In my 88 years, I have had at least a dozen medical problems. Some have gone away on their own, some have been removed surgically, and a few have become CHRONIC, lasting for years, ultimately becoming a part of my life.
I have compiled a list of these and other SYMPTOMS & CONDITIONS I have seen as a physician. Over the next year, I will discuss them one by one, appending these vetted articles for further reading.
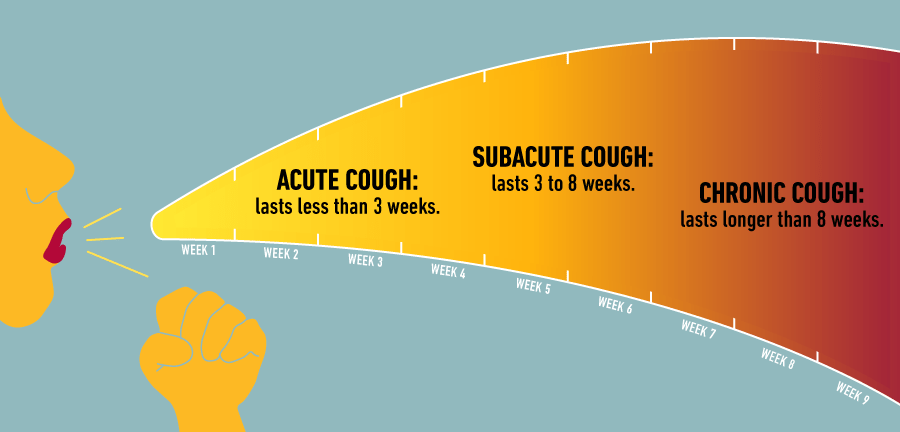
The ‘CHRONIC COUGH’ will be the first discussed.
As an Allergist, I was involved with coughing all of my adult life. If my patients did NOT have asthma, they usually coughed from mucus pouring down the back of their throat (post-nasal drip), from their allergic nasal condition (allergic rhinitis), or sometimes from the associated SINUSITIS drainage.
Asthma was a much more common cause of Chronic Cough for my Patients, sometimes theIr main problem. All asthmatic have a chronic inflammation of their breathing tubes(bronchi), and the resulting BRONCHITIS irritates the airway nerve endings, causing Cough.
Without enough narrowing of the airways to cause wheezing, this is called “cough equivalent asthma”. With the addition of airway narrowing (constriction) to the above situation, ASTHMA results.
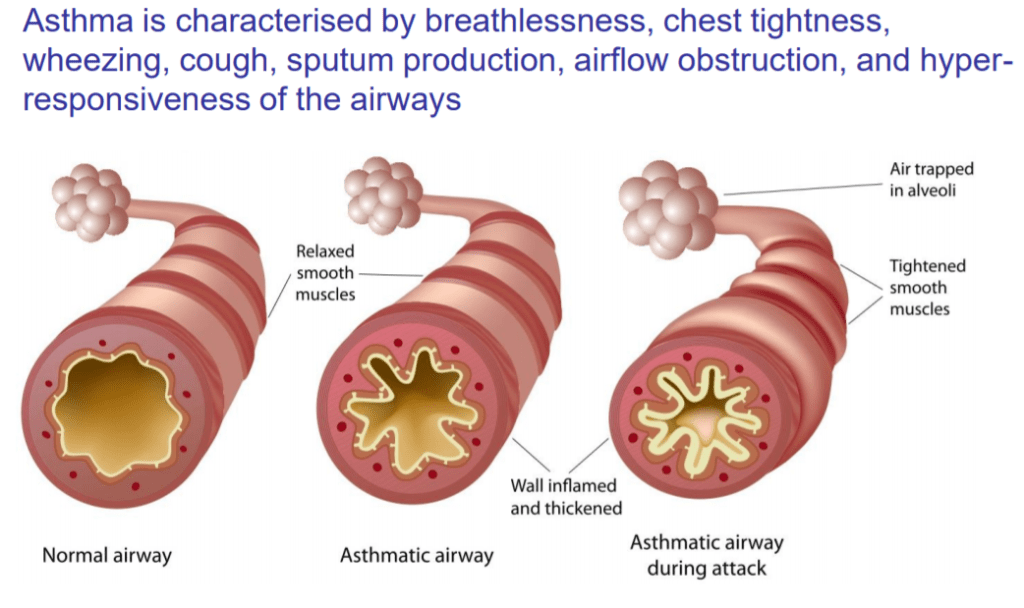
There is added shortness of breath (dyspnea), and the cough becomes the “tight” wheezy cough of full-blown Asthma.
COPD (chronic obstructive pulmonary disease) may be a residue of long-term asthma, but commonly results from cigarette smoking. Where loss of alveolae (air sacs) predominates, dyspnea (shortness of breath) is more common.
Where bronchial tube inflammation is more prominent, mucus and cough result. This cough is useful in clearing the mucus; a USEFUL COUGH (although my Patients did not always appreciate their friend, which could be bad enough to cause hernias or incontinence).
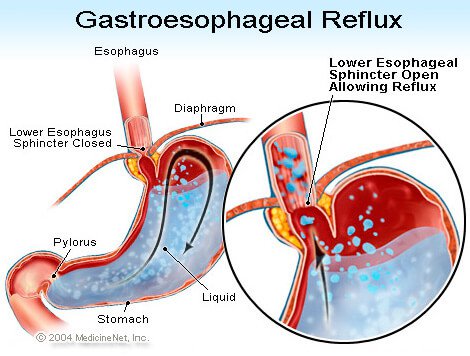
Gastro-esophageal reflux is a chronic condition where stomach contents are not retained in the stomach by the G-E Sphincter ( a type of “purse-string” Gate), but spill(reflux) up, when not restrained by gravity, at NIGHT. The ACIDIC STOMACH CONTENTS burn the esophagus on the way up(heart burn), and are often aspirated into the airways during sleep, causing inflammation and COUGH.
There are many other less common CHRONIC LUNG ( pulmonary) DISEASES (conditions) such as sarcoidosis, bronchiectasis, interstitial pneumonitis, TB, and cancer, that can be diagnosed by imaging (X-Ray, etc.). Heart failure can also cause cough, as can blood pressure medication (ACE inhibitors).
Smoking is an obvious cause; chronic smoking, chronic cough. Smokers know what is causing their cough, and usually don’t bother coming to the Doctor unless they cough up some blood, or develop one of the myriads of diseases caused by their habit.
If you have a chronic cough, check with your Primary Care Doctor, who may refer you to an Allergist or Pulmonologist. The following article will be useful to your understanding of cough, and will provide a LIST OF QUESTIONS the DOCTOR will likely ask you.