Target LDL depends on many factors, including your age, family history, and personal history of cardiovascular disease. For people at intermediate risk, LDL should be lowered by 30% to 50%. For those who have already had a heart attack, target LDL is no more than 70 mg/dl (note: automatic download).
Which non-statin therapies are recommended first?
Five non-statin therapies described in this post aim to help people achieve target LDL goals while minimizing side effects. They may be combined with a statin or given instead of statins.
Each helps lower LDL cholesterol when diet and statins are not sufficient, such as when there is a family history of high cholesterol (familial hypercholesterolemia). But so far, only two options are proven to reduce cardiovascular risk — the risk for heart attack, stroke, heart failure, and other issues affecting the heart and blood vessels.
Ezetimibe (Zetia)
What it does: Lowers LDL and cardiovascular risk by reducing cholesterol absorption.
How it’s given: A daily pill
Relatively inexpensive and often given with statins.
PCSK9 inhibitors, alirocumab (Praluent) and evolocumab (Repatha)
What it does: A protein called PCSK9 controls the number of LDL receptors on cells. These medicines are monoclonal antibodies against PCSK9 that increase LDL receptors on the liver, helping to clear circulating LDL from the bloodstream.
How it’s given: A shot every two to four weeks
Highly effective for lowering LDL, but expensive and may not be covered by insurance.
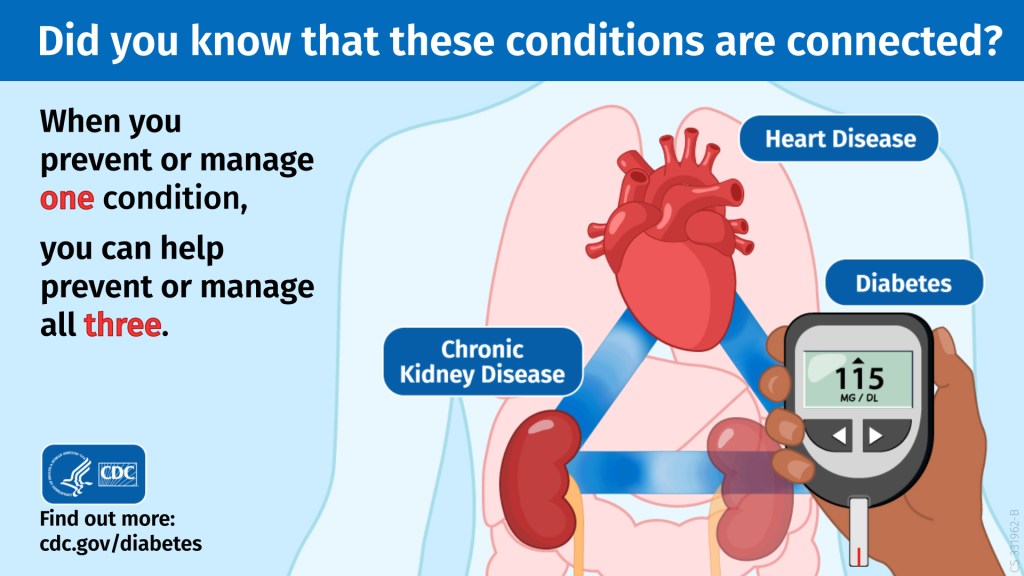
The body is complicated! While organs in your body each have a specific job to do to keep you healthy, they still rely on each other to function well. When one organ isn’t working the way it should, it can put stress on other organs, causing them to stop working properly as well.
The relationship between chronic kidney disease (CKD), diabetes, and heart disease is one example of the ways our organs are connected.
The body uses a hormone called insulin to get blood sugar into the body’s cells to be used as energy. If someone has diabetes, their pancreas either doesn’t make enough insulin or can’t use the insulin it makes as well as it should.
If someone has CKD, their kidneys are not able to filter out toxins and waste from their blood as well as they should.
Heart disease refers to several types of heart conditions. The most common condition, coronary artery disease, leads to changes in blood flow to the heart, which can cause a heart attack.
Make the Connection
So how are these three conditions connected? Risk factors for each condition are similar and include high blood sugar, high blood pressure, family history, obesity, unhealthy diet, and physical inactivity.
High blood sugar can slowly damage the kidneys, and, over time, they can stop filtering blood as well as they should, leading to CKD. Approximately 1 in 3 adults with diabetes has CKD.
When the kidneys don’t work well, more stress is put on the heart. When someone has CKD, their heart needs to pump harder to get blood to the kidneys. This can lead to heart disease, the leading cause of death in the United States. Change in blood pressure is also a CKD complication that can lead to heart disease.
Luckily, preventing or managing one condition can help you prevent and manage the others and lower the risk for more complications.
The American Heart Association (AHA) recently revised its checklist for achieving optimal heart health, introducing its new Life’s Essential 8. The list replaces the AHA’s decade-old Life’s Simple 7.
Sleep health is the new addition to the cardiovascular health scoring tool, which now advises that adults get seven to nine hours per night. The organization updated four of the categories:
Diet: More emphasis was given to following heart-healthy diets like the DASH and Mediterranean.
Nicotine exposure: Secondhand smoke and vaping were added as risk factors.
Blood lipids: People now can get a non-fasting blood sample that measures total, HDL, and non-HDL cholesterol. Non-HDL cholesterol can provide similar risk information as LDL cholesterol.
Blood sugar: Measurements now include hemoglobin A1c, a key component to assessing type 2 diabetes risk.
Three categories were unchanged:
Physical activity: The optimal weekly level is at least 150 minutes of moderate activity or 75 minutes of vigorous activity.
Body mass index (BMI): A BMI of 18.5 to 24.9 is ideal for heart health.
Blood pressure: Levels less than 120/80 millimeters of mercury (mm Hg) remain optimal. Stage 1 hypertension is 130 to 139 mm Hg for systolic pressure (the first number) or 80 to 89 mm Hg for diastolic pressure (the second number).
You can calculate your heart health score at mlc.heart.org. The guidelines were published online June 29, 2022, by Circulation.
Each year, medical diagnosis errors affect the health of millions of Americans and cost billions of dollars. Machine learning technologies can help identify hidden or complex patterns in diagnostic data to detect diseases earlier and improve treatments.
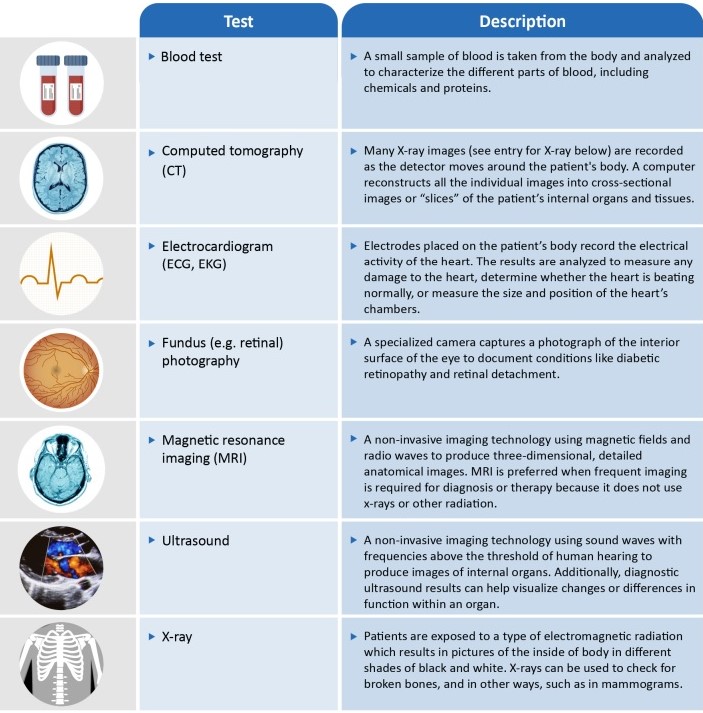
Several machine learning (ML) technologies are available in the U.S. to assist with the diagnostic process. The resulting benefits include earlier detection of diseases; more consistent analysis of medical data; and increased access to care, particularly for underserved populations. GAO identified a variety of ML-based technologies for five selected diseases
Certain cancers,
Diabetic retinopathy,
Alzheimer’s disease,
Heart disease,
COVID-19
Most technologies relying on data from imaging such as x-rays or magnetic resonance imaging (MRI). However, these ML technologies have generally not been widely adopted.
Cardiomyopathy is a disease of the heart muscle that makes it harder for the heart to pump blood to the rest of the body. Cardiomyopathy can lead to heart failure.
The main types of cardiomyopathy include dilated, hypertrophic and restrictive cardiomyopathy. Treatment — which might include medications, surgically implanted devices, heart surgery or, in severe cases, a heart transplant — depends on the type of cardiomyopathy and how serious it is.
There might be no signs or symptoms in the early stages of cardiomyopathy. But as the condition advances, signs and symptoms usually appear, including:
Breathlessness with activity or even at rest
Swelling of the legs, ankles and feet
Bloating of the abdomen due to fluid buildup
Cough while lying down
Difficulty lying flat to sleep
Fatigue
Heartbeats that feel rapid, pounding or fluttering
Chest discomfort or pressure
Dizziness, lightheadedness and fainting
Signs and symptoms tend to get worse unless treated. In some people, the condition worsens quickly; in others, it might not worsen for a long time.
Consuming just a half-tablespoon or more of olive oil a day is linked to a lower risk of dying from heart disease and other chronic health conditions, new research suggests.
The study included more than 92,000 women and men from the Nurses’ Health Study and the Health Professionals Follow-up Study, who filled out diet questionnaires every four years for 28 years. Olive oil intake was calculated from how much they reported using in salad dressings, on bread and other food, and in baking or frying.
Compared with participants who rarely or never consumed olive oil, those who consumed the most (about a half-tablespoon or more daily) had a 19% lower risk of dying from heart disease during the study. Researchers also noted lower death rates over all among people who substituted olive oil for a similar amount of margarine, butter, mayonnaise, or dairy fat. The findings, published Jan.18, 2022, in the Journal of the American College of Cardiology, lend further support for choosing olive oil — a key component of the heart-friendly Mediterranean diet.
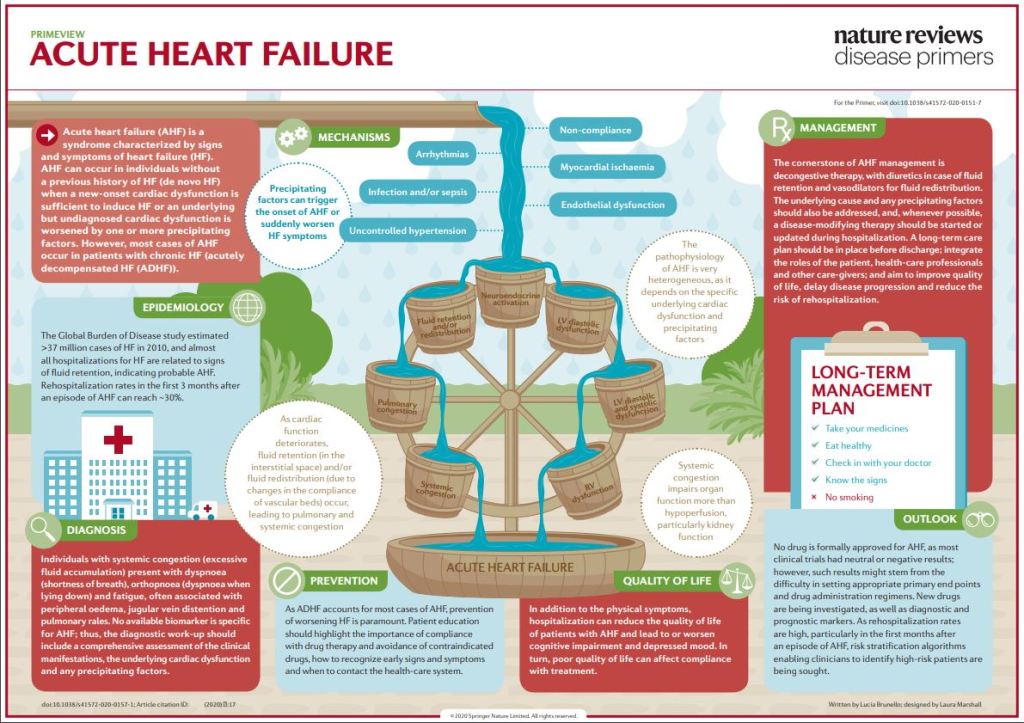
Acute heart failure (AHF) is a syndrome defined as the new onset (de novo heart failure (HF)) or worsening (acutely decompensated heart failure (ADHF)) of symptoms and signs of HF, mostly related to systemic congestion. In the presence of an underlying structural or functional cardiac dysfunction (whether chronic in ADHF or undiagnosed in de novo HF), one or more precipitating factors can induce AHF, although sometimes de novo HF can result directly from the onset of a new cardiac dysfunction, most frequently an acute coronary syndrome.
Despite leading to similar clinical presentations, the underlying cardiac disease and precipitating factors may vary greatly and, therefore, the pathophysiology of AHF is highly heterogeneous. Left ventricular diastolic or systolic dysfunction results in increased preload and afterload, which in turn lead to pulmonary congestion. Fluid retention and redistribution result in systemic congestion, eventually causing organ dysfunction due to hypoperfusion. Current treatment of AHF is mostly symptomatic, centred on decongestive drugs, at best tailored according to the initial haemodynamic status with little regard to the underlying pathophysiological particularities.
As a consequence, AHF is still associated with high mortality and hospital readmission rates. There is an unmet need for increased individualization of in-hospital management, including treatments targeting the causative factors, and continuation of treatment after hospital discharge to improve long-term outcomes.
COMMENTARY:
High frequency sound (ultrasound) bounces off of tissues, like an echo, and allows an electronic look at the heart. Doppler echocardiography is the doctors method of choice for evaluating a heart failure. One of the most important numbers determined by this method is the EJECTION FRACTION, which is a measure of heart efficiency. If the ejection fraction is low, let’s say below 45%, the heart is pumping out only 45% of its volume with each stroke, which means it must work harder to produce the same amount of circulation. The normal is about 60%.
This is the basis of SYSTOLIC Heart failure.
The test can also tell about blood coming into the heart; the early part of the blood entering is usually 80% of the total. If it drops, let’s say below 50%, it means the heart is stiff and resists blood coming in, which is the basis of DIASTOLIC heart failure.
FACES Is an acronym-mnemonic for the symptoms of heart failure. F is for FATIGUE.
A is for ACTIVITY LIMITATION. C is for CONGESTION in the lungs. E is for EDEMA, or swelling, usually of the ankles and legs. S is for SHORTNESS of BREATH.
If you want to remember a bit about heart failure, think about echoes and faces. If your Doctor orders an ultrasound with Doppler, be sure to ask about your ejection fraction and percent of blood that enters early, before the “atrial kick”. Being informed is always a good thing.
To be honest, I have never encountered a person who was given a Doppler echocardiogram and could tell me what his ejection fraction was, but I am eternally hopeful.
In December 2020, a week before cardiologist Stuart Katz was scheduled to receive his first COVID-19 vaccine, he came down with a fever. He spent the next two weeks wracked with a cough, body aches and chills. After months of helping others to weather the pandemic, Katz, who works at New York University, was having his own first-hand experience of COVID-19.
On Christmas Day, Katz’s acute illness finally subsided. But many symptoms lingered, including some related to the organ he’s built his career around: the heart. Walking up two flights of stairs would leave him breathless, with his heart racing at 120 beats per minute. Over the next several months, he began to feel better, and he’s now back to his normal routine of walking and cycling. But reports about COVID-19’s effects on the cardiovascular system have made him concerned about his long-term health. “I say to myself, ‘Well, is it really over?’” Katz says.
In one study1 this year, researchers used records from the US Department of Veterans Affairs (VA) to estimate how often COVID-19 leads to cardiovascular problems. They found that people who had had the disease faced substantially increased risks for 20 cardiovascular conditions — including potentially catastrophic problems such as heart attacks and strokes — in the year after infection with the coronavirus SARS-CoV-2. Researchers say that these complications can happen even in people who seem to have completely recovered from a mild infection.
Some smaller studies have mirrored these findings, but others find lower rates of complications. With millions or perhaps even billions of people having been infected with SARS-CoV-2, clinicians are wondering whether the pandemic will be followed by a cardiovascular aftershock. Meanwhile, researchers are trying to understand who is most at risk of these heart-related problems, how long the risk persists and what causes these symptoms.
COMMENTARY:
The heart and Covid are connected from a variety of angles.
Obese people with high blood fats, diabetes, the metabolic syndrome tend to have atherosclerosis and heart problems, making them more susceptible to severe Covid and long Covid. Covid loves to involve the lining of blood vessels and the heart, the endothelium, where the number of ACE receptors are high.
The respiratory tract and lung are a particular target for Covid, and reduced oxygen from lung involvement can compromise the hard-working heart.
Heart cells, cardio myocytes, can be directly infected with the virus. Even Covid vaccines can rarely produce myocarditis, raising the possibility that there is some antigenic similarity between the virus and heart cells, similar to the beta hemolytic streptococcus and the heart which sets up rheumatic fever.
If this similarity is real, the tendency of Covid to compromise the immune system and produce a cytokine storm in severe cases could therefore specifically involve the heart.
The nature article indicates several different varieties of heart problems and is a recommended read. From my personal standpoint, arrhythmias were mentioned, and I already have trouble with a couple of different types, AF and NSVT.
To make definite statements about the likelihood of heart involvement in Covid is problematic. The patients reported on were infected with an earlier strain of Covid, and the present one, BA.5, seems to be milder, and may not be as hard on the heart as previous strains. Many more people are now immunized, and the most susceptible patients may have passed away. There are medications to take, such as remdesivir, and even select immune globulins, such as an immuno-suppressed friend of mine was given when he contracted Covid recently.
The bottom line for me is that I am 90 years old and have no desire to let Covid have a crack at me, so I avoid big gatherings, and wear a mask whenever I am exposed.
The most common heart attack symptom in women is the same as in men — some type of chest pain, pressure or discomfort that lasts more than a few minutes or comes and goes.
But chest pain is not always severe or even the most noticeable symptom, particularly in women. Women often describe heart attack pain as pressure or tightness. And it’s possible to have a heart attack without chest pain.
Women are more likely than men to have heart attack symptoms unrelated to chest pain, such as:
Neck, jaw, shoulder, upper back or upper belly (abdomen) discomfort
Shortness of breath
Pain in one or both arms
Nausea or vomiting
Sweating
Lightheadedness or dizziness
Unusual fatigue
Heartburn (indigestion)
These symptoms may be vague and not as noticeable as the crushing chest pain often associated with heart attacks. This might be because women tend to have blockages not only in their main arteries but also in the smaller ones that supply blood to the heart — a condition called small vessel heart disease or coronary microvascular disease.
Postmenopausal women whose screening mammograms show signs of calcification in their breast arteries may have a higher risk of cardiovascular disease: https://t.co/iktQotQz5n#HarvardHealth
The routine mammograms women receive to check for breast cancer may also offer clues to their risk for heart disease, new research suggests.
White spots or lines visible on mammograms indicate a buildup of calcium in breast arteries. This breast arterial calcification is different from coronary artery calcification, which is known to be a marker for higher cardiovascular risk. For the study, researchers followed 5,059 postmenopausal women (ages 60 to 79) for six and a half years. They found that those with breast arterial calcification were 51% more likely to develop heart disease or have a stroke than those without calcification. The study was published March 15, 2022, in Circulation: Cardiovascular Imaging.
Empowering Patients Through Education And Telemedicine