

It also shows that restoring the integrity of the epigenome reverses age-related symptoms.
Learn more at https://hms.harvard.edu/news/loss-epi…

It also shows that restoring the integrity of the epigenome reverses age-related symptoms.
Learn more at https://hms.harvard.edu/news/loss-epi…
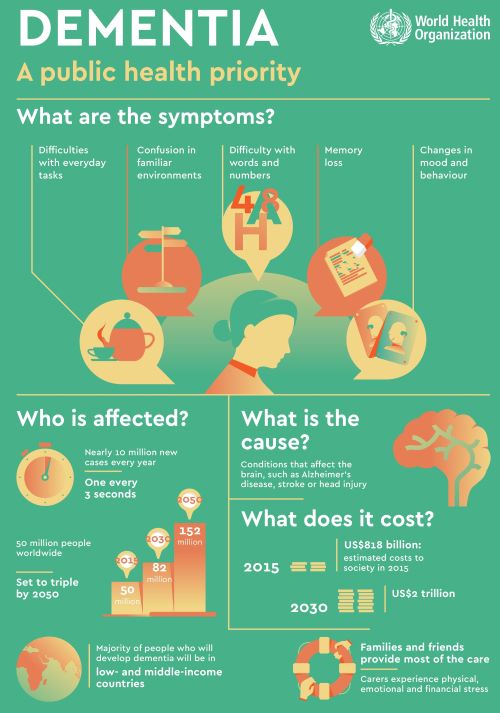
Biomarkers are measurable indicators of what’s happening in your body. They can be found in blood, other body fluids, organs, and tissues, and can be used to track healthy processes, disease progression, or even responses to a medication. Biomarkers are an important part of dementia research.
For many older adults, a good night’s rest is elusive. The implications of chronically poor sleep can be far-reaching and include a decline in cognitive functioning and detrimental effects on health and general well-being. Fortunately, relief may be in sight.
A new study led by investigators at the Stanford University School of Medicine shows that neurons in the lateral hypothalamus, a brain region, play a pivotal role in sleep loss in old mice. More specifically, the arousal-promoting hypocretin neurons become hyperexcitable, driving sleep interruptions.
Read the full story: https://stan.md/3JQ7z77
Luis de Lecea, PhD, is a professor of psychiatry and behavioral sciences at Stanford Medicine. He is the study’s senior author and hopes the finding could pave the way to new drug treatments for age-related sleep problems in humans.
Shi-Bin Li, PhD, is an instructor in the Psychiatry and Behavioral Sciences department at Stanford Medicine. He is also a basic life research scientist in the de Lecea lab, and is the lead author of the study. Lisa Kim is Senior Manager of Media Relations for Stanford Medicine and Stanford Health Care. Lisa has a deep background in journalism, as she is an Emmy Award-winning journalist who has covered stories on both the national and local levels.
Swelling of the ankles becomes increasingly common as you get older. This swelling can be caused by thrombophlebitis, or skin infections which have been discussed in previous articles. Otherwise it is usually part of a condition called edema.
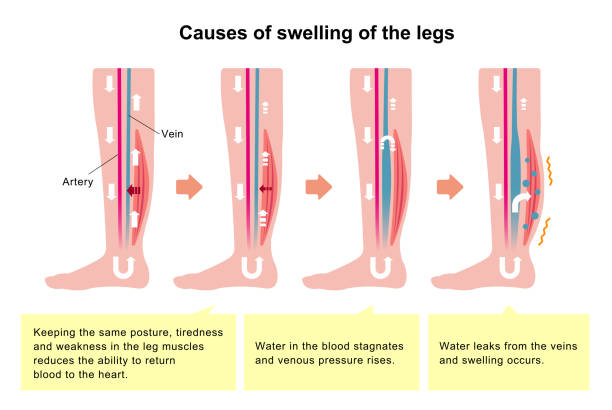
Edema is commonly caused by problems in the cardiovascular system, kidneys, or liver. Edema can occur in the face and abdominal cavity or elsewhere, But because of gravity and the fact that we are usually upright-on our feet, it is usually is most prominent in the legs, especially the ankles. Edema can be caused by a normal pregnancy. The developing baby puts quite a strain on the heart and circulatory system.
Chronic accumulation of fluid in the tissues usually occurs because of heart and blood vessel problems, liver disease (albumin lack), diet (excess salt intake), kidney disease (deficient salt excretion), vein problems (valve malfunction), and lymphatic problems (surgical lymph node excision).
Obesity contributes by impacting the heart and liver primarily. Proper sleep, diet and exercise help in most of these areas, and edema is rare in healthy people.
I have always considered sugar(obesity, cardiovascular effects) and salt(hypertension, cardiovascular and kidney load) as poisonous. I discovered the valve incompetence in the veins of my left leg because it became more blue than my right leg. With good exercise, sleep, diet program and compression stockings, edema never occurred.
The swelling and stretched shiny skin in the ankles that I see in many of my overweight friends makes a tempting target for germs of all kinds. and small skin sores often follow.
If you developed swelling in your ankles or other areas, it’s best to check with your doctor to get an explanation.
Sleep apnea and obesity are bound together as Charles dickens observed in his Pickwick papers. The Pickwickian syndrome is obesity associated with alveolar hypoventilation(insufficient breathing) with an increase in CO2 in the bloodstream which causes narcosis, or SLEEPINESS, in the daytime.
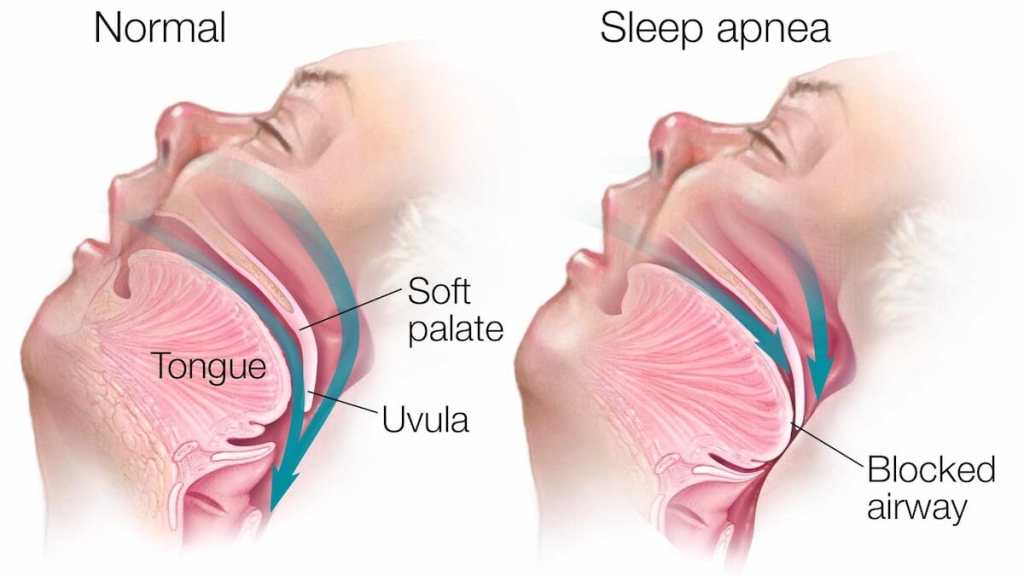
When I went in for my sleep apnea study, I noticed a number of double wide chairs available for the usual clientele there. OBESITY is one of the major risk factors for sleep apnea. Depositions at the base of the tongue and throat interfere with breathing, and causes snoring to the point of tracheal blockage and apnea at night.
Some people with normal “ BMI”, have sleep apnea. Sleep apnea can run in families, occur when you are older, or have a thick neck. So no matter what your weight, if you have daytime sleepiness after an apparently full night of sleep, you should be considered for a sleep study.
A SLEEP STUDY requires that you go into a sleep center overnight, get hooked up to an electroencephalogram machine, oxygen monitor, chest straps, and the like. This is the gold standard for a diagnosis of sleep apnea, but a recording pulse oximeter will let you know a lot less expensively if you have the critical problem, a drop in oxygen saturation. The type of sleep apnea I have been discussing so far is obstructive sleep apnea. Of course there are other types such as central, or complex sleep apnea.
Most sleep apnea responds to nasal CPAP, if you can tolerate it.
My own sleep apnea was diagnosed as moderate, 15% central and 85% obstructive in type. I have a stuffy nose which I believe to be the main problem setting me up for sleep apnea, and I could not tolerate the positive nasal CPAP. There is also a dental apparatus that I tried unsuccessfully. I wound up sleeping on my side, and propping myself in that position with pillows .This seems to help me, but I still wake up several times a night, usually at the end of a 90 minute sleep cycle, and with a full bladder.
I sleep through better on days when I have had more physical or mental exercise. Avoiding a full stomach at bedtime is also helpful with both sleep apnea and GERD.
I do use Afrin on the left side of my nose, which is more obstructed. I restrict the use to every third day, although I have heard that you can use it every other day, alternating sides, if you have a stuffy nose that has resisted other treatments .I have also heard that using corticosteroid nasal sprays makes Afrin better tolerated. Be sure to get clearance with your doctor before trying this.
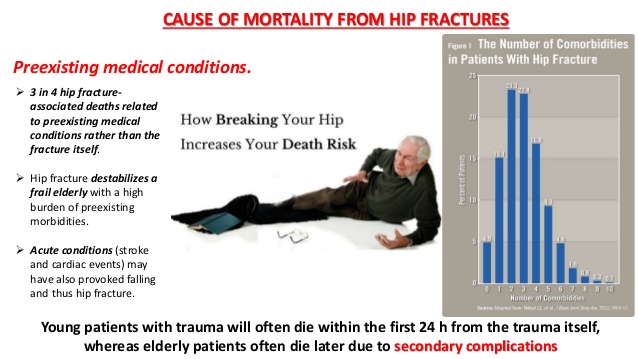
Hip fracture is an iconic bugaboo of old age. It is a chronic condition in the sense that its complications, such as Depression, blood clots and pneumonia often extend long beyond the healing process.
Predisposing factors include old age and associated risk factors like osteoporosis, sarcopenia (loss of muscle mass and strength), poor vision, poor balance and hazards in the home.
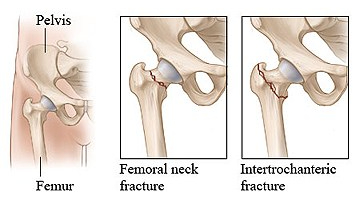
FALLING is the usual agency that produces the fracture. At the risk of being ostracized, I will point out that thousands of injuries sustained by walking or tripping over dogs (and cats) occur every year.
In my small “hilltop” group of friends, there was 1 fatality, 1 shoulder fracture-dislocation, 1 hip fracture, and 0 acknowledgements of animal causation. Members of the family are immune to blame.
Treatment of hip fracture involves surgery with pins, or the more cost-effective Hip replacement. PREVENTION is critical. Osteoporosis must be prevented by exercise, Calcium, vitamin D, and avoidance of certain medication like Corticosteroids.
Balance should be developed by exercises. Vision problems, such as cataracts,should be corrected. Muscle mass should be preserved by diet and exercise, and the home cleared of throw-rugs and obstacles removed.
Just yesterday, a friend wearing socks (reducing friction?) fell down some stairs after stepping over a dog-gate. She is scheduled to have her elbow pinned. Have I mentioned SLEEP, DIET and EXERCISE RECENTLY?
–Dr. C.

Old age is an inevitable condition if you are lucky enough to live a long life. Middle aged people say it begins at 70 years of age. According to an Elysium survey of people 40 and older, the average American FEELS old for the first time at age 47 years.
In the distant past, 50 was CONSIDERED to be old. The generally better conditions and Medicine of modern times keeps extending LIFESPAN, if not always HEALTHSPAN. Old age is certainly a Condition, and it is for sure Chronic, thereby qualifying for inclusion, but is it a Disease?
It is not considered a disease by the authorities, and so it doesn’t gather research funds like it should. What exactly IS old age? Being 88 Years old, and a physician, I feel qualified to comment. Old age is a collection of past accidents and sports injuries plus complications of past illnesses engrafted on a gradually deteriorating body.
Where does Obesity and Metabolic syndrome fit in this rubric? The Plague of our time fits in the disease category. It is definitely preventable, although with difficulty. Please search past postings for more information on this topic.
In what way does the body gradually deteriorate? Any organized, non-random high information structure gradually becomes more disordered, and “worn away” with the passage of TIME, the destroyer. Entropy (disorder) gradually increases, in the absence of corrective energy input.
Even rocks and mountains eventually erode, given enough time. One of the most interesting characteristics of life is that it maintains its integrity for an inordinate amount of time, given its complexity and furious dynamism.
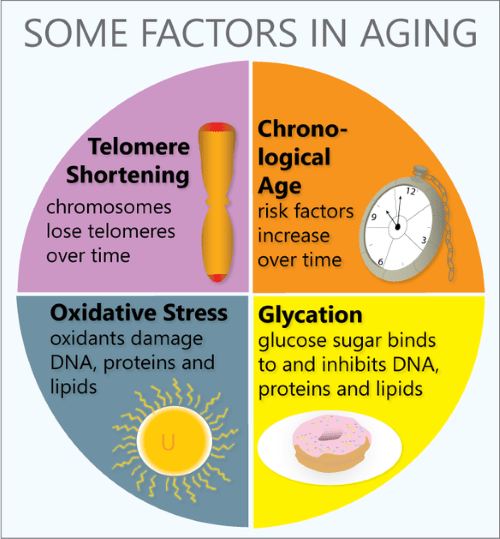
Every day our DNA sustains thousands of molecular ruptures from high energy radiation and other stressors. Proofreading and repair mechanisms are employed, at high energy cost, to repair these breaks. This corrective is especially efficient when we are young and vigorous; In our youth, our reproductive years, growth and repair predominate. Gradually, growth ceases, repair mechanisms age, and we become old.
Our Darwinian “warranty” expires. We are left with an aging body, unimportant to evolution. We are long on experience and short on future. But we still have a marvelous metabolism at our disposal, depending on our lifestyle. There are a number of metabolic pathways which affect aging, 2 of which have been more studied.
The mTOR pathway is most attuned to youth, senses nutrients and gears up for ANABOLISM, or growth. If you have not been careful to tailor your food intake to suit your decreasing requirements, your efficient metabolism stores it away for a rainy day, around your belly and in your arteries, a bad effect from an essential mechanism. Antagonistic Pleiotropy is the name for a body mechanism that can be good for one function (or age) and bad for another.
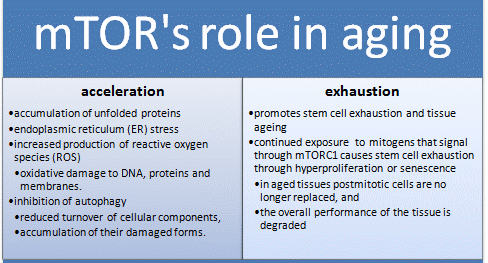
The Sirtuin system is also important in aging, and has a variety of housekeeping functions, including mitochondrial maintenance. It is activated by exercise. The cells of our bodies change with aging. In old tissues, there are less stem cells and other young, functional units. There are more damaged, dysfunctional “zombie” cells that don’t do much but promote inflammation, and hence more inflammatory cells accumulate.
Controlling the mTOR System and promoting the sirtuins help increase apoptosis and get rid of dysfunctional cells, including cancer. DOCTORS SHOULD PRESCRIBE EXERCISE, as well as SLEEP AND DIET, like they do medicine, and maybe we wouldn’t need so many pills. We might also feel better into old age.
Disease, Metabolic syndrome, Entropy, DNA, Metabolism, Apoptosis, Zombie cells

If you’re enrolled only in original Medicare with a Medigap supplemental plan, and don’t use a drug plan, there’s no need to re-evaluate your coverage, experts say. But Part D drug plans should be reviewed annually. The same applies to Advantage plans, which often wrap in prescription coverage and can make changes to their rosters of in-network health care providers.

“The amount of information that consumers need to grasp is dizzying, and it turns them off from doing a search,” Mr. Riccardi said. “They feel paralyzed about making a choice, and some just don’t think there is a more affordable plan out there for them.”

When creation of the prescription drug benefit was being debated, progressive Medicare advocates fought to expand the existing program to include drug coverage, funded by a standard premium, similar to the structure of Part B. The standard Part B premium this year is $144.60; the only exceptions to that are high-income enrollees, who pay special income-related surcharges, and very low-income enrollees, who are eligible for special subsidies to help them meet Medicare costs.
“Given the enormous Medicare population that could be negotiated for, I think most drugs could be offered through a standard Medicare plan,” said Judith A. Stein, executive director of the Center for Medicare Advocacy.
“Instead, we have this very fragmented system that assumes very savvy, active consumers will somehow shop among dozens of plan options to see what drugs are available and at what cost with all the myriad co-pays and cost-sharing options,” she added.
Advocates like Ms. Stein also urged controlling program costs by allowing Medicare to negotiate drug prices with pharmaceutical companies — something the legislation that created Part D forbids.
COMMENTARY
Medicare is a blessing. It is a great help to retired and elderly people and generally does the job it was intended to do. There are a great variety of Medicare supplement plans and pharmaceutical purchase plans, And they jockey and change every year.
I get a headache just thinking about how to compare these plans from my individual needs and and whether their cost is worth it. The take-home message from the New York Times article is that you can get individual attention from an advisor who presumably knows the field well.
The key acronyms are SHIP and HICAP, which stands for state health insurance assist program and California health insurance counseling and advisor program respectively.
The California number is 1-800-434-0222. Be sure to write down the medications that you are taking and Your diagnosed illnesses, as well as your financial status in order to make best use of the service.
—Dr. C.
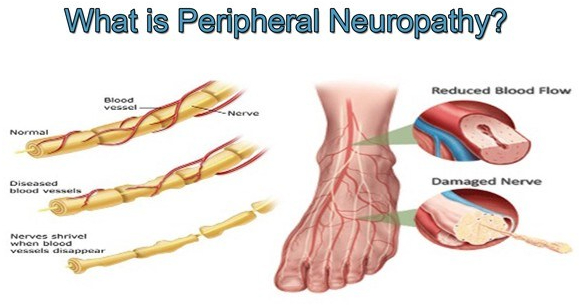
Peripheral Neuropathy is a common problem, and almost a quarter of the population will eventually suffer from it. It is very common in diabetes and metabolic syndrome, alcoholism, and in cancer therapy.
Even getting older is a risk; almost 10% of individuals 65 years old have some symptoms. There are more than 100 different types of peripheral neuropathy, and often it is just one feature of a primary illness.
Sometimes there is no known cause, such as in 2 of my older friends. I have a diminished vibratory sense in my feet, which causes me no noticeable problem. The longer nerves are more likely to be involved, except for the rare sensory ganglionopathy which is symptomatic of some cancers ( a “paraneoplastic disorder”) , some infections and autoimmune diseases.
When the sensory ganglia are involved, the numbness, tingling or pain can be more central, such as in the face or upper arm. There are 3 types of nerves that can be involved in peripheral neuropathy; Sensory, Motor and autonomic.
The sensory nerves deal with sensations, such as hot, cold, touch, pain, tingling, and numbness. Motor nerve involvement results in weakness or paralysis of an arm, leg or other area under Voluntary control. The autonomic nervous system coordinates activities beyond voluntary control, such as sweating, salivation, food propulsion and heart rate, which can be activated or inhibited.
The symptoms of neuropathy depend upon the type of nerve involved. Balance is a complex ability that can be disturbed by a lack of proper sensory nerve function (Position sense or proprioception) motor weakness, vision or coordination which involve higher centers.
The medical evaluation of peripheral neuropathy begins with a family practitioner or internist who does a detailed history, asking about such things as diet, medications, alcohol consumption, and injuries. Vitamin intake is important, but can be overdone.
Peripheral nerve symptoms can actually be caused by excessive B6, pyridoxine. The upper limit is 100 Mg.. A physical exam checks for weakness, sensory problems, reflexes and balance. Blood tests may reveal diabetic, kidney, liver, thyroid or immune problems problems.
A major disorder associated with neuropathy may be revealed and pursued. If nothing turns up, and the neuropathy is significant, referral may be needed to a neurologist, or other appropriate specialist. Many specialized tests and treatments may be needed.
Even with the best of care, a specific “cure” may not be found. Peripheral neuropathy can often be avoided by a healthy lifestyle.





