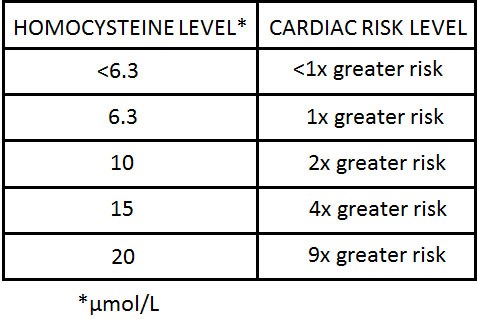
Folic acid has a secure place in my medicine cabinet, and is there for one of the best reasons. In screening for possible causes for heart disease, my doctor ordered a HOMOCYSTEINE LEVEL. The Laboratory value came back elevated.
The treatment given was folic acid. Some background is necessary. Homocysteine is a rather toxic amino acid that can cause heart disease and neurological problems, among other things. If you do not get enough folic acid in your diet with green vegetables, legumes, nuts, eggs and the like (it is hard to be deficient with a good diet), your Homocysteine may become elevated.
You need folic acid to convert Homocysteine to the essential amino acid, Methionine. 10-15% of the population, and up to 30% of older people have elevated Homocysteine levels. Stiffness, slow gait, and heart disease can be related to these elevated levels.
Since I have a good diet, I assume that I have a weak form of an enzyme called Tetrahydrofolate Reductase, which is the rate limiting enzyme in converting Homocysteine to Methionine. A weak enzyme needs more folic acid to do its job. The MDR of Folic acid is 0.4 mg./day. I started supplementing with 1 mg. Daily, without effect on the Homocysteine level. I doubled the dose to 2 mg., and my blood level was still above the upper limits of normal, 15 micromoles/L.. I doubled it again to 4 mg., 2 mg. Twice daily.

Finally my level became normal at 10, This was a decade ago. Recently, I have been doing some research on Alzheimer’s Disease, because a Friend is losing her short term memory. I talked to a neurologist to see if a medical evaluation was mandatory, and found that he has recently BEEN GIVING FOLIC ACID supplements to his AD Patients.
Folic acid deficiency is now being suspected as being a factor in AD! This story is similar to the Vitamin D conundrum. Should I take Vitamin D or not? Am I a “believer” or not. The resolution is easy. You get a Vitamin D blood level.
The lab test will report “normal” if your level is above 20 ng,/ml. I prefer 50, which I achieve with 4000 i.u. Daily supplement. The NFL likes their players to be above 50 to be in best shape. The point is, take a measurement, and then decide.
If you chose to take a Folic acid supplement, I would suggest checking both your Folic acid blood level, and Homocysteine blood level as a reference.
Also, if you take folic (B9) supplements, you should also take extra B12, and B6, since they are involved in the same metabolic pathways. Balance is necessary in metabolism.







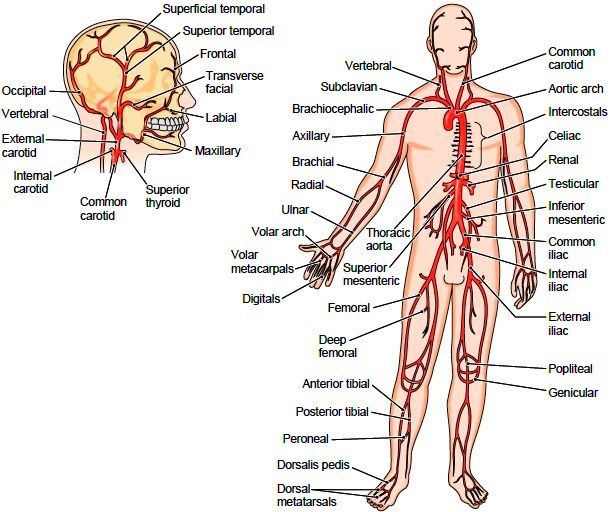
 whether he could have other areas of arterial blockage. His doctor then listened to his neck and discovered a bruit (noise) in the carotid artery, after which he had a Carotid endarterectomy.
whether he could have other areas of arterial blockage. His doctor then listened to his neck and discovered a bruit (noise) in the carotid artery, after which he had a Carotid endarterectomy.