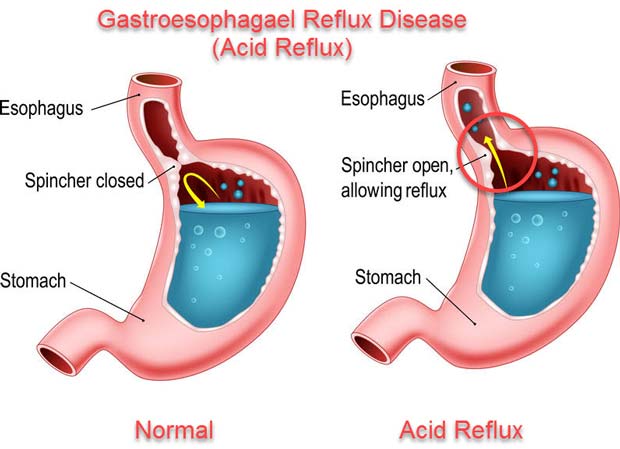
I have been having Heartburn for more than 40 years. The cause of Heartburn is leakage of acid from the stomach, where tissues have evolved to tolerate the highly acidic conditions, into the esophagus, where they haven’t.
The young body has an efficient, functional gate, or sphincter, keeping the food, once swallowed into the stomach, from coming back up. As you eat, you chew your food well to aid digestion. Your taste buds, sensing chemicals in the delicious food, activate saliva.
The salivary enzymes start the digestion of the carbohydrates in the food. If you eat slowly enough, you may be able to appreciate the digestion of tasteless starch, like in bread, into sweet sugar, right in your mouth.
You then swallow the food, which slips past another gate, called the epiglottis, diverting the bolus of food past your windpipe. This gate sometimes does not shut tight, and you choke on the food or drink. The food is then conducted into the highly acidic environment of the stomach.
The stomach evolved to be an acidic, “fiery pit”, inhospitable to any bacteria that came in with the food, thus protecting the stomach from infection. In the old days, there were a lot of bacteria, and the acidity of the stomach was useful, and evolutionarily conserved.
These days, the “fiery pit” tends to be a problem. As you get older, the gate that keeps food in the stomach gets more floppy and relaxed, and allows food to come back up into the esophagus, and sometimes, most often at night when you would rather be sleeping, all the way up to your throat, and is inhaled into your windpipe and lungs in what is called “gastroesophageal reflux”, or GERD.
Even if the food, and acid, doesn’t make it all the way up, and stops at the esophagus, which has not evolved to tolerate acid, you will have “heart burn”. Of course it is not the heart that is burning, but the esophagus, which runs right past the back of the heart as it goes all the way from the throat to the stomach.
When I first developed Heartburn, all that was available was the flavored chalk, Calcium Carbonate, sold as Tums. It works right away, and is a source of Calcium, but can cause trouble, like kidney stones, if you take too much. The relief didn’t last long enough for me, and I had to take more in the middle of the night.
My next medicine was Xantac, a medication that blocks histamine from stimulating acid production in the stomach. The H2 blockers have recently been recalled because of NDMA contamination. I sometimes used H2 blockers like Xantac when my patients would get a bad allergic reaction. In such cases BOTH an H1 blocker like Benadryl, and an H2 blocker are called for.
Zantac was not strong enough for me, and I soon graduated to Prilosec,which directly blocks the secretion of acid in the stomach.

Prilosec was then very expensive, but now is available as the inexpensive GENERIC Medication, Omeprazole. It seems that no medication is without side effects.
Omeprazole, by reducing stomach acid, makes stomach and GI infections more likely, and interferes with the absorption of B12, and Calcium.
If you have had a lot of heartburn over a long period of time, you should check with a Gastroenterologist, who may scope you to rule out Barritt’s esophagus, which can lead to Cancer.
It is interesting that the antacid Tums in excess can cause too MUCH Calcium in the body, and can cause kidney stones and other kidney problems like MAS, and Omeprazole, by interfering with absorption can cause too LITTLE absorption of Calcium, leading to OSTEOPOROSIS.
The best rule is to take as low a dose of ANY medication as possible, preferably none, to understand the possible side effects, and compensate for them if you can.