One of my previous posts, “bad breath”, was so well received that I am emboldened to deal briefly with another important, if politically incorrect, topic; Constipation.
I have anemia, and take regular IRON, which produces constipation. A high fiber diet solved it. My bones have also been thinning over the years into Osteopenia, a deficiency of Calcium. I Increased my calcium intake with some CALCIUM citrate powder, and developed one of the worst episodes of Constipation I have ever had, in spite of my high fiber diet.
Stopping the Calcium leaves me with the osteopenia worry, but was a great relief. Many other medications can cause constipation. Ask your Pharmacist for a list.` Hypothyroidism, and a variety of autoimmune, intestinal and neurological conditions have constipation as a symptom.
As I struggled with something that should be automatic, I worried about possibly pushing out a hernia, ballooning out one of my colonic diverticula, or developing hemorrhoids. These are all complications of constipation, not to mention the big waste of time. Regularity is much to be desired.
If you have regular SLEEP and EXERCISE a low Calorie density, high fiber diet, and are not taking a lot of drugs and supplements, you most likely don’t have constipation. If you have constipation, you might consider examining your sleep, diet, exercise and medications. If you don’t want to change your habits and medication, try METAMUCIL and drink lots of WATER.
Old age is an inevitable condition if you are lucky enough to live a long life. Middle aged people say it begins at 70 years of age. According to an Elysium survey of people 40 and older, the average American FEELS old for the first time at age 47 years.
In the distant past, 50 was CONSIDERED to be old. The generally better conditions and Medicine of modern times keeps extending LIFESPAN, if not always HEALTHSPAN. Old age is certainly a Condition, and it is for sure Chronic, thereby qualifying for inclusion, but is it a Disease?
It is not considered a disease by the authorities, and so it doesn’t gather research funds like it should. What exactly IS old age? Being 88 Years old, and a physician, I feel qualified to comment. Old age is a collection of past accidents and sports injuries plus complications of past illnesses engrafted on a gradually deteriorating body.
Where does Obesity and Metabolic syndrome fit in this rubric? The Plague of our time fits in the disease category. It is definitely preventable, although with difficulty. Please search past postings for more information on this topic.
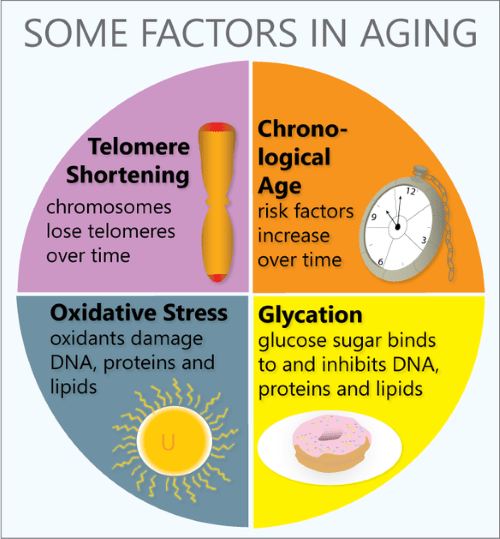
In what way does the body gradually deteriorate? Any organized, non-random high information structure gradually becomes more disordered, and “worn away” with the passage of TIME, the destroyer. Entropy (disorder) gradually increases, in the absence of corrective energy input.
Even rocks and mountains eventually erode, given enough time. One of the most interesting characteristics of life is that it maintains its integrity for an inordinate amount of time, given its complexity and furious dynamism.
Every day our DNA sustains thousands of molecular ruptures from high energy radiation and other stressors. Proofreading and repair mechanisms are employed, at high energy cost, to repair these breaks. This corrective is especially efficient when we are young and vigorous; In our youth, our reproductive years, growth and repair predominate. Gradually, growth ceases, repair mechanisms age, and we become old.
Our Darwinian “warranty” expires. We are left with an aging body, unimportant to evolution. We are long on experience and short on future. But we still have a marvelous metabolism at our disposal, depending on our lifestyle. There are a number of metabolic pathways which affect aging, 2 of which have been more studied.
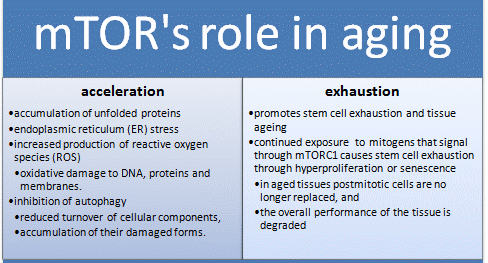
The mTOR pathway is most attuned to youth, senses nutrients and gears up for ANABOLISM, or growth. If you have not been careful to tailor your food intake to suit your decreasing requirements, your efficient metabolism stores it away for a rainy day, around your belly and in your arteries, a bad effect from an essential mechanism. Antagonistic Pleiotropy is the name for a body mechanism that can be good for one function (or age) and bad for another.
The Sirtuin system is also important in aging, and has a variety of housekeeping functions, including mitochondrial maintenance. It is activated by exercise. The cells of our bodies change with aging. In old tissues, there are less stem cells and other young, functional units. There are more damaged, dysfunctional “zombie” cells that don’t do much but promote inflammation, and hence more inflammatory cells accumulate.
Controlling the mTOR System and promoting the sirtuins help increase apoptosis and get rid of dysfunctional cells, including cancer. DOCTORS SHOULD PRESCRIBE EXERCISE, as well as SLEEP AND DIET, like they do medicine, and maybe we wouldn’t need so many pills. We might also feel better into old age.
Migraine Headache in its classic form is a unique syndrome, or grouping of symptoms. There is often a PRODROME of anxiety, mood changes or fatigue a day or two before the Headache. There may also be an AURA, such as visual or other sensory symptoms, preceding the headache by minutes.
The Headache is often ONE-SIDED (hence the name, HeMigraine). The Headache is SEVERE, and accompanied by NAUSEA AND VOMITING, a “sick” Headache.
There are a variety of TRIGGERS, such as ripened Cheeses, Red wine, Nitrate-containing foods like hot dogs and pepperoni, and missing your cup of coffee. Stress and Hormonal Changes (menstrual periods) may trigger Migraine.
Migraine often has a FAMILY HISTORY. If one parent has migraine, the risk is 50%, and if both parents, 75%. It is more common in women. During the Headache, Migraine sufferers often seek out a quiet, dark room, and avoid stimulation.
My own experience with Migraine is with isolated OPHTHALMIC MIGRAINE. I have the aura, but luckily have no pain. In my day, 50 years ago, Migraine was considered a Vascular Headache Problem, with Vasodilation being the cause. Many triggers result in Vasodilation.
After a half century of intense study, including the discovery of Calcitonin Gene Related Product (CGRP) in the blood during Migraine, It is now considered a NEUROVASCULAR Headache Problem, and there is optimism for future progress.
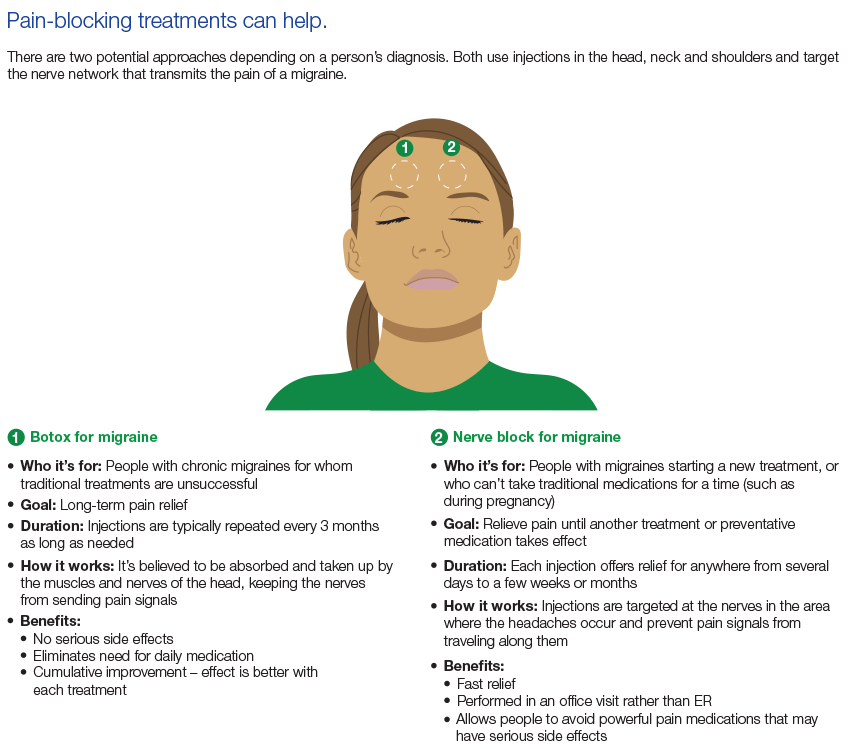
TREATMENT can be to abort, to shorten the attack after the warning Prodrome or Aura start. If the attacks are too frequent, such as several times a week,
PREVENTATIVE treatment may be needed. Medications include a host of chemicals, including Hormones, and most recently, CGRP. Many of these chemicals are vasoconstrictors, which narrow blood vessels.
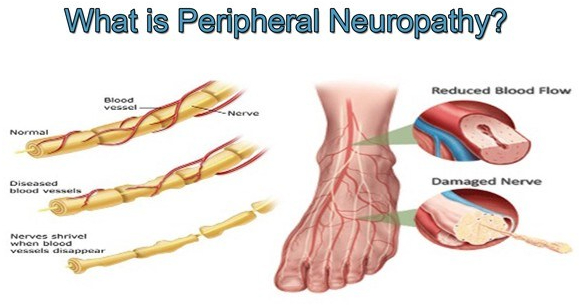
Peripheral Neuropathy is a common problem, and almost a quarter of the population will eventually suffer from it. It is very common in diabetes and metabolic syndrome, alcoholism, and in cancer therapy.
Even getting older is a risk; almost 10% of individuals 65 years old have some symptoms. There are more than 100 different types of peripheral neuropathy, and often it is just one feature of a primary illness.
Sometimes there is no known cause, such as in 2 of my older friends. I have a diminished vibratory sense in my feet, which causes me no noticeable problem. The longer nerves are more likely to be involved, except for the rare sensory ganglionopathy which is symptomatic of some cancers ( a “paraneoplastic disorder”) , some infections and autoimmune diseases.
When the sensory ganglia are involved, the numbness, tingling or pain can be more central, such as in the face or upper arm. There are 3 types of nerves that can be involved in peripheral neuropathy; Sensory, Motor and autonomic.
The sensory nerves deal with sensations, such as hot, cold, touch, pain, tingling, and numbness. Motor nerve involvement results in weakness or paralysis of an arm, leg or other area under Voluntary control. The autonomic nervous system coordinates activities beyond voluntary control, such as sweating, salivation, food propulsion and heart rate, which can be activated or inhibited.
The symptoms of neuropathy depend upon the type of nerve involved. Balance is a complex ability that can be disturbed by a lack of proper sensory nerve function (Position sense or proprioception) motor weakness, vision or coordination which involve higher centers.
The medical evaluation of peripheral neuropathy begins with a family practitioner or internist who does a detailed history, asking about such things as diet, medications, alcohol consumption, and injuries. Vitamin intake is important, but can be overdone.
Peripheral nerve symptoms can actually be caused by excessive B6, pyridoxine. The upper limit is 100 Mg.. A physical exam checks for weakness, sensory problems, reflexes and balance. Blood tests may reveal diabetic, kidney, liver, thyroid or immune problems problems.
A major disorder associated with neuropathy may be revealed and pursued. If nothing turns up, and the neuropathy is significant, referral may be needed to a neurologist, or other appropriate specialist. Many specialized tests and treatments may be needed.
Even with the best of care, a specific “cure” may not be found. Peripheral neuropathy can often be avoided by a healthy lifestyle.
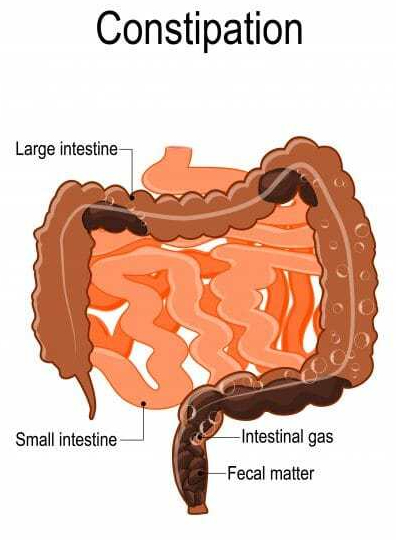
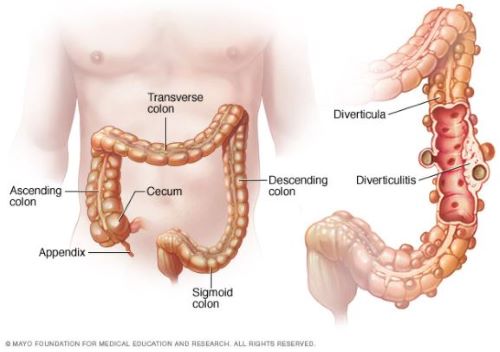
Your large bowel, or colon, is at the end of the Gastrointestinal tract. It starts on the right side of your abdomen, where the small intestine empties into the caecum. This is also where the Appendix bulges down, looking like a little finger coming from the caecum. The 5 foot long large intestine is the final processing area of your food, after the nutrients have been absorbed.
The Colon contains virtually all of the microbiome, reduces the volume of the fecal matter, and propels it to its final destination. The propelling muscles are an inner circular ring, and 3 outer longitudinal strips. These outer strips of muscle do not completely encircle the Colon, allowing for protuberances of lining membrane and circular muscle to balloon out into prominences called Taenia.
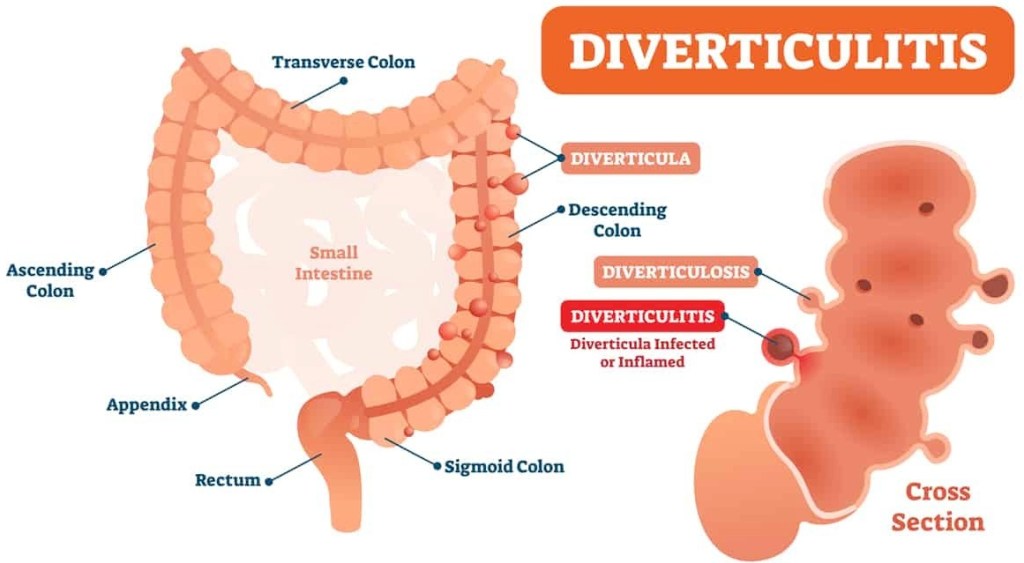
It is in these weakened areas, especially where blood vessels penetrate that little herniations form over the years. Diverticulosis occurs in 50% of people more than 60 years of age, and in almost everybody more than 80 years.
Diverticulosis is a condition where pressures up to 120 mm or mercury, generated by the colonic muscles gradually push out little pouches of lining membrane called diverticula. Nobody knows why some people get an INFLAMMED diverticulum.
Age, of course, is a factor, as are Obesity, diabetes, smoking and poor diet; a tendency toward inflammation is common in all of these risk factors. Comparing diverticulitis with Appendicitis is an interesting exercise. The symptoms are mirror images of each other. Appendicitis occurs on the right side.
Diverticulitis usually occurs on the left side, except in asian people. The asian DIET seems to favor diverticula on the right side. When asians immigrate to the U.S. and start eating more Red meat and fewer vegetables, the diverticula shift to the left side.
Signs of Diverticulitis include gastrointestinal symptoms, such as pain, tenderness,nausea, cramps, constipation, and Fever. Rectal bleeding can sometimes occur. Treatment includes antibiotics.
If the condition worsens, serious complications, such as abcess may develop and require surgery. As usual, Prevention, including diet and exercise, is better than Treatment. A HIGH FIBER DIET is the best prevention.
–Dr. C.
Article #1 to read – Diverticular disease of the colon: New perspectives in symptom development and treatment
Article #2 to read – Management of Colonic Diverticulitis | Effective Health Care Program
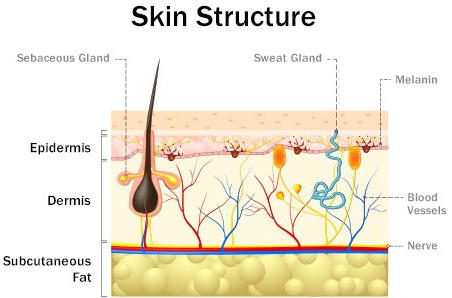
The skin is the protective barrier between the inside of our bodies and the outside world of microorganisms, parasites and toxins. It is often the site of inflammation and infections.
In past times, before the advent of cleanliness and antibiotics, mankind was plagued by erysipelas, boils, carbuncles, and other severe infections of the skin, which are rarely seen now. The beta hemolytic streptococcus and Staphylococcus aureus were ubiquitous in the past, and mostly are contained today.
Severe Infections presently require some skin abnormality, immune deficiency, neglect, animal bite or other breach of skin integrity to be a problem. Antibiotic resistance, however, is allowing some organisms like MERSA to make a comeback.
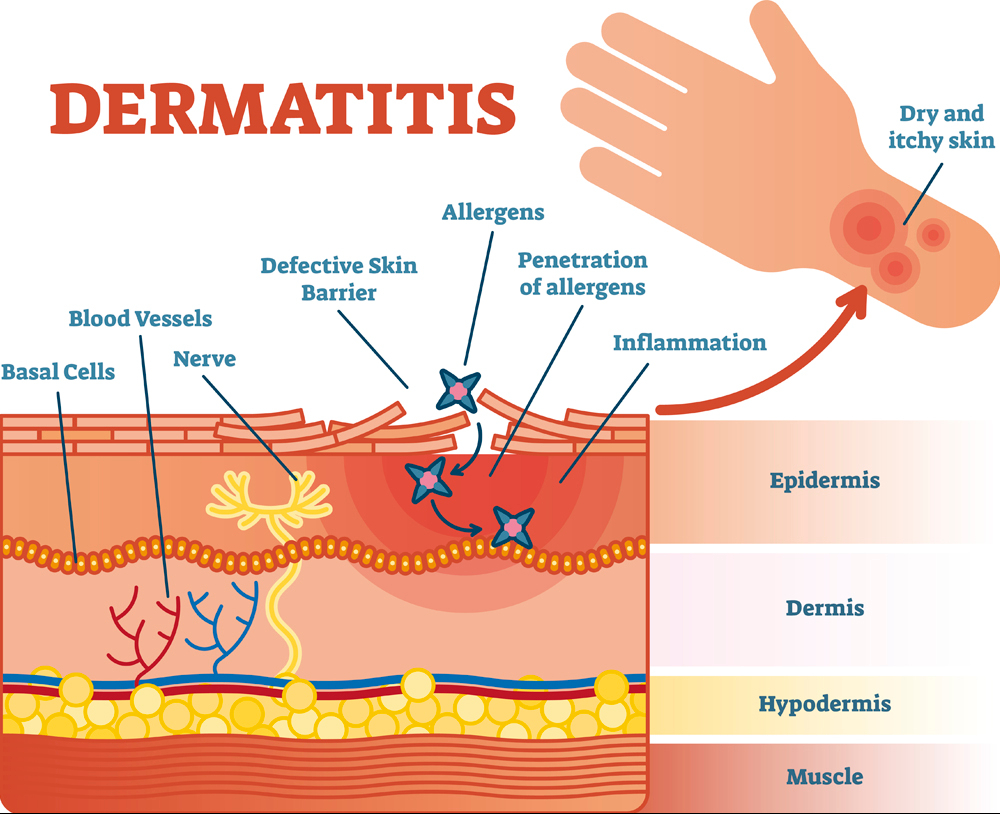
ECZEMA. or Atopic Dermatitis, was common in my medical practice. This condition weakens the skin barrier, allowing Staphylococcal infection to gain a foothold. In my day, If there were a flare of eczema severity, antibiotics would often help. Leg edema and swelling. such as from heart failure, especially coupled with diabetes and blood vessel disease is also an invitation to infection, such as cellulitis.
Redness, swelling, warmth and pain- the classic rubor, tumor, calor and dolor- as well as swollen local lymph nodes and fever often betray infection of the skin. Please see the recently posted infographic on celulitis.
IMMUNE DEFICIENCY raises the likelihood and risk of severe skin infections. Infection from “flesh-eating bacteria”, often beta hemolytic streptococci in deep tissue planes , is a medical emergency. Immediate surgery is often needed.
Disproportionate PAIN after injury or surgery is often a clue. Certain age groups have characteristic skin infections, such as the scalded skin syndrome of infants, and the acne of adolescents. Viruses, molds, and arthropods can also infect the skin.
Viruses, such as herpes in particular can simulate bacterial infection. Ringworm from fungi is easy to distinguish, but arthropod bites, and especially bee sting can look very much like bacterial infection. Scabies and mite infestation are so itchy as to be distinct.
Topical antibiotics applied on skin breaks like cuts or breaks are useful in preventing infection. These ointments and creams are like “artificial skin”. Once again, prevention is key.
Red hair and freckles are associated with MCR-1 gene variants, and large areas of skin with lowered melanin protection against the adverse effects of the sun. I have red hair and freckles, for which I was teased. My response was that I had a lot of Iron in my blood, and that the freckles were Rust. This is ironic (no pun intended).
Since becoming an Octogenarian, I have had trouble keeping my Iron levels normal. I live in a beach area, where all the young ladies are sunning themselves to promote the socially desirable “bronze goddess” effect, and all of the older ladies hide their leathery skin and wear broad-brimmed hats.
The sun has a good reputation as a health-giver. Being outside does correlate with a lot of beneficial effects, such as enhancing production of Vitamin D. My recommendation, however biased, is to get your Vitamin D in capsule form, and reduce sun exposure.
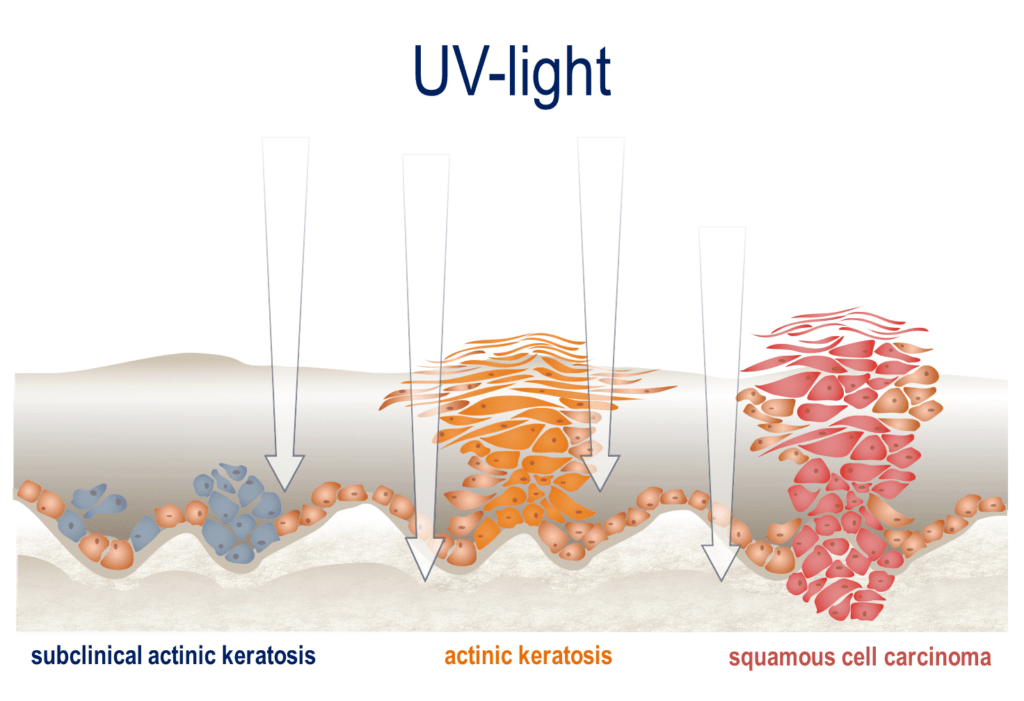
SUNSHINE, however salutary, is accompanied by invisible, high energy photons capable of breaking DNA strands, and ultimately causing SKIN CANCER. Not accidentally,Visible light has insufficient energy to break bonds, although the rhodopsin in rods and cones do release electrons if stimulated by light.
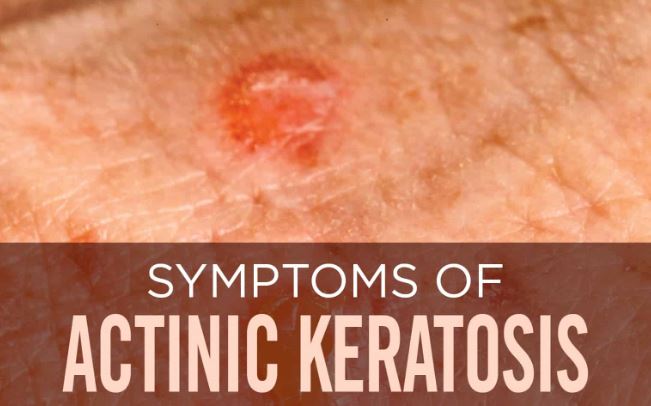
Actinic Keratoses are the roughened plaques of skin, often on the face, which have a small but definite risk of turning into Cancer. I have a dermatology check every 6 months for precancerous areas to be frozen and destroyed by CO2 spray.
PREVENTION of UV Skin damage is advisable. I wear a broad brimmed hat and UV-blocking sunglasses (UV can promote cataracts and retinal damage as well) when outside in the sun. When swimming I wear a “rashguard” shirt with UV protection in the fabric.
Also, I try to limit my exposure to the Evening and Morning sun, because the light is warmer, and contains less UV. Even with these precautions, I use Sunscreen creams and lotions. I always wondered how a transparent lotion can block UV light.
The explanation lies in the chemicals contained. Such chemicals as Avobenzone and Homosalicylate actually absorb the energy of UV light. Protect yourself now for later health.
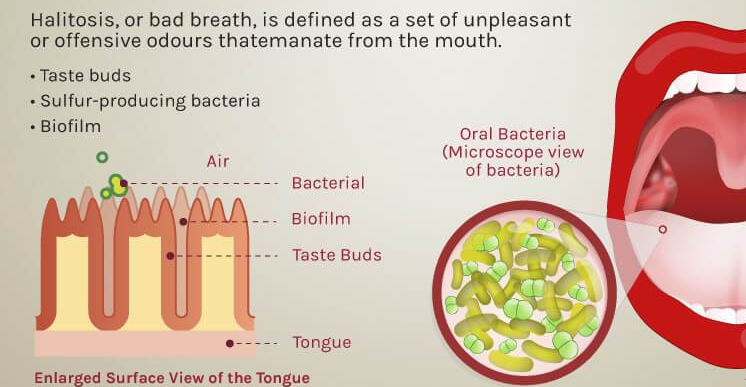
Bad breath is a big social deal, and is unpleasant to be around. You are always conflicted when near a person with Halitosis; you are tempted to tell him for his own good, but are embarrassed to do so.
“Mask Breath” is the most recent reincarnation of bad breath. Supposedly the mask itself does not have an odor, but merely makes the person aware of the bad breath he has had all along. Bad breath is not only a direct problem for the person who has it, but often betrays important medical conditions which need attention.
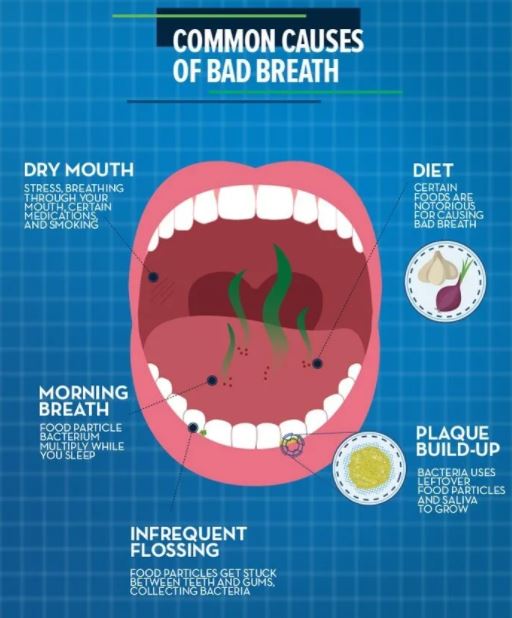
Several oral conditions can cause halitosis. The most common is poor oral hygiene. Lack of regular brushing and flossing leads to accumulation of food particles between the teeth, in the gum lines, and even under crowns. This food provides lunch for the oral bacteria, releasing malodorous compounds. This can be expensive. Have you priced restorations and implants recently?
The sneakier result of poor oral hygiene is gingivitis, or gum disease. This leads to inflammation, and is a major contributor to the inflammatory load resulting in Metabolic syndrome with its widespread effects on the brain, kidneys, and heart. And in addition, you may eventually lose your teeth. Tonsils can become inflamed and malodorous, and the associated adenoids may enlarge, leading to mouth breathing, dry mouth, and you guessed it, Bad Breath.
GERD is often associated with Bad Breath. The reflux of stomach contents will often leave behind a bad taste as well as bad breath. Certain metabolic conditions can give bad breath. Ketosis from diabetes, mousy breath from liver failure, and the “Fish odor syndrome”, Trimethylaminuria, can be causes.
So drink lots of water, and don’t forget to brush your teeth and floss regularly. You might benefit from a medical or dental evaluation if your bad breath doesn’t go away.
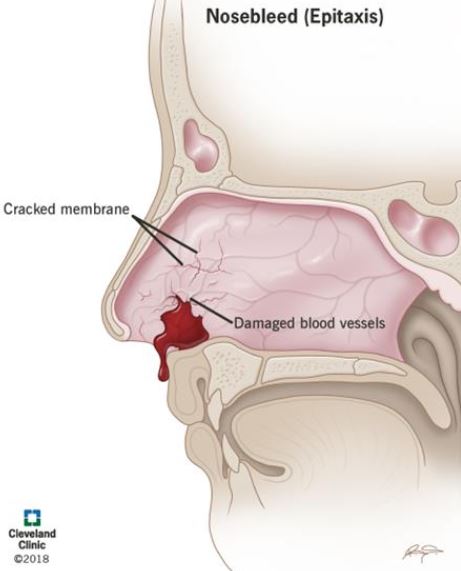
Nosebleeds afflict almost everybody at one time or another. The nose is well supplied with blood vessels, and sticks out from the face, often into other people’s business. Fistfights and falls will often cause nosebleeds in children. Kids will often pick their noses.
Dry air and allergies make the nose bleed more often. Sometimes, nosebleeds just happen. The bleeding usually comes from the front of the septum, the cartilaginous divider of the nose, and the best way to stop the bleeding is to lean forward and pinch the nostrils together.
This most likely compresses the bleeding area, and if held for 5 minutes or so will usually stop the bleeding. Sometimes, even after repeating this several times, and even putting ice on the bridge of the nose, the bleeding won’t stop, you may need to seek help. If the bleeding is voluminous it may originate from larger vessels at the back of the nose, and an ENT Doctor may be needed to put in a “posterior pack” of gauze.
Infrequent nosebleeds from identifiable causes are not too disturbing, but if they become CHRONIC and unexplained, a visit to the doctor and further investigation may be needed.
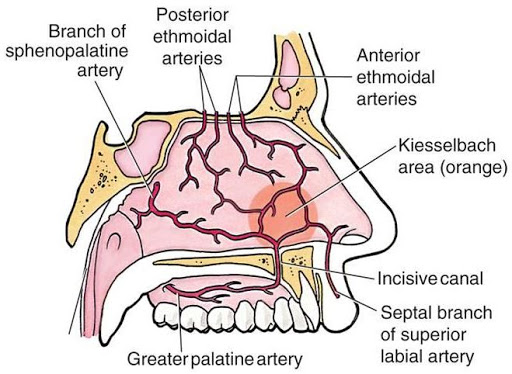
High blood pressure can be a cause of regular nosebleeds. High altitudes and the accompanying dry air can be a contributory cause. Cocaine use may irritate the nose and cause “Kiesselbach’s plexus” on the anterior nasal septum to bleed.
If you bleed a lot from your nose, especially if you have trouble with clotting from cuts or periods, you may have a coagulation problem, of which there are several, such as Von Willebrands disease.
Blood thinners are commonly used these days, and the dosage may need adjusting. For more information, please consult the accompanying article on “epistaxis” by the Cleveland Clinic, which usually has good articles on medical problems.
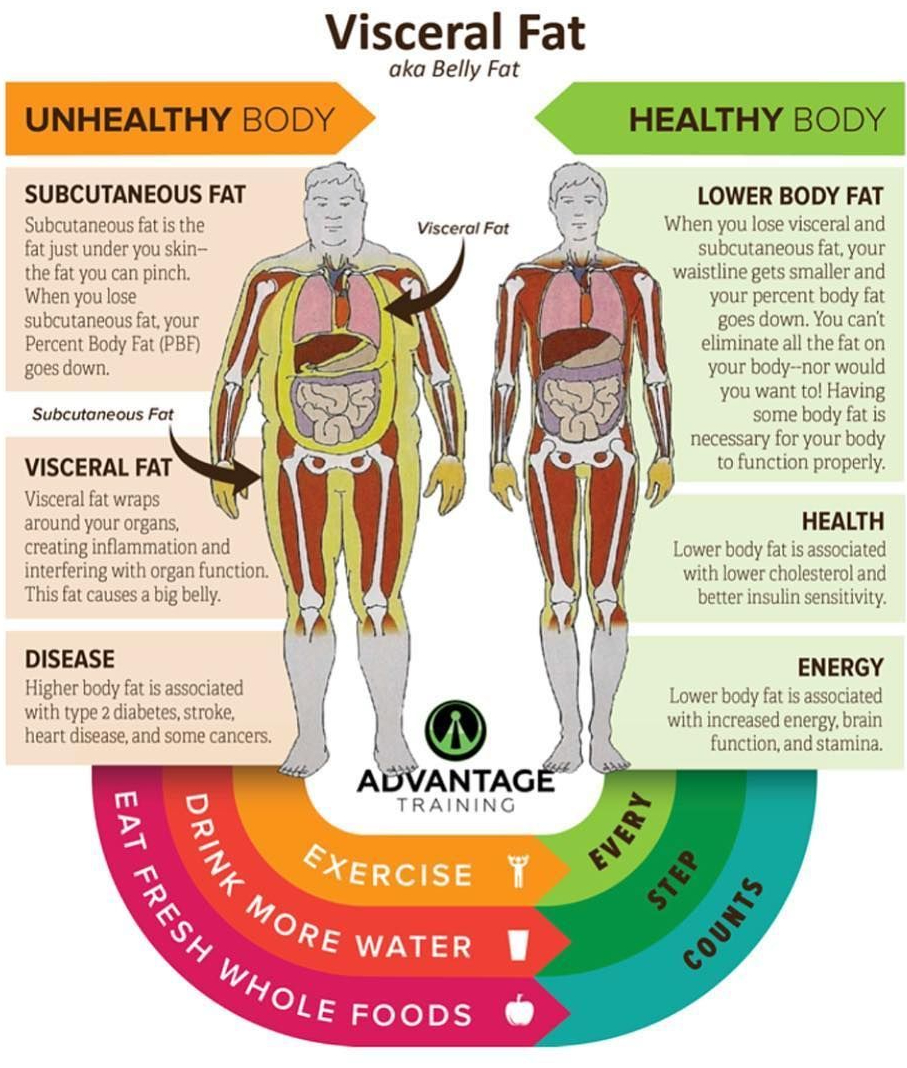
ABDOMINAL (VISCERAL) FAT KILLS. The following post tells you how, and suggests what you might do to prevent this scourge, which is gradually becoming an epidemic in America.
OBESITY is an energy imbalance problem. MORE CALORIES ARE CONSUMED THAN ARE NEEDED AND CAN BE UTILIZED. A Good quality Diet, with lots of natural (rather than processed) foods, especially vegetables and fruits, have lots of FIBER that takes up space and makes you feel full.
Fiber also feeds the MICROBIOME. If the foods are DIVERSE, the microbiome will also be diverse and help utilize the calories you eat. A healthy Microbiome also contributes to your health by manufacturing neurotransmitters, vitamins, and other factors that are just starting to be appreciated. Diet QUALITY, as well as quantity, is important.
EXERCISE is critical for more than utilizing calories. It increases ADIPONECTIN which guides fat to fat stores where they belong, rather than to the liver, and IRISIN which favors the production of BROWN FAT, thus utilizing energy. The opposite of exercise, the SEDENTARY LIFESTYLE, is now considered a disease system in itself.
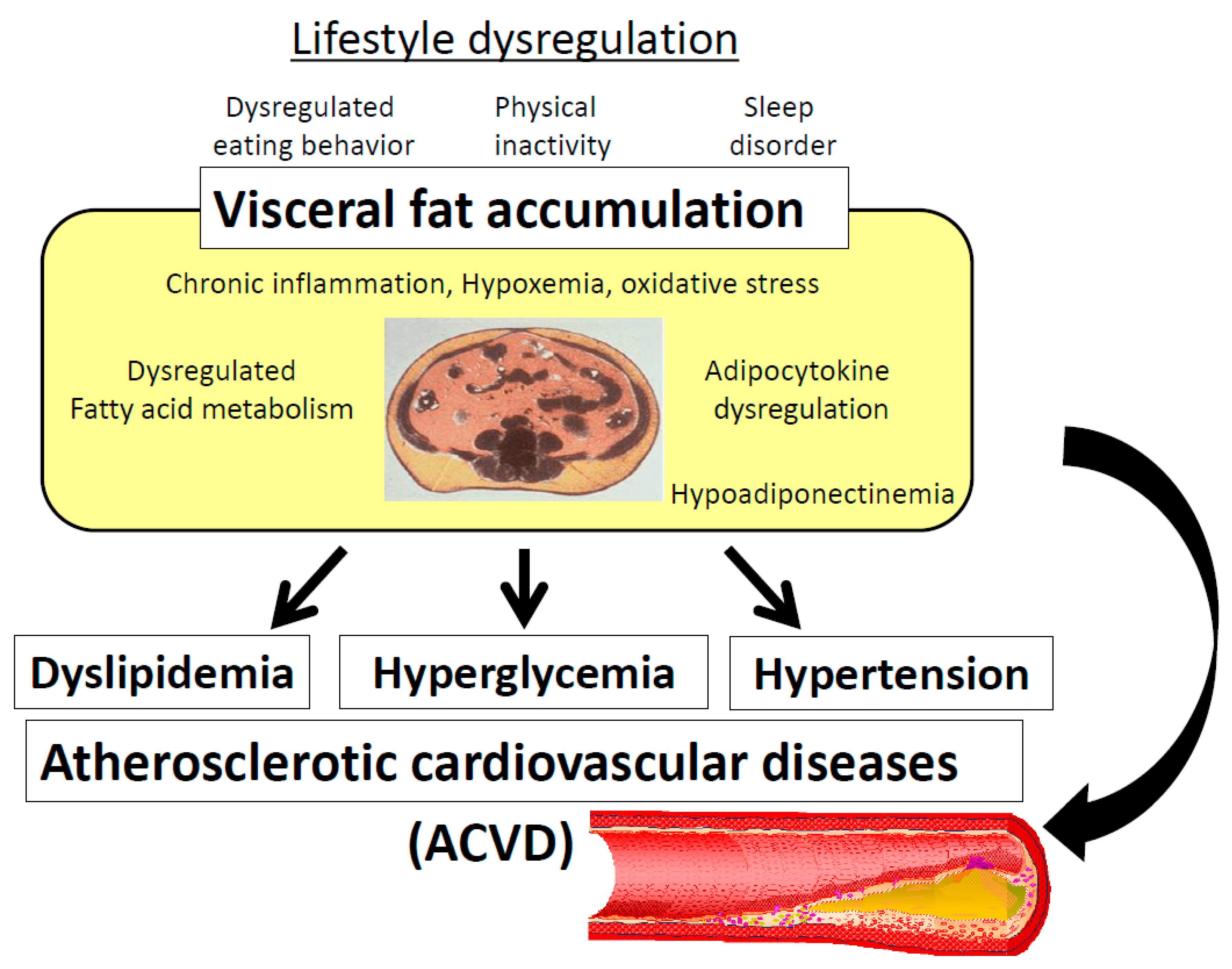
Lack of SLEEP favors obesity in a number of ways; at the very least, you can’t eat while asleep. Abdominal fat contains INFLAMMATORY cells which go directly to the Liver via the hepatic portal system to cause metabolic disruption. Insulin sensitivity falls, blood sugar, LDL and triglycerides rise. DIABETES and the METABOLIC SYNDROME result.
The excessive weight also causes back, hip and knee problems which contribute to the 10% increase in overall medical costs due to Obesity.
We have no photographs, abdominal, navel-level girth measurements, CTs, BMIs or death certificates to prove it, but it is highly unlikely that Paleolithic Humans suffered from excessive abdominal fat. They had no refrigerators, deliciously packaged snacks, sugary, fructose-containing soft drinks and candy, nor did they have cave-lighting to extend their daylight eating hours and disrupt their diurnal rhythm.
They had to walk or run long distances to obtain their meagre food supplies, which tired them out so that they most likely had a good night’s sleep. SLEEP, DIET and EXERCISE are built into our Metabolism by Darwinian Evolution. Paleolithic humans didn’t live long lives and succumb to cancer and heart disease.
They died most often by violence, which made Blood clotting a survival benefit, rather than the Risk factor for stroke and heart attacks that coagulation is to us now. It is not all our fault that OBESITY is steadily increasing over the last few decades.
CAPITALISM is driven to provide us with ever increasingly available and tasty food. Both consumers and purveyors scream when even the most logical political check on OVEREATING is legislated: Taxing of sugary, fructose-containing, nutritionless soft drinks was tried in Philadelphia to a chorus of complaints. To my knowledge the tax has survived, reduced sugary drink consumption, and was helpful in reducing the weight of Philadelphia residents. Not many cities were brave enough to follow suit.
GENETIC Influences can also conspire against weight control. The FTO gene, while relatively infrequent does have an influence, as shown in twin studies. And there seems to be a SET POINT in weight that makes it difficult to take off the pounds and keep them off. 2 years after almost all diets, the weight has returned. Eating HABITS, once established are hard to change.
BARIATRIC SURGERY has been shown to help Obesity, as well as Metabolic syndrome and Diabetes .I hope it will survive the test of time. Weight gain is easier to PREVENT than it is to treat. Somehow, society must get to the children, and keep them from gaining weight in the first place. Even children are now becoming obese.
INTERMITTENT FASTING can help contain Obesity. My own version is TIME-RESTRICTED EATING. I limit my eating to 6 hours a day, from Noon (usually 1PM) until 6PM. This has resulted in a modest weight loss from 142 pounds to 137 pounds. My son lost some 30 pounds in a 30 day, 1000 calorie “crash” diet to fend off advised Back Surgery. He exercised a lot of SELF CONTROL both to lose the weight, and to keep it off.
Unfortunately, Self Control is in short supply in our present SOCIETY OF EXCESS. Good luck in your quest, if you choose to embark on weight reduction. And good luck with your health if you don’t. I recommend “the secret life of fat” by Sylvia Tara in either case. Also, search for intermittent fasting in DWWR.
–Dr. C.
Empowering Patients Through Education And Telemedicine