

Yearly Archives: 2020

THE DOCTORS 101 CHRONIC SYMPTOMS & CONDITIONS #2: NASAL CONGESTION
Chronic nasal congestion, the constant condition of not being able to breathe through your nose, can be a major problem, interferes with sleep (often via sleep apnea), undermining one of the 4 pillars of health (sleep, diet, exercise and intellectual stimulation). Well, maybe a second one as well, since it is hard to function intellectually when you are sleepy all the time.
Chronic nasal congestion in kids is often due to allergy and associated ADENOID (located at the back of the throat) ENLARGEMENT. Adenoids can cause sleep apnea and pulmonary hypertension, ear infections and sinusitis.
If left untreated, the bones of the face don’t grow properly, and the constricted bony structures can lead to later problems. Nasal polyps can be a factor in nasal airflow blockage, and their removal may benefit the blockage.
If associated with sinusitis and aspirin (aspirin is rarely used in children anymore because if Reyes’ Syndrome) sensitivity, the combination is known as “sampters’ triad. Regrowth of the polyps is common and aspirin desensitization may be helpful.
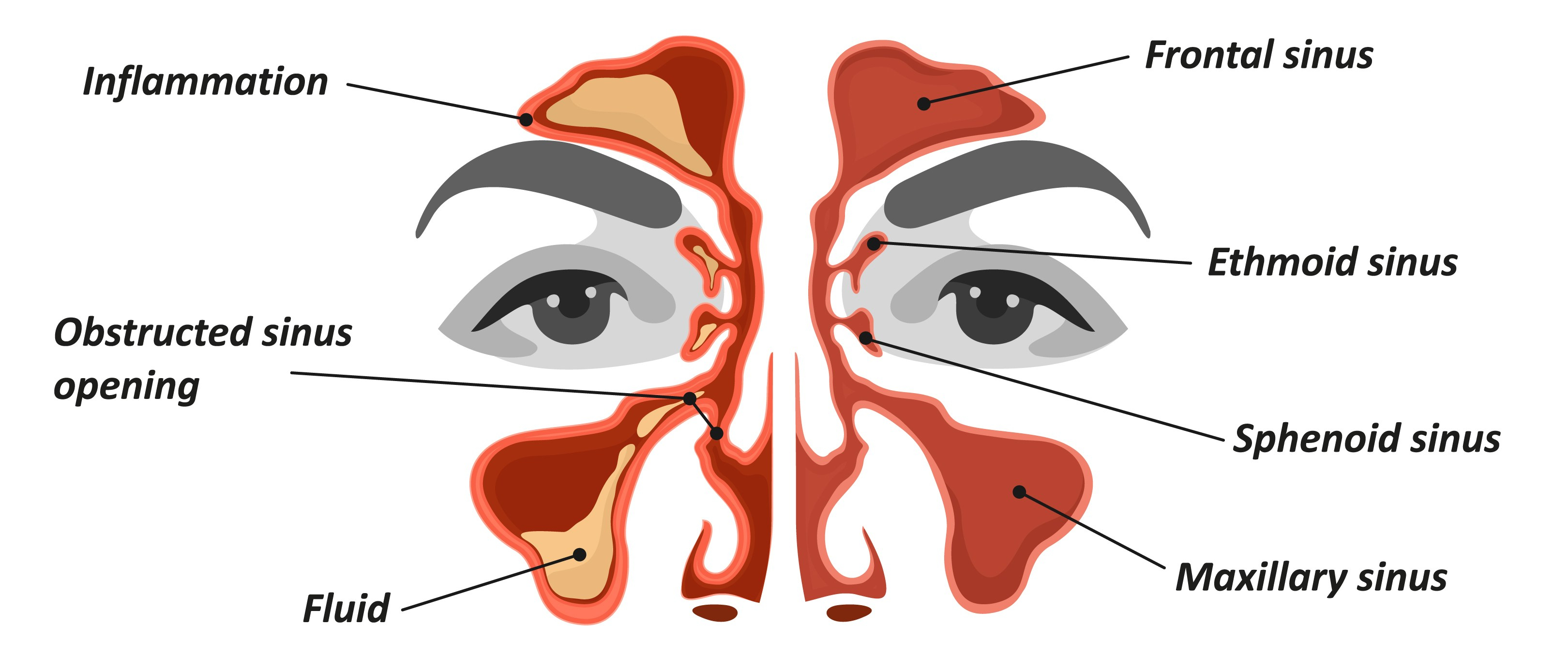
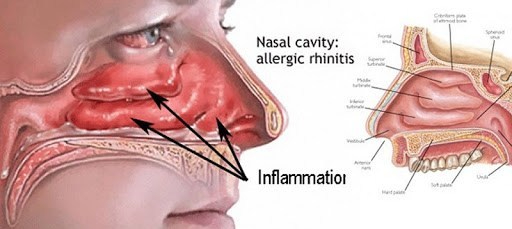
ALLERGIC RHINITIS is treated by avoidance, medication and desensitization. SINUSITIS can cause chronic nasal blockage. Both medical and surgical treatments are useful.
One-sided nasal blockage raises a red flag. One of my young patients had pushed a rock into his nose, which I then removed. Nasal polyps can be on one side, and can be removed, NASAL SEPTAL DEVIATION can cause one-sided nasal blockage, and if severe can be surgically corrected.
The nasal tissues are “erectile tissues” I have a nasal septal deviation to my left side. I SLEEP ON MY SIDE to CONTROL my SLEEP APNEA (more when I get to that subject, which certainly qualifies as a chronic problem), When I sleep on my right side, I don’t breathe as well since my “good side” is down and becomes study.
Those lucky people who breathe freely on both sides, and who sleep on their sides, may possibly be aware that the DOWN SIDE (my good side, above) blocks up. It seems that the nasal tissues are “erectile tissues” body wants to REST one side at a time, and the down side is easier, since gravity pools the blood there.
Nasal tissues are under the control of the autonomic nervous system, decongest (nasal passages are open) with the alarm (fight or flight, “sympathetic”) reaction, and do the opposite (tissues congest, nasal passages close) when the “parasympathetic” takes over after a meal, when you are “vegetating”. in front of the TV

PODCAST: “THE EFFECTS OF HEARING LOSS ON COGNITIVE DECLINE” (JAMA REVIEWS)
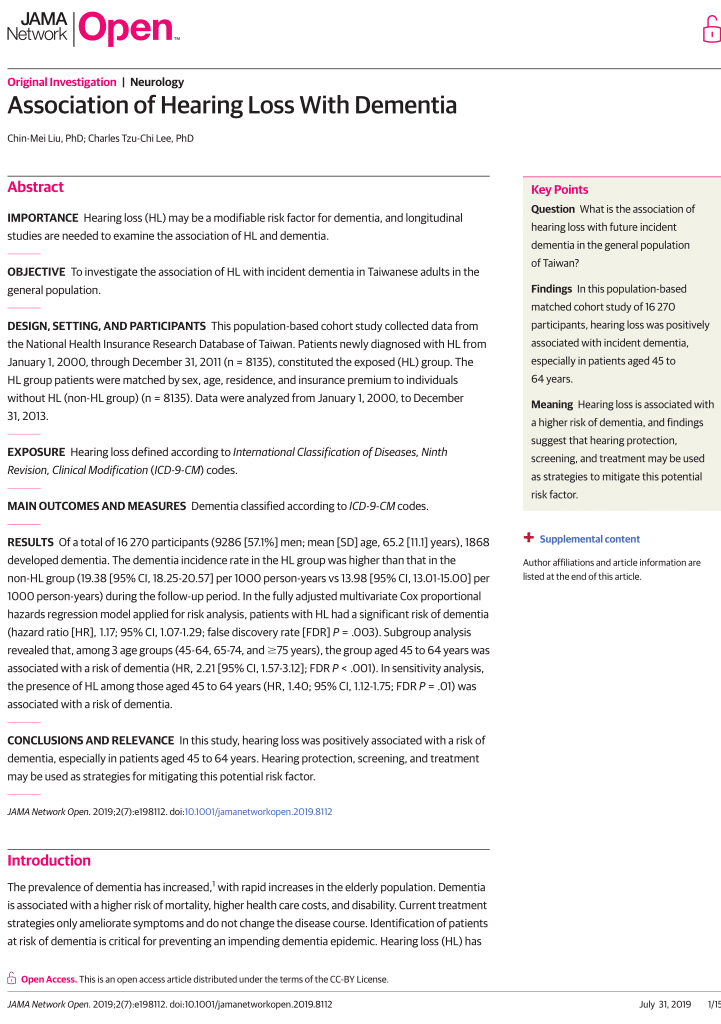
Even limited hearing loss might be associated with cognitive decline. If true, early intervention with hearing aids might help people have better cognitive performance.
Michael Johns III, MD, online editor for JAMA Otolaryngology, speaks with Justin Golub, MD, MS, assistant professor of otolaryngology at Columbia University, whose research has shown that very mild hearing loss can be associated with cognitive disability.
COMMENTARY
Hearing loss and cognitive ability decline together as we age, starting earlier in some people than others.
LIVING A HEALTHY LIFE STYLE-with good SLEEP, DIET, EXERCISE and COGNITIVE STIMULATION -seems to help benefit almost everything, including hearing, while a poor life style, neglecting the 4 Pillars, smoking, and drinking alcohol to excess seems to hasten our aging.
Certain medications, often taken to treat the results of a poor life style, can also harm our hearing.
LOUD SOUNDS (such as AMPLIFIED MUSIC), especially if prolonged, are particularly bad. SOUND POLLUTION contaminates the modern world as much as industries‘ excesses. I would often wear ear plugs to Football games (108 dB on my meter) and even in row 4 of the Symphony.
Once damaged, the delicate HAIR CELLS of our inner ear don’t grow back, although medical science once again is working feverishly to save us from ourselves.
Hearing aids can now be programmed to compensate for our particular pattern of frequency loss.
The premise made in the above article and podcast, that decreased HEARING is accompanied by (and Causes?)decreased COGNITION could be supported by a study demonstrating that Improved hearing restores the cognition. I understand that early results may suggest a cognitive benefit of hearing aids.
But PRESERVING BOTH with healthy living would of course be better- at least in my opinion.
Prevention, unfortunately, is a very hard sell in a world of costly medical treatments, where we are protected from directly confronting those costs by ever-expanding insurance. How about Medical savings accounts?
—Dr. C.
.
THE DOCTORS 101 CHRONIC SYMPTOMS & CONDITIONS #1 – THE “CHRONIC COUGH”

In my 88 years, I have had at least a dozen medical problems. Some have gone away on their own, some have been removed surgically, and a few have become CHRONIC, lasting for years, ultimately becoming a part of my life.
I have compiled a list of these and other SYMPTOMS & CONDITIONS I have seen as a physician. Over the next year, I will discuss them one by one, appending these vetted articles for further reading.
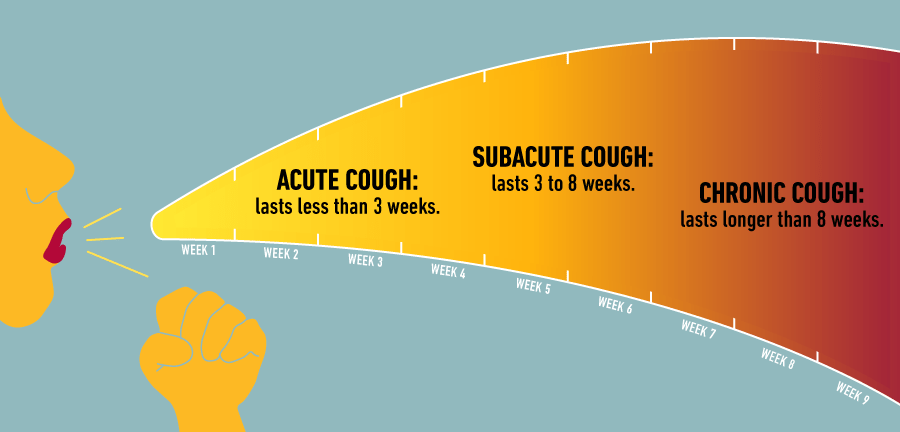
The ‘CHRONIC COUGH’ will be the first discussed.
As an Allergist, I was involved with coughing all of my adult life. If my patients did NOT have asthma, they usually coughed from mucus pouring down the back of their throat (post-nasal drip), from their allergic nasal condition (allergic rhinitis), or sometimes from the associated SINUSITIS drainage.
Asthma was a much more common cause of Chronic Cough for my Patients, sometimes theIr main problem. All asthmatic have a chronic inflammation of their breathing tubes(bronchi), and the resulting BRONCHITIS irritates the airway nerve endings, causing Cough.
Without enough narrowing of the airways to cause wheezing, this is called “cough equivalent asthma”. With the addition of airway narrowing (constriction) to the above situation, ASTHMA results.
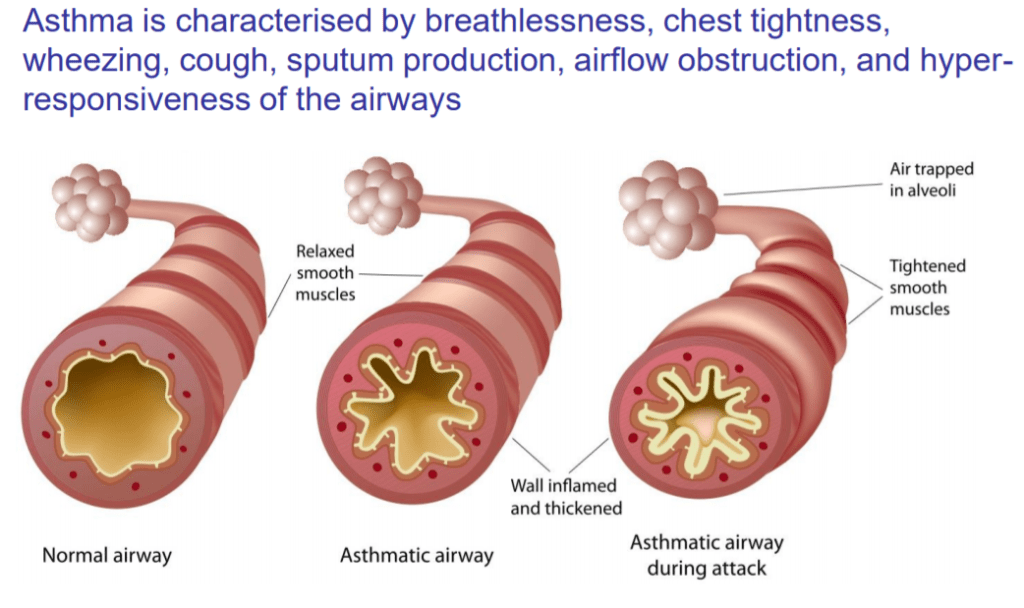
There is added shortness of breath (dyspnea), and the cough becomes the “tight” wheezy cough of full-blown Asthma.
COPD (chronic obstructive pulmonary disease) may be a residue of long-term asthma, but commonly results from cigarette smoking. Where loss of alveolae (air sacs) predominates, dyspnea (shortness of breath) is more common.
Where bronchial tube inflammation is more prominent, mucus and cough result. This cough is useful in clearing the mucus; a USEFUL COUGH (although my Patients did not always appreciate their friend, which could be bad enough to cause hernias or incontinence).
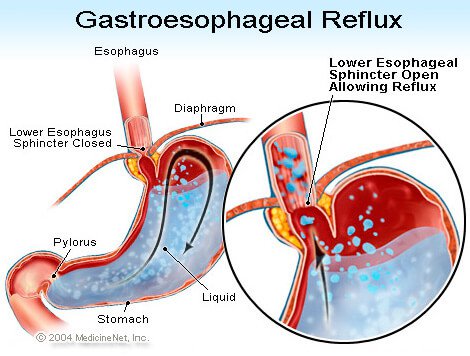
Gastro-esophageal reflux is a chronic condition where stomach contents are not retained in the stomach by the G-E Sphincter ( a type of “purse-string” Gate), but spill(reflux) up, when not restrained by gravity, at NIGHT. The ACIDIC STOMACH CONTENTS burn the esophagus on the way up(heart burn), and are often aspirated into the airways during sleep, causing inflammation and COUGH.
There are many other less common CHRONIC LUNG ( pulmonary) DISEASES (conditions) such as sarcoidosis, bronchiectasis, interstitial pneumonitis, TB, and cancer, that can be diagnosed by imaging (X-Ray, etc.). Heart failure can also cause cough, as can blood pressure medication (ACE inhibitors).
Smoking is an obvious cause; chronic smoking, chronic cough. Smokers know what is causing their cough, and usually don’t bother coming to the Doctor unless they cough up some blood, or develop one of the myriads of diseases caused by their habit.
If you have a chronic cough, check with your Primary Care Doctor, who may refer you to an Allergist or Pulmonologist. The following article will be useful to your understanding of cough, and will provide a LIST OF QUESTIONS the DOCTOR will likely ask you.
—Dr. C.

VIDEOS: THE “ABC’S OF KIDNEY DISEASE” (JOHNS HOPKINS MEDICINE)
ABC’s of Kidney Disease. An educational video to help better the lives of people living with kidney disease and those interested in learning about kidney disease.

VIDEO: “IS TELEMEDICINE THE FUTURE OF HEALTH CARE?”
The coronavirus pandemic has overwhelmed hospitals, physicians and the medical community. That’s pushed telemedicine into the hands of providers and patients as the first response for primary care. Telemedicine isn’t new to the medical community, however it hasn’t been embraced due to insurance coverage, mindset and stigma. Here’s how it works and what it means for the future of health care.
COMMENTARY
The safety and convenience of Telemedicine have been amply illustrated by Covid 19. It’s place in the future of Medicine would seem to be assured.
Once the epidemic is over, however, some sticky details, waved away by fiat during the early days, must be addressed.
Will Payment parity be allowed by the Health insurance companies (And Medicare) be continued? Will cross-border Practice still be allowed by the states. Will more Doctors modernize? Will lawyers (and litigious patients) restrain themselves?
Stay Tuned!
—Dr. C.

OPINION: HEART AND BRAIN HEALTH ARE LINKED FOR LIFE
Your heart and your brain are your two most vital organs, and if you enjoy life, they should be a top priority. These amazing structures are tethered to life-giving support by your arteries, just as the new you was tethered by your ubilical cord.
Life is fragile, hanging by a thread, or an artery. over the span of your life, These arteries can become plugged by fatty deposits called plaques. A healthy life style-SLEEP, DIET and EXERCISE– could slow down or prevent this atherosclerosis.
But everybody should know about the symptoms of HEART ATTACK and STROKE (1) and how to respond if the arteries sustaining your heart or brain become blocked.
You should be familiar with the hospitals in your area. How close are they? What are their capabilities? Are they Class 1 for heart attacks and stroke? Do they have a CATH LAB?
SPEED is important. Within minutes of the BLOCKAGE of an ARTERY to your heart or brain, vital cells start to die. The goal is to remove the blockage as soon as possible. CALL 911 as soon as you have heart attack or stroke symptoms. Don’t be afraid of the ER because of Covid, since almost all now use TELEMEDICINE SCREENING to keep infected patients segregated.
Alas, for many people, such PREVENTATIVE MEDICINE requires too much SELF DISCIPLINE AND CONVICTION. America has an epidemic of OBESITY and an avalanche of tasty FAST FOODS provided by a CONSUMER SOCIETY that is ever-attentive to the latest fads and trends.
DR. C

DOCTORS CALL: “CHRONIC COUGH – DIAGNOSIS AND TREATMENT” (MAYO CLINIC)
On the Mayo Clinic Radio program, Dr. Kaiser Lim, a Mayo Clinic pulmonary and critical care physician, explains chronic cough and how it can be treated.
COMMENTARY
If you have had a cough for more than 8 weeks, the good news is that you don’t have Covid 19. The bad news is that you need a Medical evaluation, tests and imaging to find out what is going on.
COUGH is not a disease, but is a manifestation, a SYMPTOM of a disease.
Your Primary Care Doctor will do a Medical History, an examination and a chest X-Ray which may allow her to DIAGNOSE what disease or problem Is causing the cough, and allow her to treat it.
If you continue to cough, you will be referred to a specialist, such as an Allergist or a Pulmonologist. ENT (sinusitis) and Gastroenterology (GERD) are 2 other medical fields often involved.
Usually blessed relief comes when Chronic Cough is properly diagnosed and treated, but a few Patients continue to suffer, challenging the best of medical care. 2 of my friends continue to cough after Medical School Level evaluations.
Nature continues to hide some of her secrets from Medical Science.
—Dr. C.

TELEMEDICINE 2020: guidance to move forward in a POST-PANDEMIC world
From a John Locke Foundation article (May 13, 2020):
A combination of stay-at-home orders, recommendations from health professionals, and the rollback of restrictive telehealth regulations boosted the use of telehealth.
….with an eye toward the future, the authors offer recommendations for all interested parties to consider moving forward. These recommendations were informed by our research and a stakeholder meeting of industry groups who work with telehealth. These groups included Doctor on Demand, the American Medical Association, and the Center for Connected Health Policy. The paper’s recommendations are as follows:
- Data on COVID-19 telehealth administration and programs must be collected and analyzed.
- Regulatory flexibility should be built into telehealth to accommodate the range of use cases.
- Telehealth services should be utilized for primary care to reduce service redundancies.
- States should be empowered to move away from parity models to reduce the cost of telehealth services.
- Telehealth services should be available to the medically underserved.
- Innovation, privacy, and data security in telehealth services should be the norm.
COMMENTARY
Telemedicine is an “almost perfect” extension of Medical Care for the Covid epidemic (1). As we ease away from Panic, we will not be abandoning distancing, cleanliness, and other personal measures that keep us well. SARS-CoV-2, or the next Pandemic Virus will be lurking in the background.
Likewise, Medicine will always embrace Telemedicine for its’ convenience, safety, and efficiency, if we can overcome the roadblocks discussed in the above article.
One efficiency in particular, discussed in the previous RPA( from Australia) article stood out; the use of Nurse-triage to direct telephone (or someday audio-visual) Patients to the most appropriate destination; ER, Urgent Care, after-hours clinic, or home care.
The Schmidtt-Thompson protocol ( which guides triage) has been used since 1980, having stood the test of time and lawyers. It is available in electronic form, and when fully automated, it should be made available without cost.
Just imagine all of the unnecessary ER visits And Physician Visits potentially saved!
Telemedicine has indeed added convenience and safety in the Era ( it seems like forever) of Covid.
There are many Telemedicine ideas that will still be used when Covid hopefully takes its’ place in the Influenza immunization vial.
—Dr. C.

TELEHEALTH IN AUSTRALIA: “RPA VIRTUAL HOSPITAL” IS A 24/7 PATIENT CARE SYSTEM
From The Guardian (May 12, 2020):
“Now, everybody is on board,” says Dr Teresa Anderson, chief executive of the Sydney Local Health District. “There is not one clinical department across the district that is not providing care virtually.”

What a difference a pandemic makes. Although RPA Virtual Hospital was well into development when news broke from Wuhan in January, pandemic preparations meant it was scaled up far quicker than had been envisaged.
Anderson says RPA Virtual Hospital opened on 3 February with just six nurses. It now has more than 30 nurses, as well as medical and allied health teams, and 600 registered patients. Operating out of Royal Prince Alfred Hospital campus, it functions in many ways like a regular hospital, with a clinical handover, ward rounds, multidisciplinary team meetings and its own governance structures.
The virtual hospital is part of a wider suite of innovations developed at breakneck speed during the pandemic response, which include providing care in rented hotel and apartment accommodation to Covid-19 patients and others in quarantine, thus freeing up hospital beds.
COMMENTARY
The Covid epidemic spurred development of an addition to an already good medical care system.
A group of chronically ill patients were invited into the virtual care system. Nurses are used on initial encounter. They direct the enhanced home care, referrals or hospital care as needed. Electronic devices record the care given.
Hotels are used to quarantine suspected Covid patients, with telemonitoring.
As in America, the Covid epidemic has exposed the excesses of unneeded “elective” surgery, most notoriously surgery for back pain.
We can learn a lot by studying the health care of other countries.
—Dr. C.
