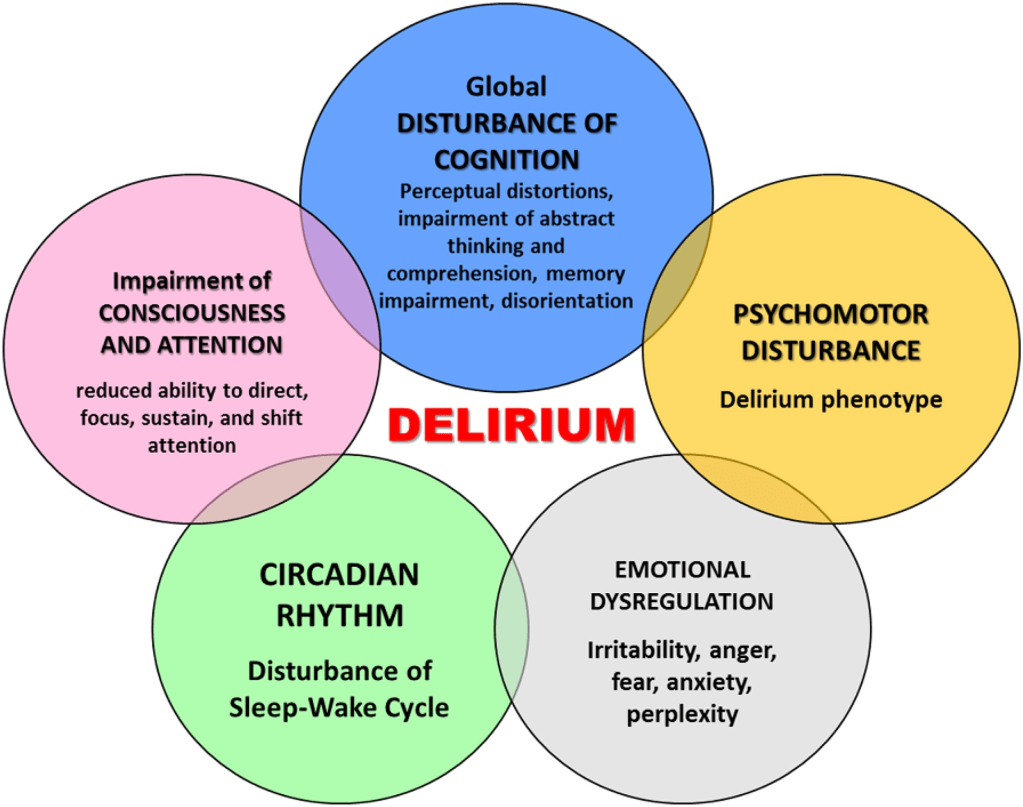
DELIRIUM is a rapidly-developing TEMPORARY DEMENTIA in response to almost any trauma, infection or stress, usually in a hospital setting, with its restrictive, isolating and disorienting environment.
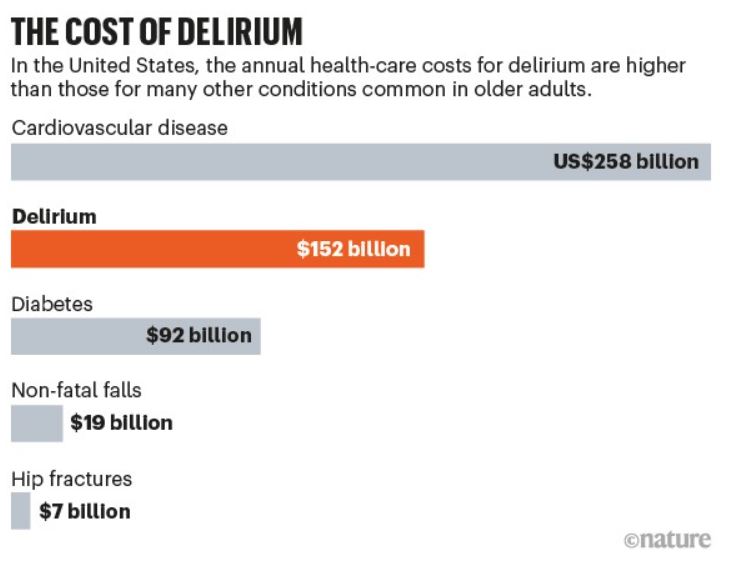
I had little appreciation of the frequency or economic hazard of Delirium before I encountered this infographic. I knew little about the causative mechanisms, and after reading about it, I still don’t know what is going on. But I do know one thing; I don’t want to become delirious and risk its ominous outcome. To improve my odds, I want to keep myself as healthy as possible.
To prevent loss of focus, cognition and memory, challenge the Brain as much as possible. To prevent or restrain infection, support the immune system with a healthy diet. To combat sleep disturbances, practice Sleep Hygiene. To maintain adequate oxygen and nutrient delivery to the Brain, support a healthy cardiovascular-pulmonary system with regular aerobic exercise.
These preventative steps will also postpone the FRAILTY on which delirium feeds. This fuzziness, which afflicts most conditions with PSYCHIATRIC OVERTONES, should not be surprising, since the human Brain, the location of Delirium, is the most complex entity in the known universe.
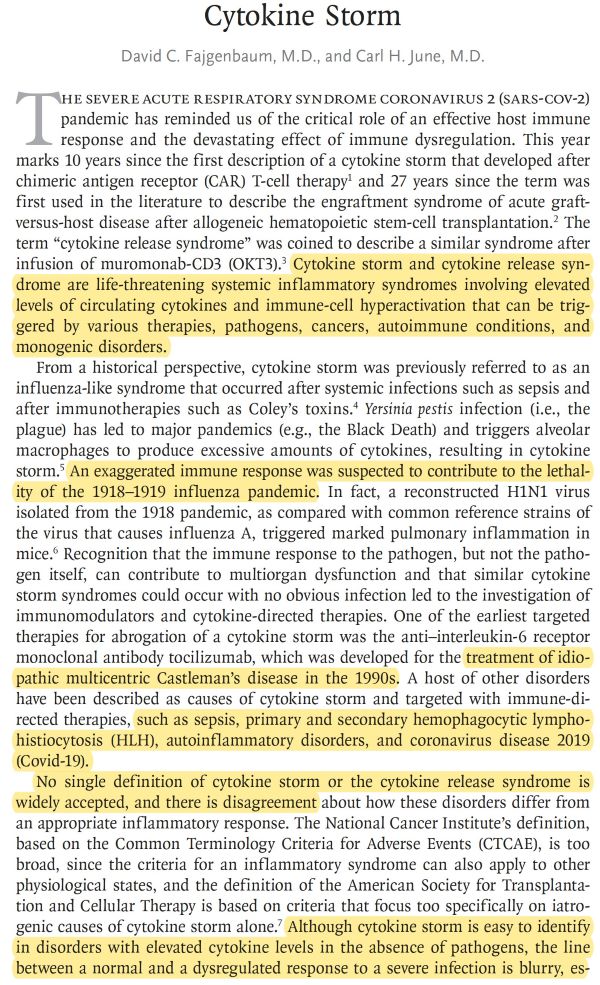
Medical Knowledge of Delirium is still at the descriptive stage, even though it has been a feature of human life since Ancient times. Causation? Excess or Deficiency of most neurotransmitters have been described. To paraphrase “cytokine storm”, which can incidentally cause Delirium, one could call the condition a “neurotransmitter storm”.
Treatment? If the Delirious Patient is on a Psychotropic medication, try stopping it. If not taking such medication, try starting it. The only universal green light is Good general supportive care with IV fluids, oxygen, nutrition, and psychological support, with gentle, regular attention. Please read the accompanying Mayo Clinic article for a more conventional discussion.