

In my 88 years, I have had at least a dozen medical problems. Some have gone away on their own, some have been removed surgically, and a few have become CHRONIC, lasting for years, ultimately becoming a part of my life.
I have compiled a list of these and other SYMPTOMS & CONDITIONS I have seen as a physician. Over the next year, I will discuss them one by one, appending these vetted articles for further reading.
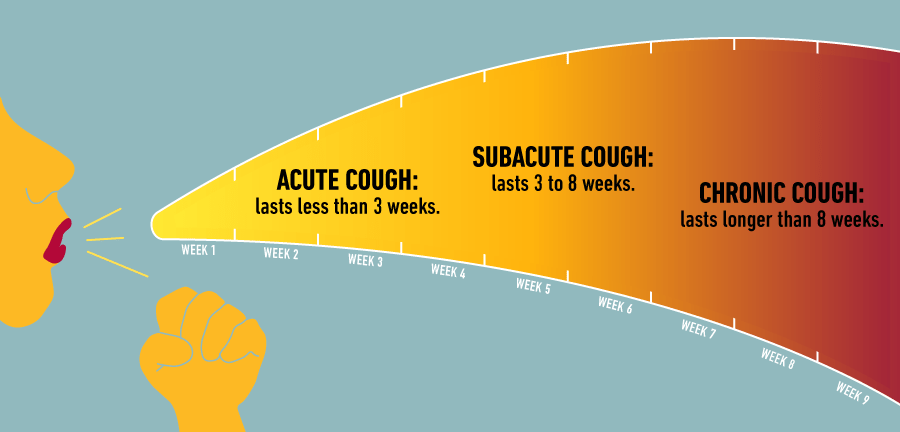
The ‘CHRONIC COUGH’ will be the first discussed.
As an Allergist, I was involved with coughing all of my adult life. If my patients did NOT have asthma, they usually coughed from mucus pouring down the back of their throat (post-nasal drip), from their allergic nasal condition (allergic rhinitis), or sometimes from the associated SINUSITIS drainage.
Asthma was a much more common cause of Chronic Cough for my Patients, sometimes theIr main problem. All asthmatic have a chronic inflammation of their breathing tubes(bronchi), and the resulting BRONCHITIS irritates the airway nerve endings, causing Cough.
Without enough narrowing of the airways to cause wheezing, this is called “cough equivalent asthma”. With the addition of airway narrowing (constriction) to the above situation, ASTHMA results.
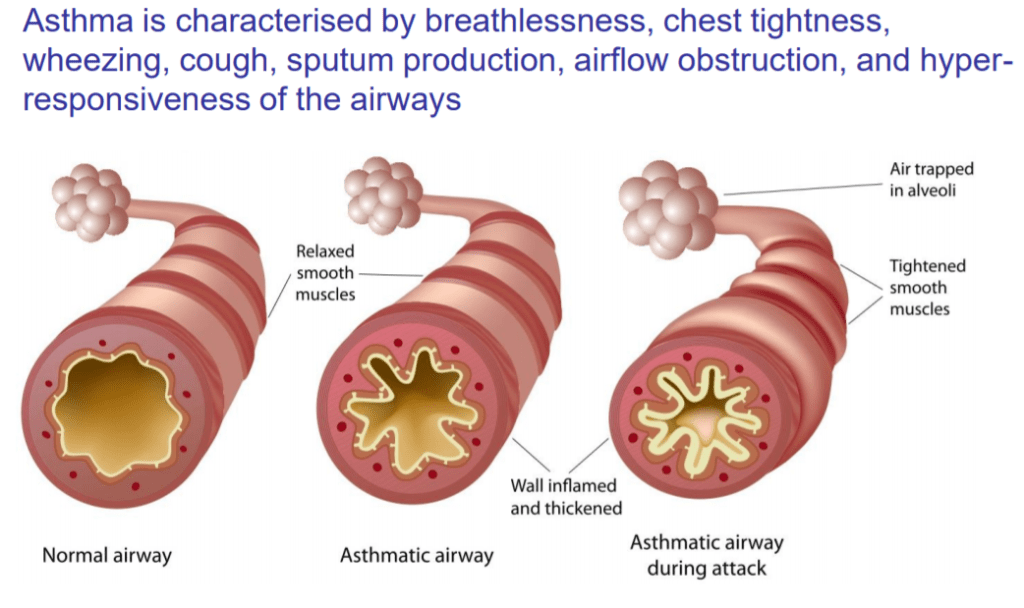
There is added shortness of breath (dyspnea), and the cough becomes the “tight” wheezy cough of full-blown Asthma.
COPD (chronic obstructive pulmonary disease) may be a residue of long-term asthma, but commonly results from cigarette smoking. Where loss of alveolae (air sacs) predominates, dyspnea (shortness of breath) is more common.
Where bronchial tube inflammation is more prominent, mucus and cough result. This cough is useful in clearing the mucus; a USEFUL COUGH (although my Patients did not always appreciate their friend, which could be bad enough to cause hernias or incontinence).
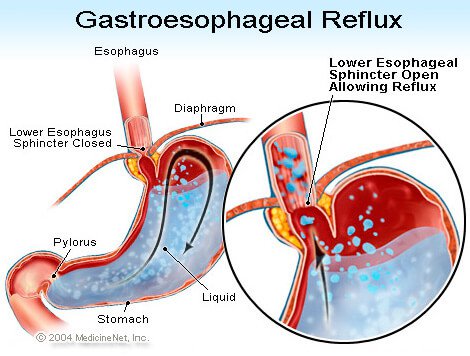
Gastro-esophageal reflux is a chronic condition where stomach contents are not retained in the stomach by the G-E Sphincter ( a type of “purse-string” Gate), but spill(reflux) up, when not restrained by gravity, at NIGHT. The ACIDIC STOMACH CONTENTS burn the esophagus on the way up(heart burn), and are often aspirated into the airways during sleep, causing inflammation and COUGH.
There are many other less common CHRONIC LUNG ( pulmonary) DISEASES (conditions) such as sarcoidosis, bronchiectasis, interstitial pneumonitis, TB, and cancer, that can be diagnosed by imaging (X-Ray, etc.). Heart failure can also cause cough, as can blood pressure medication (ACE inhibitors).
Smoking is an obvious cause; chronic smoking, chronic cough. Smokers know what is causing their cough, and usually don’t bother coming to the Doctor unless they cough up some blood, or develop one of the myriads of diseases caused by their habit.
If you have a chronic cough, check with your Primary Care Doctor, who may refer you to an Allergist or Pulmonologist. The following article will be useful to your understanding of cough, and will provide a LIST OF QUESTIONS the DOCTOR will likely ask you.
ABC’s of Kidney Disease. An educational video to help better the lives of people living with kidney disease and those interested in learning about kidney disease.
From a John Locke Foundation article (May 13, 2020):
….with an eye toward the future, the authors offer recommendations for all interested parties to consider moving forward. These recommendations were informed by our research and a stakeholder meeting of industry groups who work with telehealth. These groups included Doctor on Demand, the American Medical Association, and the Center for Connected Health Policy. The paper’s recommendations are as follows:
COMMENTARY
Telemedicine is an “almost perfect” extension of Medical Care for the Covid epidemic (1). As we ease away from Panic, we will not be abandoning distancing, cleanliness, and other personal measures that keep us well. SARS-CoV-2, or the next Pandemic Virus will be lurking in the background.
Likewise, Medicine will always embrace Telemedicine for its’ convenience, safety, and efficiency, if we can overcome the roadblocks discussed in the above article.
One efficiency in particular, discussed in the previous RPA( from Australia) article stood out; the use of Nurse-triage to direct telephone (or someday audio-visual) Patients to the most appropriate destination; ER, Urgent Care, after-hours clinic, or home care.
The Schmidtt-Thompson protocol ( which guides triage) has been used since 1980, having stood the test of time and lawyers. It is available in electronic form, and when fully automated, it should be made available without cost.
Just imagine all of the unnecessary ER visits And Physician Visits potentially saved!
Telemedicine has indeed added convenience and safety in the Era ( it seems like forever) of Covid.
There are many Telemedicine ideas that will still be used when Covid hopefully takes its’ place in the Influenza immunization vial.

COMMENTARY
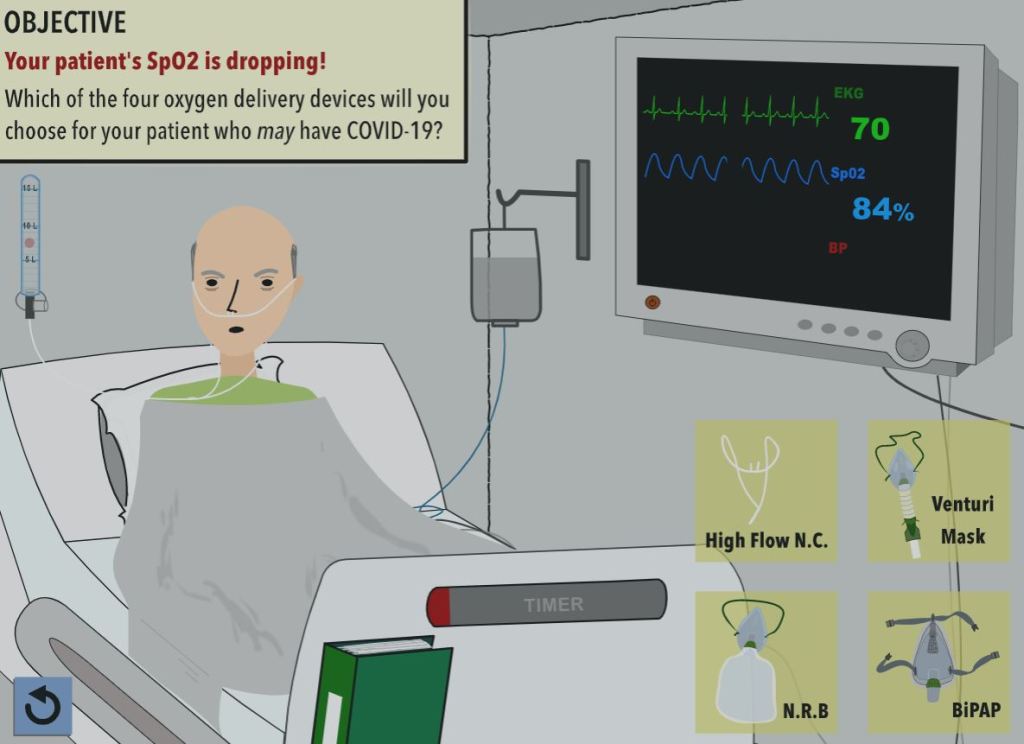
This interactive simulated case of Covid 19 (SARS CoV-2) is remarkable: a unique opportunity to stand in the shoes of a ER Doctor without any risk, except to our egos.
This is meant for doctors, but the intellectually curious Guests of this site might enjoy the experience, especially Doctor Lisa Sanders fans.
The vocabulary is full Medical, and will give a foretaste of the words I will slowly be exploring. I believe that patients should not be intimidated by their lab reports.
I’ll start the vocabulary journey with FERRITIN which is a marker for IRON STORES in the body. You can have too much iron, which is dangerous (iron overload), in which case the ferritin is high.
There was a time when I had too little iron ( was anemic, with a hemoglobin of 8.6, and felt terrible) and my ferritin was low. I now check my ferritin every 6 months to make sure I am taking enough iron to offset my blood loss, which is another story I will tell when I start go through my medicine cabinet and discuss the Meds one at a time.
The reason for testing ferritin in our interactive Covid 19 case was because ferritin is markedly elevated in cases of inflammation/ infection. It is an “acute phase reactant”, and may reflect the “cytokines storm” that may be a contributor to the lethality of Covid 19.
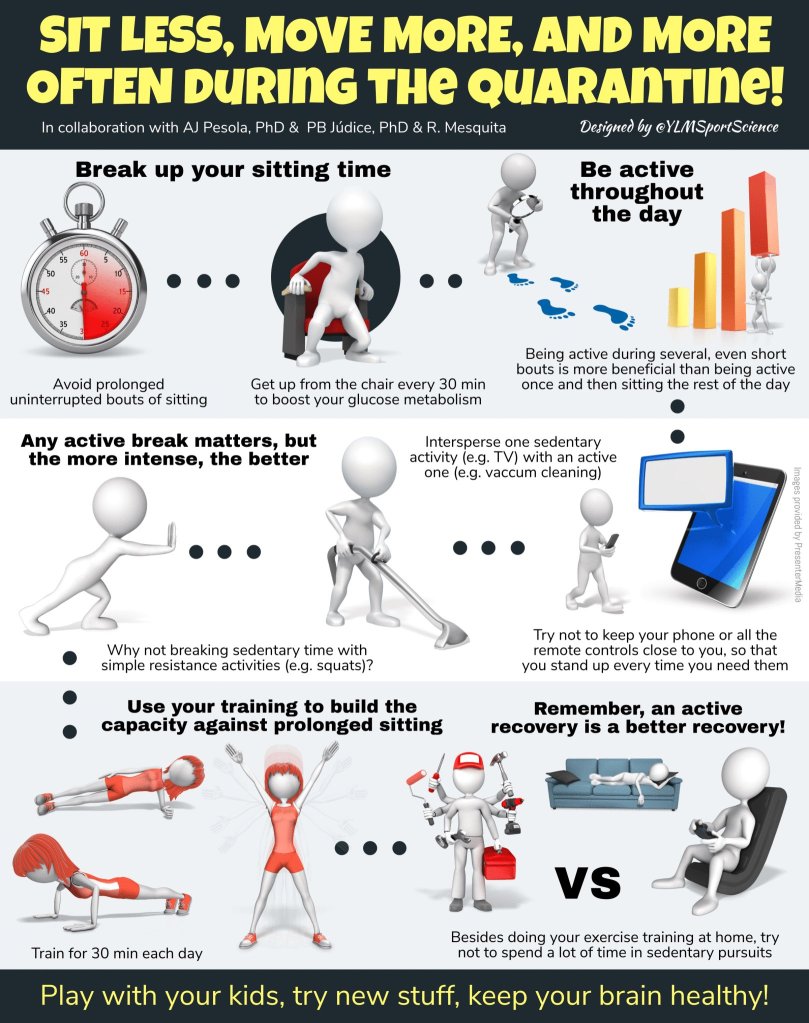
There is another way to benefit from this simulation: the train-wreck of a patient serves as a cautionary tale of what you wish NOT to become. Our present medical profession is so DISEASE oriented. How much better if our society and our medical profession were HEALTH oriented instead.
This video will highlight some of the best practices for healthcare providers when using telehealth to provide services.
More information can be found at http://www.telehealthresourcecenter.org.

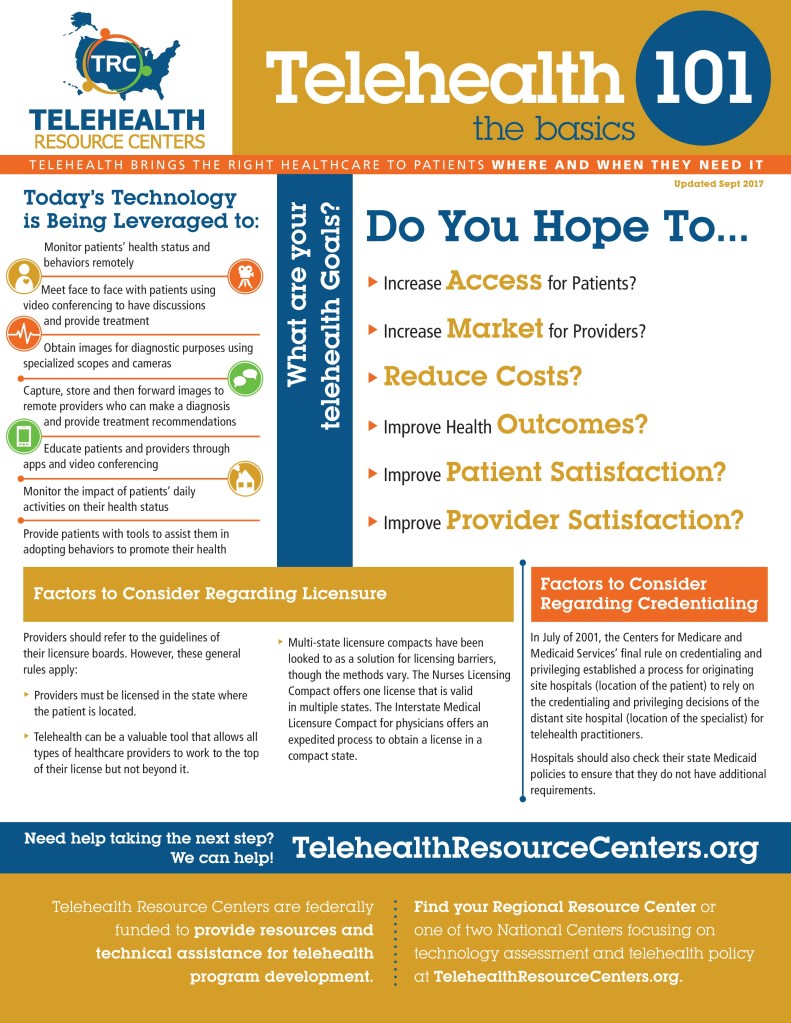
Wondering how to get started with telehealth? Check out the information below to better understand your options.

If screening tools and self-checkers do not lead you to the care or information you are seeking, you can reach out directly to your doctor or health insurance company for options that can help connect you to a provider online. Understanding telehealth
Find out what it is, what to expect during a visit, and what kinds of care may be available. Telehealth during the COVID-19 emergency
Whether you’re looking for health care related to COVID-19 or something else, find out more about how to prepare for the visit. Preparing for a video visit