From Fast Company article (June 26, 2020):
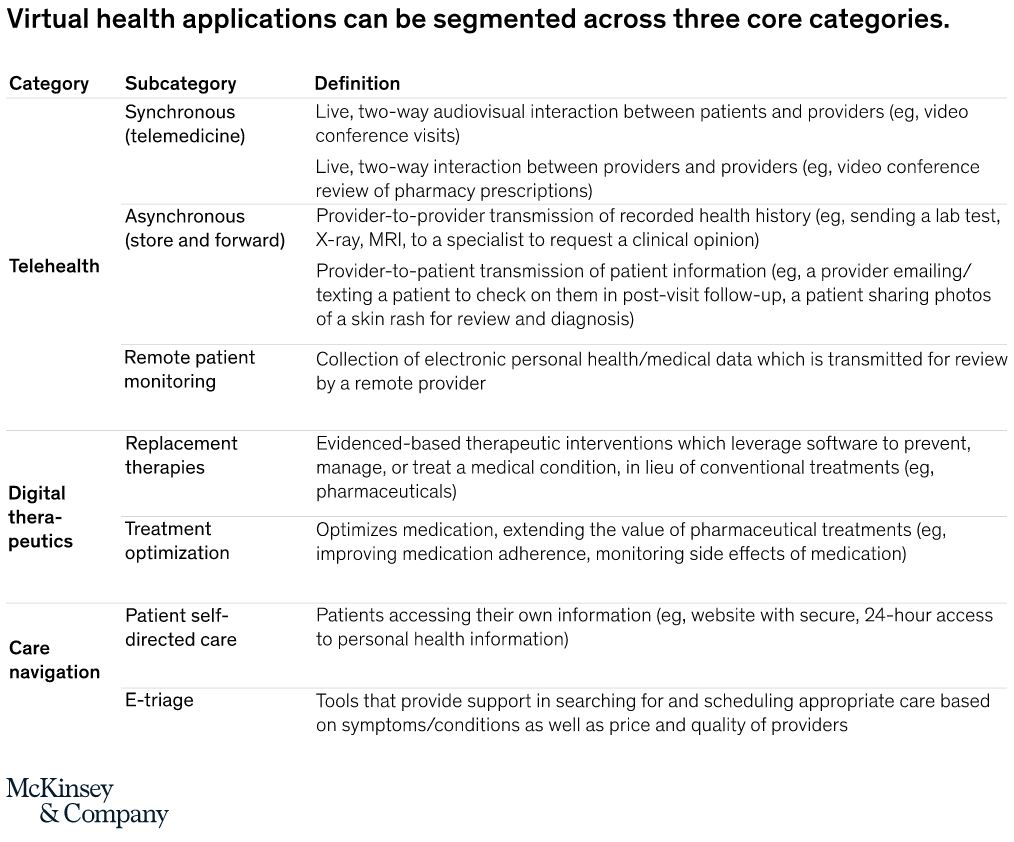
An increasing number of hospitals are now equipping emergency vehicles to treat stroke patients while en route to the ER. UCHealth is a health system in Colorado that has a tricked-out ambulance, the Mobile Stroke Treatment Unit. A neurologist at the hospital is connected wirelessly through telehealth to the vehicle. First responders’ gear includes portable CT scanners and tPA.
Currently, there are also more than two dozen telestroke networks in the United States. At the hub of each is a large hospital with on-call neurologists, and broadband that connects the hospital directly to satellite hospitals and clinics. There’s always a neurologist on call to guide the smaller hospital staffs’ treatment of a stroke patient.
When I had a stroke five years ago at 10:20 on a Saturday night, telehealth saved my life. At the time, only 3% to 5% of people in the United States were able to get the “clot-busting” drug called tPA in time to avoid brain damage.
In addition to offering telestroke capabilities, healthcare providers should equip emergency vehicles with portable ultrasound devices and defibrillators. Rural communities can consider strategically deploying high-powered wired and wireless hotspots in case patients need immediate medical attention while still en route to the hospital. Following natural disasters such as earthquakes or floods, mobile hotspots configured for telehealth could be helicoptered into isolated communities.
COMMENTARY
SPEED is especially important when a blood clot blocks an artery servicing an important organ. Our Heart and BRAIN top the list of vital organs. TELESTROKE showcases Telemedicine at its best.
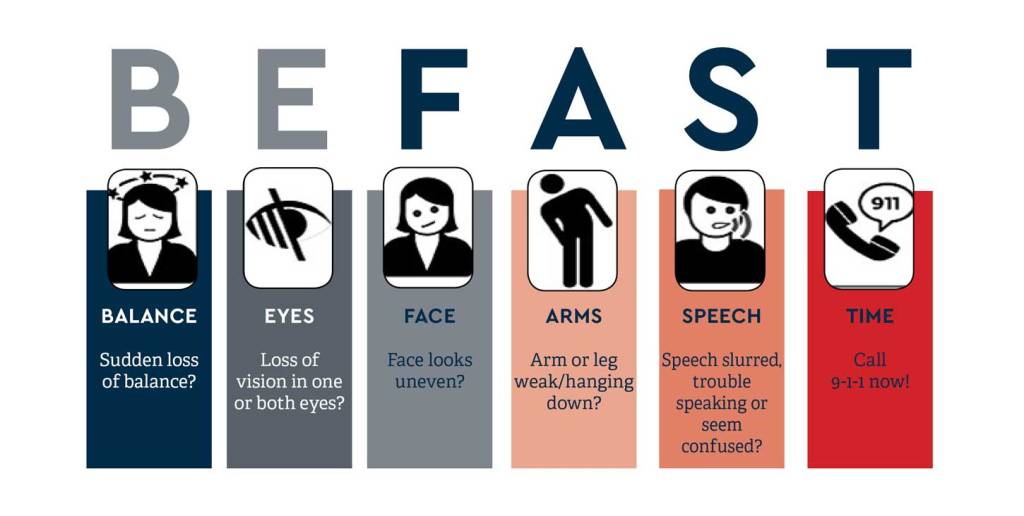
RECOGNITION of a stroke is a weak link in the chain of prompt Brainsaving treatment, and a Mnemonic helps.
—Facial assymetry or drooping
—Arm or leg weakness on one side
—Speech disturbance
—Time is all important
FAST is a good mnemonic, and adding B for balance and E for Eye, or vision loss, for BEFAST gives 2 more parameters to think about.
Living alone adds to the challenge, so be as focused as you can. I was interested to hear that some TELESTROKE ambulances are adding mobile CT and drug (tpa) capabilities, in addition to TELECONFERENCING with a NEUROLOGIST. Treating a stroke within 15 minutes is becoming a possibility.
So particularly if you have risk factors such as hypertension, diabetes or obesity, be on the alert for symptoms of stroke.