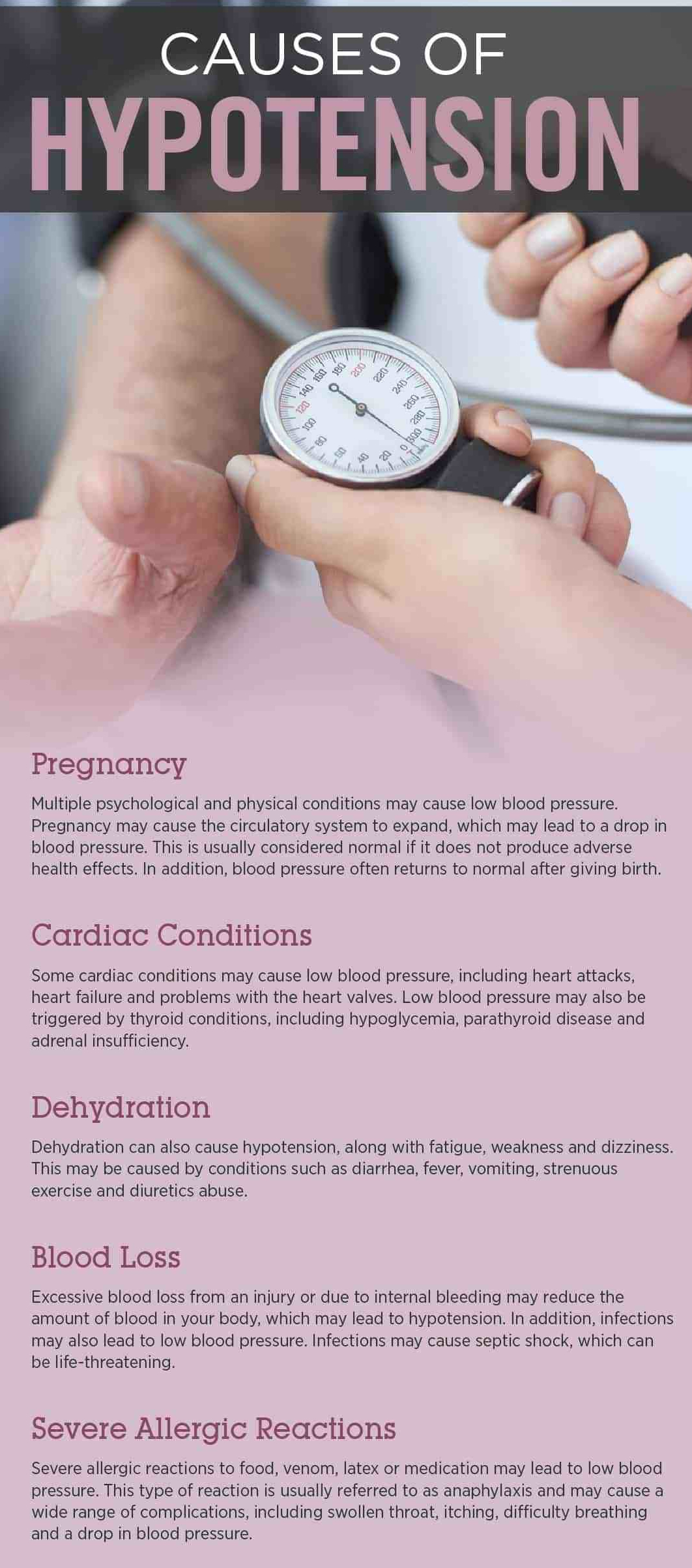
ORTHOSTATIC (postural) HYPOTENSION may be made worse by a variety of other influences, such as an abnormally slow heart, rate, dehydration, blood loss, certain medications and standing still too long.
Since the brain needs both Oxygen and Glucose, High altitude or a low blood sugar will also facilitate faintness. If you have a tendency toward lightheadedness when you stand up, be careful lest you fall and injure yourself.
If you are unable to cope with these spells, a checkup with your Doctor may be in order; perhaps you have an underlying problem, such as with your heart, which is the next subject of discussion.
Falling down is common on both ends of the Human lifespan. Little kids are always falling down, but there isn’t much energy to dissipate, since their mass is small and they don’t have far to fall. Moreover, their bones are pliable.
The Elderly also fall, increasingly, as they age. They have a lot further to fall, and their bones are often brittle and osteoporotic. Injury is quite common, they often break a hip, and may slide into a peogressive deterioration leading to their demise..
Ordinary walking, a “normal gait”, is a very complex activity and requires a lot of information and coordination by the nervous system.
VISION is critical, as you are often navigating through a minefield of stairs, rug edges, slippery objects, lamp cords, tubes and pets. Cataracts may be a problem to be corrected. Multifocal glasses can be a factor.
HEARING can warn of certain hazards or warnings and is important. A FINE SENSE OF TOUCH is required to give you cues as you are walking. Peripheral neuropathy can make walking difficult.
PROPRIOCEPTION, the positional sense of where your extremities are located in space, is a sense we take for granted, but which may deteriorate in time. Proprioception is very important for a normal Gait. The inner ear, with it’s semicircular canals and vestibular apparatus is necessary for proper BALANCE.
Balance can be PRACTICED in a number of ways, like standing on one leg, or merely WALKING a lot. These MULTIPLE SENSES must be COORDINATED by the Thalamus, Corpus Striatum, medulla, Cerebellum, and Cerebral Cortex and instructions sent to the muscles of your Legs, Arms, back and abdomen.
It is mandatory to keep these muscles, your Heart and your body, STRONG and FIT. Factors that make you more likely to have a fall are mostly the reverse of the above, and are called RISK FACTORS.
–Previous Falls are the best predictor. More than 2 or 3 in a year is worrisome.
–Balance Impairment is best treated by practice.
–Decreased Muscle strength. –Visual impairment.
–Polypharmacy (more than 4 prescription Meds), or a Psychoactive drug (look up)
–Gait impairment, Walking difficulty.
–Depression, which is often treated by antidepressants or sleeping pills- Psychoactive drugs.
–Dizziness or orthostatic hypotension, which causes a drop in blood pressure on standing. and a number of other problems, often a function of age.
PREVENTION of falls is of course better than treatment of the resulting INJURY. Working on your HEALTH will help the INTRINSIC causes of falls, and that is what we have been discussing.
Preventing the EXTRINSIC causes of falls means working on: –Improving the household safety by putting in railings, getting rid of throw rugs, clutter, and maybe pets( a good friend went into a downward spiral after tripping over his Dog.
Adjusting or eliminating psychoactive drugs and antihypertensive drugs (which often include the beta blockers which worsen orthostatic hypotension.
Interestingly, VITAMIN D supplements were mentioned in 2 references I saw. Apparently Vitamin D reduces falls by increasing MUSCLE STRENGTH.
Please refer to the following Canadian article for a more complete discussion.
Scientists are working at breakneck speed to develop an effective vaccine for the coronavirus. Their ultimate goal: to immunize enough of the world’s population to reach herd immunity. WSJ explains.
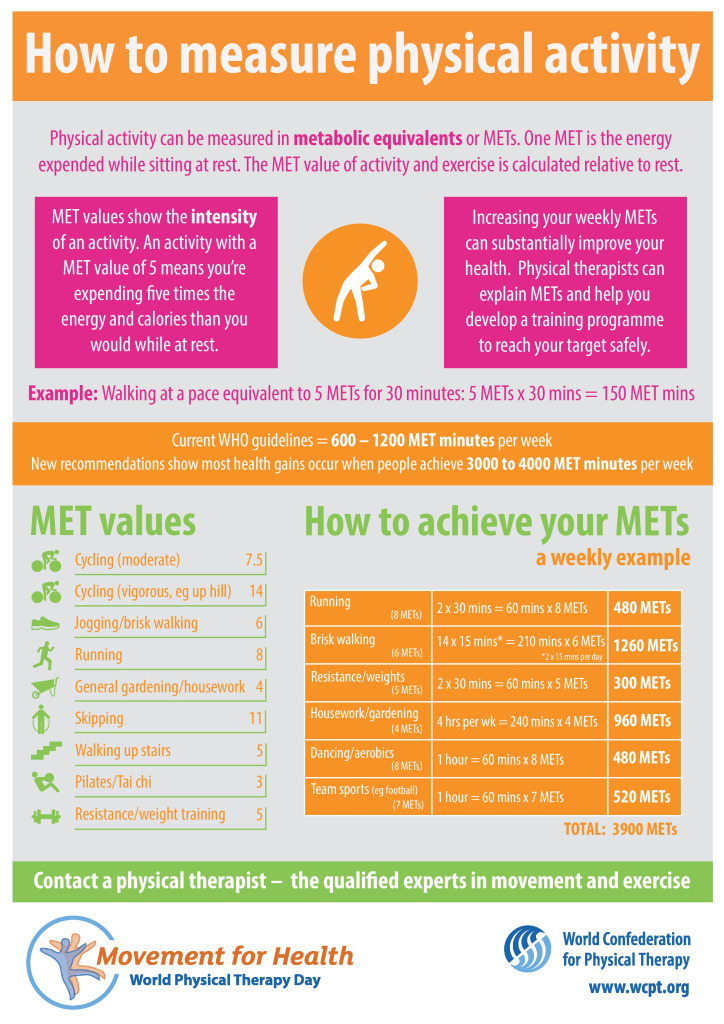
The idea of “METS” as a unit of energy expenditure is interesting and practical. I agree that EXERCISE IS IMPORTANT.
Frank Wilczek, in an article on Dyson Freeman, talked about another unit that I find even more interesting . He proposed that 100 Watts be the unit of energy expenditure. This is (approximately) the energy used in an old 100 Watt incandescent light bulb. It is also the amount of energy used by the “average” human on a 2000 Calorie diet.
Using this unit, the average U.S. Citizen uses 95 units, compared to a 25 unit world average. The suns output is 5 X ten to the fourteenth power, of which 1X ten to the fourth power units lands on earth. Good cocktail information.
I also read that a professional cyclist has an output of only 400 watts, vs. the 14 Mets mentioned in the article.but when I read that the human body is only 20-25% efficient in converting Calories to Watts of Output, 14 Mets made more sense.
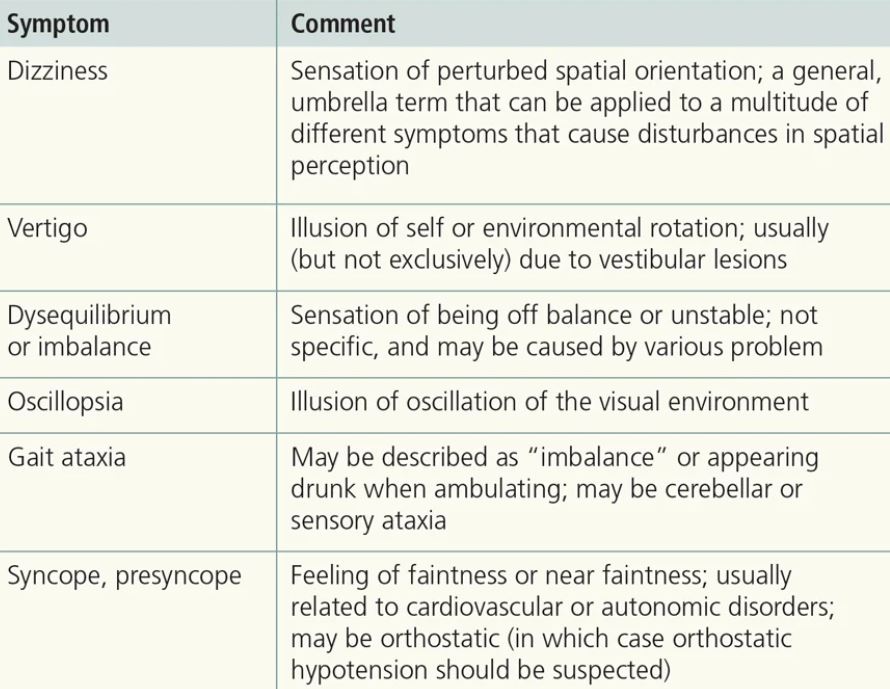
Dizziness, Fainting, Falls, Orthostatic Hypotension, Heart rate and rhythm, Cardiac output and Perfusion, The Autonomic Nervous system,
Falls and Injury are all very interconnected. They all tend to accumulate as we age, but the young are not immune to these conditions. In all of these discussions,
I make the ASUMPTION that you have these conditions in an undramatic, infrequent, moderate way, and are not burdened by Risk factors such as diabetes and hypertension. Stroke is always a worry lingering in the background, and will be discussed at the end of the series.
I will begin with DIZZINESS AND FAINTING. The amazing thing is that we are able to walk upright all day without falling. We can surprisingly lie on our backs, suddenly get up and run away seamlessly, or at least we were able to do these things, most of the time. Our bodies almost magically supply our brains and balance mechanisms with the right amount of blood and nourishment ALMOST all of the time.
Everybody gets dizzy if they spin around enough, and even young people can faint if they stand long enough in one place. Dizziness and fainting is usually considered normal if there is a good explanation. It is when they are too sudden, too severe, last too long, or happen too frequently that we seek medical Help.
Dizziness can mean “lightheadedness” without the room spinning. This is often more concerning than Vertigo, since it more often is due to a lessening of blood flow to the brain. When we get up suddenly from a sitting or lying position, the blood may pool in our abdomen and legs, with consequent insufficient pumping of blood to the brain.
This happens at 1G to civilians, but it takes about 5Gs for young jet pilots to need their “blackout” suits. Instead of blackout suits, we can use support-hose, or even a constricting pants-suit which includes our lower abdomen.
I have also been using a buzzer-timer which reminds me to walk every 10 minutes, to keep me from staying in my comfortable lazy-boy too long. I try to walk rapidly and breathe deeply, and believe this helps keep my body “toned up” and responsive for when I stand up rapidly.
The other way to adapt would be to “baby” my body, and stand up more slowly. There are always the opposite ways to respond: go easy, or push the body and expect it to adapt. If you are worried, your Family Doctor can help you and suggest a path forward .
Perhaps you are overmedicated, need medication, or some tests would help clarify the situation. Vertigo is where the room seems to be spinning. You might be able to tell whether it is spinning clockwise or counterclockwise.
The most common cause is BPPV, or benign periodic positional vertigo, and you can wait it out. Look it up on the internet for parameters. Persistent Vertigo can also be due to inner ear (labyrinth) problems. which an ENT Doctor can address.
For more details, I have included a couple of good articles. A discussion of Falls is next in this series.
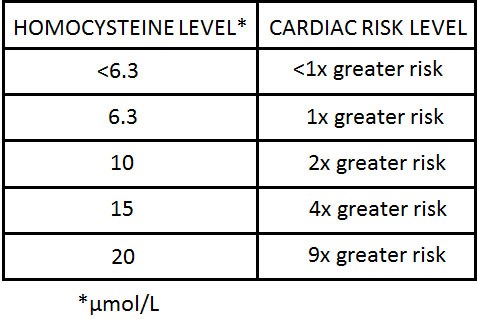
Folic acid has a secure place in my medicine cabinet, and is there for one of the best reasons. In screening for possible causes for heart disease, my doctor ordered a HOMOCYSTEINE LEVEL. The Laboratory value came back elevated.
The treatment given was folic acid. Some background is necessary. Homocysteine is a rather toxic amino acid that can cause heart disease and neurological problems, among other things. If you do not get enough folic acid in your diet with green vegetables, legumes, nuts, eggs and the like (it is hard to be deficient with a good diet), your Homocysteine may become elevated.
You need folic acid to convert Homocysteine to the essential amino acid, Methionine. 10-15% of the population, and up to 30% of older people have elevated Homocysteine levels. Stiffness, slow gait, and heart disease can be related to these elevated levels.
Since I have a good diet, I assume that I have a weak form of an enzyme called Tetrahydrofolate Reductase, which is the rate limiting enzyme in converting Homocysteine to Methionine. A weak enzyme needs more folic acid to do its job. The MDR of Folic acid is 0.4 mg./day. I started supplementing with 1 mg. Daily, without effect on the Homocysteine level. I doubled the dose to 2 mg., and my blood level was still above the upper limits of normal, 15 micromoles/L.. I doubled it again to 4 mg., 2 mg. Twice daily.
Finally my level became normal at 10, This was a decade ago. Recently, I have been doing some research on Alzheimer’s Disease, because a Friend is losing her short term memory. I talked to a neurologist to see if a medical evaluation was mandatory, and found that he has recently BEEN GIVING FOLIC ACID supplements to his AD Patients.
Folic acid deficiency is now being suspected as being a factor in AD! This story is similar to the Vitamin D conundrum. Should I take Vitamin D or not? Am I a “believer” or not. The resolution is easy. You get a Vitamin D blood level.
The lab test will report “normal” if your level is above 20 ng,/ml. I prefer 50, which I achieve with 4000 i.u. Daily supplement. The NFL likes their players to be above 50 to be in best shape. The point is, take a measurement, and then decide.
If you chose to take a Folic acid supplement, I would suggest checking both your Folic acid blood level, and Homocysteine blood level as a reference.
Also, if you take folic (B9) supplements, you should also take extra B12, and B6, since they are involved in the same metabolic pathways. Balance is necessary in metabolism.
–Dr. C
Empowering Patients Through Education And Telemedicine