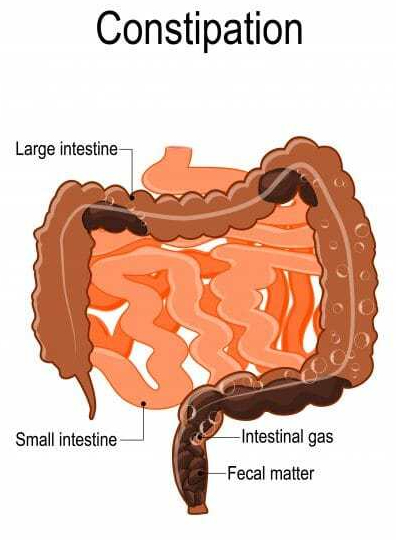
One of my previous posts, “bad breath”, was so well received that I am emboldened to deal briefly with another important, if politically incorrect, topic; Constipation.
I have anemia, and take regular IRON, which produces constipation. A high fiber diet solved it. My bones have also been thinning over the years into Osteopenia, a deficiency of Calcium. I Increased my calcium intake with some CALCIUM citrate powder, and developed one of the worst episodes of Constipation I have ever had, in spite of my high fiber diet.
Stopping the Calcium leaves me with the osteopenia worry, but was a great relief. Many other medications can cause constipation. Ask your Pharmacist for a list.` Hypothyroidism, and a variety of autoimmune, intestinal and neurological conditions have constipation as a symptom.
As I struggled with something that should be automatic, I worried about possibly pushing out a hernia, ballooning out one of my colonic diverticula, or developing hemorrhoids. These are all complications of constipation, not to mention the big waste of time. Regularity is much to be desired.
If you have regular SLEEP and EXERCISE a low Calorie density, high fiber diet, and are not taking a lot of drugs and supplements, you most likely don’t have constipation. If you have constipation, you might consider examining your sleep, diet, exercise and medications. If you don’t want to change your habits and medication, try METAMUCIL and drink lots of WATER.
Old age is an inevitable condition if you are lucky enough to live a long life. Middle aged people say it begins at 70 years of age. According to an Elysium survey of people 40 and older, the average American FEELS old for the first time at age 47 years.
In the distant past, 50 was CONSIDERED to be old. The generally better conditions and Medicine of modern times keeps extending LIFESPAN, if not always HEALTHSPAN. Old age is certainly a Condition, and it is for sure Chronic, thereby qualifying for inclusion, but is it a Disease?
It is not considered a disease by the authorities, and so it doesn’t gather research funds like it should. What exactly IS old age? Being 88 Years old, and a physician, I feel qualified to comment. Old age is a collection of past accidents and sports injuries plus complications of past illnesses engrafted on a gradually deteriorating body.
Where does Obesity and Metabolic syndrome fit in this rubric? The Plague of our time fits in the disease category. It is definitely preventable, although with difficulty. Please search past postings for more information on this topic.
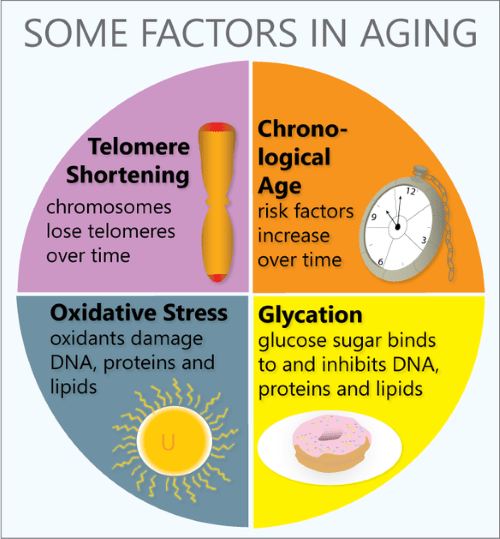
In what way does the body gradually deteriorate? Any organized, non-random high information structure gradually becomes more disordered, and “worn away” with the passage of TIME, the destroyer. Entropy (disorder) gradually increases, in the absence of corrective energy input.
Even rocks and mountains eventually erode, given enough time. One of the most interesting characteristics of life is that it maintains its integrity for an inordinate amount of time, given its complexity and furious dynamism.
Every day our DNA sustains thousands of molecular ruptures from high energy radiation and other stressors. Proofreading and repair mechanisms are employed, at high energy cost, to repair these breaks. This corrective is especially efficient when we are young and vigorous; In our youth, our reproductive years, growth and repair predominate. Gradually, growth ceases, repair mechanisms age, and we become old.
Our Darwinian “warranty” expires. We are left with an aging body, unimportant to evolution. We are long on experience and short on future. But we still have a marvelous metabolism at our disposal, depending on our lifestyle. There are a number of metabolic pathways which affect aging, 2 of which have been more studied.
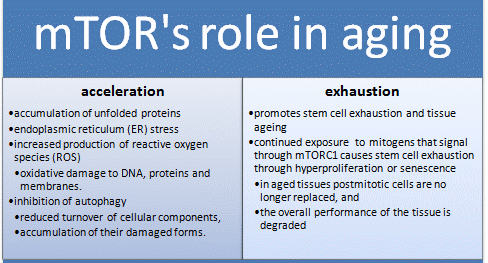
The mTOR pathway is most attuned to youth, senses nutrients and gears up for ANABOLISM, or growth. If you have not been careful to tailor your food intake to suit your decreasing requirements, your efficient metabolism stores it away for a rainy day, around your belly and in your arteries, a bad effect from an essential mechanism. Antagonistic Pleiotropy is the name for a body mechanism that can be good for one function (or age) and bad for another.
The Sirtuin system is also important in aging, and has a variety of housekeeping functions, including mitochondrial maintenance. It is activated by exercise. The cells of our bodies change with aging. In old tissues, there are less stem cells and other young, functional units. There are more damaged, dysfunctional “zombie” cells that don’t do much but promote inflammation, and hence more inflammatory cells accumulate.
Controlling the mTOR System and promoting the sirtuins help increase apoptosis and get rid of dysfunctional cells, including cancer. DOCTORS SHOULD PRESCRIBE EXERCISE, as well as SLEEP AND DIET, like they do medicine, and maybe we wouldn’t need so many pills. We might also feel better into old age.
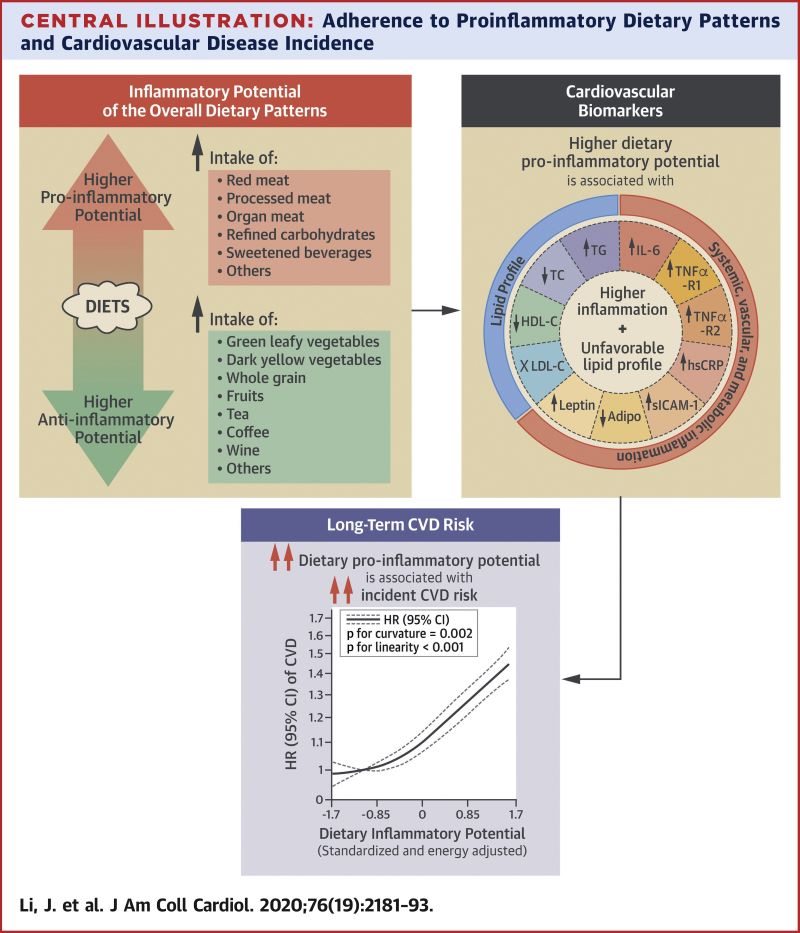
Dietary patterns with a higher proinflammatory potential were associated with higher CVD risk. Reducing the inflammatory potential of the diet may potentially provide an effective strategy for CVD prevention.
Background
Inflammation plays an important role in cardiovascular disease (CVD) development. Diet modulates inflammation; however, it remains unknown whether dietary patterns with higher inflammatory potential are associated with long-term CVD risk.
The number of older people, including those living with dementia, is rising, as younger age mortality declines. However, the age-specific incidence of dementia has fallen in many countries, probably because of improvements in education, nutrition, health care, and lifestyle changes.
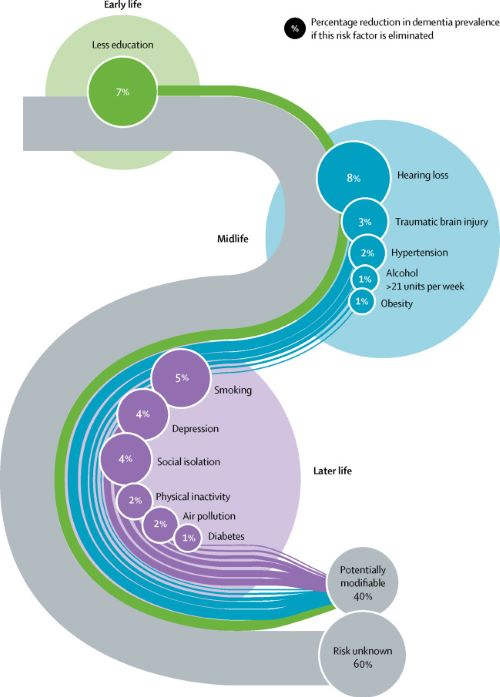
Overall, a growing body of evidence supports the nine potentially modifiable risk factors for dementia modelled by the 2017 Lancet Commission on dementia prevention, intervention, and care: less education, hypertension, hearing impairment, smoking, obesity, depression, physical inactivity, diabetes, and low social contact.
We now add three more risk factors for dementia with newer, convincing evidence. These factors are excessive alcohol consumption, traumatic brain injury, and air pollution. We have completed new reviews and meta-analyses and incorporated these into an updated 12 risk factor life-course model of dementia prevention. Together the 12 modifiable risk factors account for around 40% of worldwide dementias, which consequently could theoretically be prevented or delayed.
The potential for prevention is high and might be higher in low-income and middle-income countries (LMIC) where more dementias occur. Our new life-course model and evidence synthesis has paramount worldwide policy implications. It is never too early and never too late in the life course for dementia prevention. Early-life (younger than 45 years) risks, such as less education, affect cognitive reserve; midlife (45–65 years), and later-life (older than 65 years) risk factors influence reserve and triggering of neuropathological developments.
Culture, poverty, and inequality are key drivers of the need for change. Individuals who are most deprived need these changes the most and will derive the highest benefit.
Lancet’s 2017 Metanalysis mentions 9 Dementia risk factors. The 2020 Paper adds 3 additional factors. TRAUMATIC BRAIN INJURY, ALCOHOLISM, and AIR POLLUTION.
The inclusion of Trauma, with a 3% weighting, may be due to the increased awareness of TBE stemming from football injuries. The preventable 12 Factors are still in the minority. 60% of the factors are not preventable, since they are Genetically determined.
LESS EDUCATION, HEARING LOSS and SOCIAL ISOLATION, 3 of the original 9 factors,all lead to less brain stimulation, and can be unified under the idea of COGNITIVE RESERVE. If a person starts with less Cognition, it is reasonable to think he would be Demented sooner.
Together, less education, hearing loss, and social isolation account for almost Half of the correctable conditions. SMOKING is one of those things which impact almost every human disorder. It is amazing that cigarettes are still manufactured. In fact, their use is actually Increasing,especially the Far East, where they probably account for much of the escalating problem with Dementia in that region.
Our favorite causes, Sleep, Diet, and Exercise, apparently play only a minor role in Dementia. Sleep is completely dismissed in this report. The fact that both Sleeping less than the Ideal 7-8 hours, and more than that amount is thought to correlate with health problems is probably the main reason for the omission.
My own opinion is that people who are in poor health may need more sleep, and therefore sleep longer. My own sleep is interrupted 3-5 times per night, so it is not surprising that I need an hour extra to feel rested. Any less than 9-10 hours, and I need a nap, which in my opinion is a sign of insufficient nighttime sleep. Poor sleep may be a factor in metabolic syndrome, often leading to DIABETES, OBESITY, and HYPERTENSION, which are factors in Dementia, mentioned in the article as bit players.
PHYSICAL INACTIVITY is mentioned as a minor factor in Dementia, but exercise, studied as a treatment of dementia, was found to improve only strength. Diet is not mentioned, but does contribute to OBESITY, which is a minor factor. Dementia is a great emotional and economic burden, afflicting many otherwise happy families with misfortune.
The Lancet metanalysis is admirable. But don’t forget the healthy lifestyle emphasizing Sleep Diet and Exercise; and exercise includes cognitive exercise. Anything we can do to avoid dementia is worthwhile. –
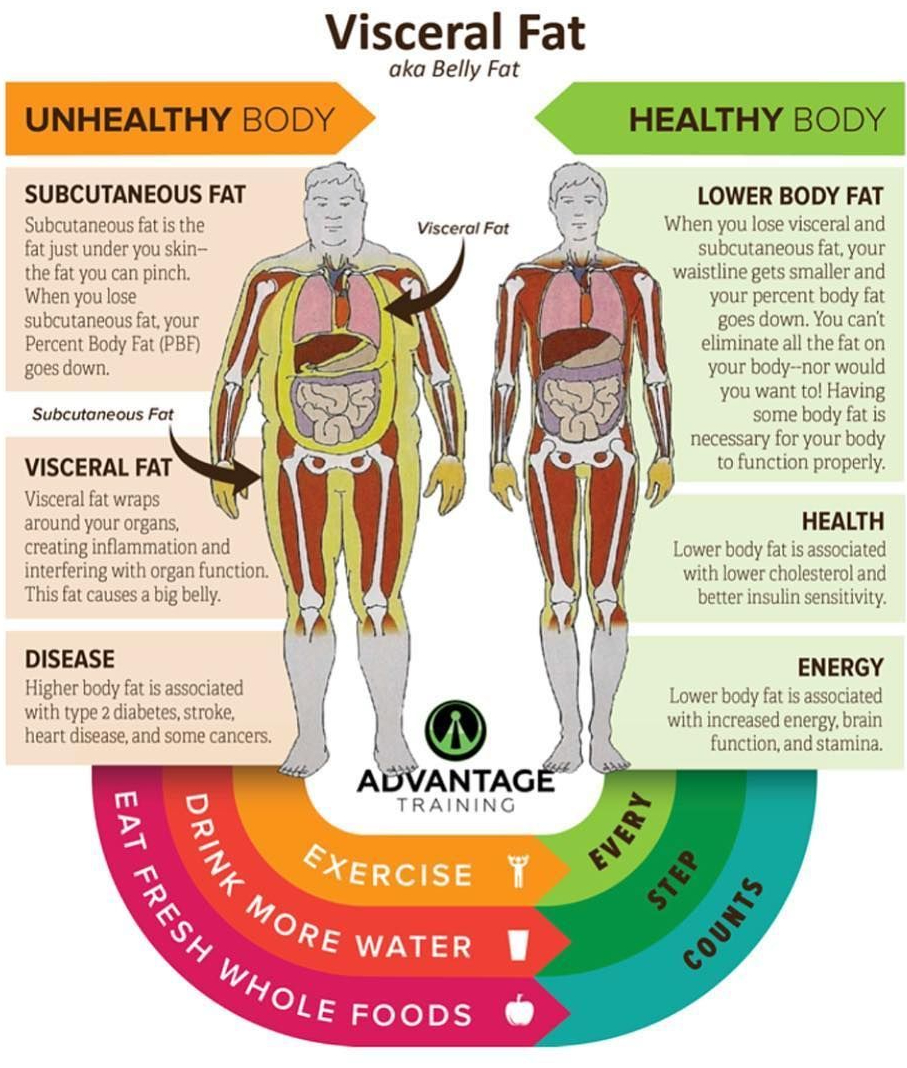
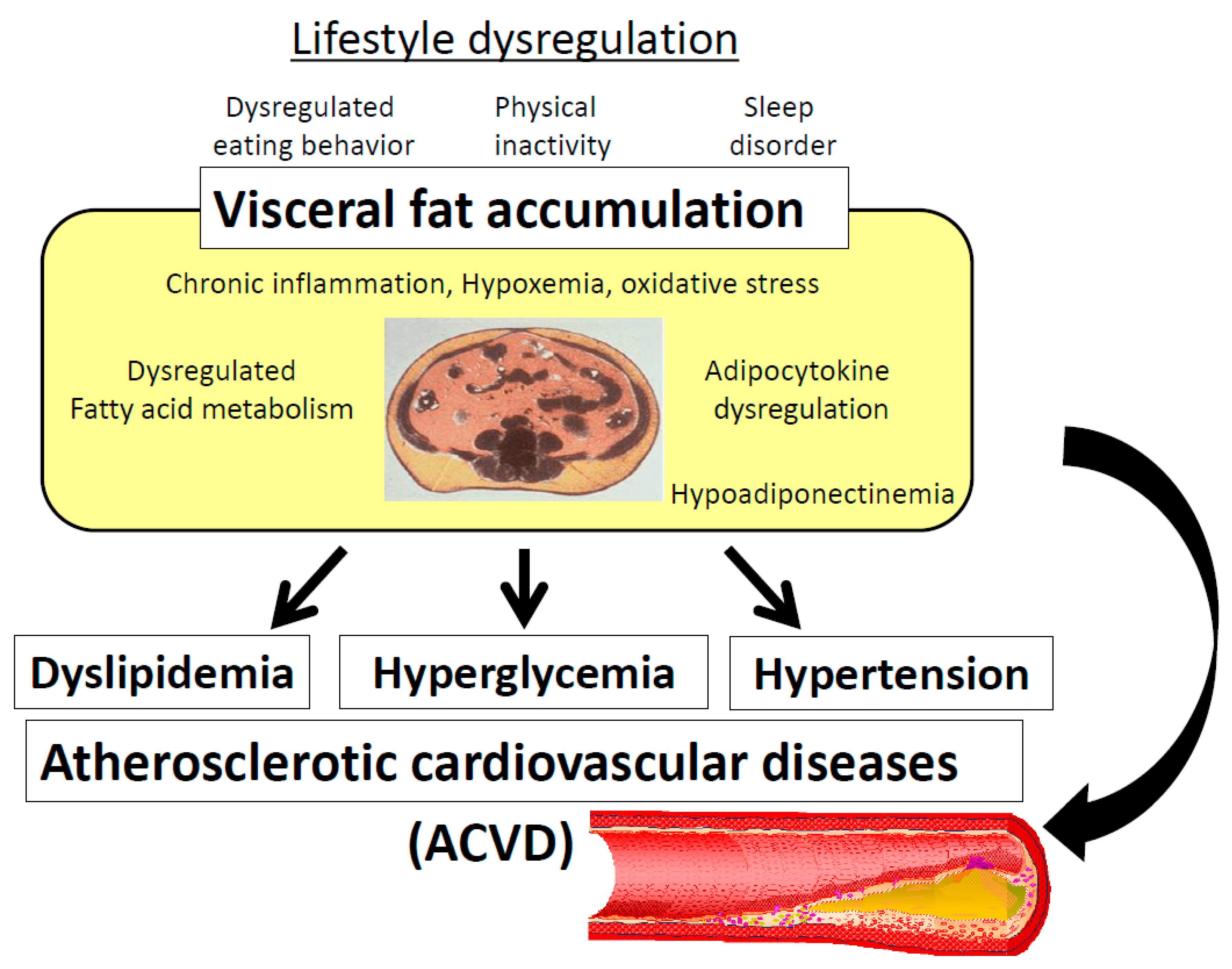
ABDOMINAL (VISCERAL) FAT KILLS. The following post tells you how, and suggests what you might do to prevent this scourge, which is gradually becoming an epidemic in America.
OBESITY is an energy imbalance problem. MORE CALORIES ARE CONSUMED THAN ARE NEEDED AND CAN BE UTILIZED. A Good quality Diet, with lots of natural (rather than processed) foods, especially vegetables and fruits, have lots of FIBER that takes up space and makes you feel full.
Fiber also feeds the MICROBIOME. If the foods are DIVERSE, the microbiome will also be diverse and help utilize the calories you eat. A healthy Microbiome also contributes to your health by manufacturing neurotransmitters, vitamins, and other factors that are just starting to be appreciated. Diet QUALITY, as well as quantity, is important.
EXERCISE is critical for more than utilizing calories. It increases ADIPONECTIN which guides fat to fat stores where they belong, rather than to the liver, and IRISIN which favors the production of BROWN FAT, thus utilizing energy. The opposite of exercise, the SEDENTARY LIFESTYLE, is now considered a disease system in itself.
Lack of SLEEP favors obesity in a number of ways; at the very least, you can’t eat while asleep. Abdominal fat contains INFLAMMATORY cells which go directly to the Liver via the hepatic portal system to cause metabolic disruption. Insulin sensitivity falls, blood sugar, LDL and triglycerides rise. DIABETES and the METABOLIC SYNDROME result.
The excessive weight also causes back, hip and knee problems which contribute to the 10% increase in overall medical costs due to Obesity.
We have no photographs, abdominal, navel-level girth measurements, CTs, BMIs or death certificates to prove it, but it is highly unlikely that Paleolithic Humans suffered from excessive abdominal fat. They had no refrigerators, deliciously packaged snacks, sugary, fructose-containing soft drinks and candy, nor did they have cave-lighting to extend their daylight eating hours and disrupt their diurnal rhythm.
They had to walk or run long distances to obtain their meagre food supplies, which tired them out so that they most likely had a good night’s sleep. SLEEP, DIET and EXERCISE are built into our Metabolism by Darwinian Evolution. Paleolithic humans didn’t live long lives and succumb to cancer and heart disease.
They died most often by violence, which made Blood clotting a survival benefit, rather than the Risk factor for stroke and heart attacks that coagulation is to us now. It is not all our fault that OBESITY is steadily increasing over the last few decades.
CAPITALISM is driven to provide us with ever increasingly available and tasty food. Both consumers and purveyors scream when even the most logical political check on OVEREATING is legislated: Taxing of sugary, fructose-containing, nutritionless soft drinks was tried in Philadelphia to a chorus of complaints. To my knowledge the tax has survived, reduced sugary drink consumption, and was helpful in reducing the weight of Philadelphia residents. Not many cities were brave enough to follow suit.
GENETIC Influences can also conspire against weight control. The FTO gene, while relatively infrequent does have an influence, as shown in twin studies. And there seems to be a SET POINT in weight that makes it difficult to take off the pounds and keep them off. 2 years after almost all diets, the weight has returned. Eating HABITS, once established are hard to change.
BARIATRIC SURGERY has been shown to help Obesity, as well as Metabolic syndrome and Diabetes .I hope it will survive the test of time. Weight gain is easier to PREVENT than it is to treat. Somehow, society must get to the children, and keep them from gaining weight in the first place. Even children are now becoming obese.
INTERMITTENT FASTING can help contain Obesity. My own version is TIME-RESTRICTED EATING. I limit my eating to 6 hours a day, from Noon (usually 1PM) until 6PM. This has resulted in a modest weight loss from 142 pounds to 137 pounds. My son lost some 30 pounds in a 30 day, 1000 calorie “crash” diet to fend off advised Back Surgery. He exercised a lot of SELF CONTROL both to lose the weight, and to keep it off.
Unfortunately, Self Control is in short supply in our present SOCIETY OF EXCESS. Good luck in your quest, if you choose to embark on weight reduction. And good luck with your health if you don’t. I recommend “the secret life of fat” by Sylvia Tara in either case. Also, search for intermittent fasting in DWWR.
Water, the miracle molecule, proteins and fats are the very essence of life. Water does not dissolve fat, allowing for the cell membranes, and the compartmentalization of metabolic activity that allows life to happen.
FAT IS ESSENTIAL TO LIFE. Alas, all fats are not equally beneficial to nutrition, as the article stresses. Trans-fats, partially hydrogenated fatty acids produced mainly by industry, are the worst, acting to stimulate cholesterol synthesis, produce inflammation and damage the endoplasmic reticulum.
Their use has been banned in most countries. Saturated fat has been widely condemned, is not as good as the mono- and polyunsaturated fats, but not as bad as trans-fats. Some of life’s most delicious foods, such as cheeses, contain saturated fats, but it is best to keep down their consumption.
Remember that the first bite of something savory tastes the best; prevent habit from shoveling it down. Unsaturated fats are found in oily fish, which should be part of your diet.
Vegetables such as nuts, seeds, olives, and avocados are sources of “good fat” and should comprise 10-15% of your calories. Fats, compared to carbohydrates, contribute almost twice as many calories to your diet on a weight basis, and it’s easy to get carried away.
Total calories must be kept under control. STAY HEALTHY!
According to a recent study, obesity increases the risk of dying of Covid-19 by nearly 50%. Governments around the world are now hoping to encourage their citizens to lose weight. But with so much complex and often contradictory diet advice, as well as endless food fads, it can be hard to know what healthy eating actually looks like.
How many pieces of fruit and vegetables should you eat a day? Will cutting out carbs help you lose weight? Is breakfast really the most important meal of the day? Speaking to Tim Spector, professor of genetic epidemiology at King’s College London about his new book Spoon-Fed, Madeleine Finlay asks why we’re still getting food science wrong, and explores the current scientific evidence on snacking, supplements and calorie labels.
Tim Spector is a Professor of Genetic Epidemiology and Director of the TwinsUK Registry at Kings College, London and has recently been elected to the prestigious Fellowship of the Academy of Medical Sciences. He trained originally in rheumatology and epidemiology. In 1992 he moved into genetic epidemiology and founded the UK Twins Registry, of 13,000 twins, which is the richest collection of genotypic and phenotypic information worldwide. He is past President of the International Society of Twin Studies, directs the European Twin Registry Consortium (Discotwin) and collaborates with over 120 centres worldwide. He has demonstrated the genetic basis of a wide range of common complex traits, many previously thought to be mainly due to ageing and environment. Through genetic association studies (GWAS), his group have found over 500 novel gene loci in over 50 disease areas. He has published over 800 research articles and is ranked as being in the top 1% of the world’s most cited scientists by Thomson-Reuters. He held a prestigious European Research Council senior investigator award in epigenetics and is a NIHR Senior Investigator. His current work focuses on omics and the microbiome and directs the crowdfunded British Gut microbiome project. Together with an international team of leading scientists including researchers from King’s College London, Massachusetts General Hospital, Tufts University, Stanford University and nutritional science company ZOE he is conducting the largest scientific nutrition research project, showing that individual responses to the same foods are unique, even between identical twins. You can find more on https://joinzoe.com/ He is a prolific writer with several popular science books and a regular blog, focusing on genetics, epigenetics and most recently microbiome and diet (The Diet Myth). He is in demand as a public speaker and features regularly in the media.
Sometimes I wake up in the morning with a feeling of RELAXED ENERGY. My mind is clear, I have no fatigue, and believe once more that the world is wonderful, and it’s great to be alive.
I St-re-tch, exercise my hands (I have Osteoarthritis, and they are stiff), take out my Nite guard ( I grind my teeth at night and would otherwise wear them away), take my beta blocker eye drops ( to lower my intraocular pressure) and wash down my Eliquis ( an anticoagulant to prevent stroke from my Atrial Fibrillation) with 16 oz. of water, while thinking about all of the delights awaiting me.
Yes, my body was in better shape 60 years ago; but I had much more responsibility then, and much less discretionary time. All things considered, I like to believe that I am happier now.
The KEY is to stay in GOOD HEALTH. GOOD SLEEP is critical, but it cannot be had by willpower alone. As I have discussed previously, you need a bedtime routine, good SLEEP HYGIENE.
You also need a…….. GOOD DIET. with lots of fruits, vegetables and whole grains. Fatty, spicy foods will stay in your stomach and bother you at night, particularly if you eat Late. I like to finish eating by 5 PM. Late dinner is also likely to produce GERD, and maybe Sleep Apnea.
GOOD EXERCISE is also critical. If you are not tired at the end of the day, it is hard to get good sleep. I always seem to sleep better on the day when I walk the hills for an hour, which is 3 days a week. Try not to exercise within 2 hours of bedtime. Assuming that you have a good base of SLEEP, DIET and EXERCISE, there are other mechanisms that can foul things up. INFLAMMATORY conditions often cause fatigue.
The most common inflammatory diseases are OBESITY, METABOLIC SYNDROME and DIABETES. OBESITY is the defining disease of our EXCESSIVE SOCIETY, where there is too much of everything, and excessive consumption is relentlessly advertised everywhere.
External correction is probably a pipe dream, since there is no will even to Tax Sugar-containing Beverages, the “low hanging fruit” of dietary excess. Internal correction is all that is left, and that takes WILL POWER, also in short supply.
INFECTIOUS DISEASES are a subset of inflammatory conditions. COVID 19 is the poster child of infection, and FATIGUE is one of the hallmarks of the disease. Interleukins, like TNF-alpha, IL-1, andIL-6 are some of the defense factors which cause the fatigue. AUTOIMMUNE Diseases like Rheumatoid Arthritis and Lupus are also associated with fatigue-producing interleukins.
Fatigue even has its own flagship disease, CHRONIC FATIGUE SYNDROME. Chronic viral disease has been suspected as the cause of this condition, and inflammatory cytokines may be elevated. This condition, and the similar GULF WAR SYNDROME are still poorly understood. Several CFS patients were sent to me when I was in practice, and I had some success in getting them to exercise regularly, which seemed to help. CANCER is another category of diseases where Fatigue is prominent.
Inflammation plays a role in these diseases, which also drain energy substrates from the Patients body; Cancer cells have a high metabolic requirement. MEDICATIONS, Cancer meds especially, but a variety of other Drugs are associated with FATIGUE. I went through MY MEDICATION LIST. Lo and behold, 3 of them are associated with fatigue.
Finasteride is a relic of my prostate operation, recommended to keep it from growing back. It causes fatigue, probably because of its ANTITESTOSTERONE effect. At least I can still pee, and am not bald. I take METFORMIN because of its fame in prolonging life. Its mechanism is that of interacting with the Sirtuin system, and increasing the inefficiency of mitochondria. Isn’t this surprising?
Like many other things in physiology, you place a stress on the body, and the body responds by improving its performance. If you are fatigued, you exercise. Respecting the body works with drugs as well. If you are drinking a ton of coffee and stop it, after a few weeks you will feel less fatigued.
And when you ARE FATIGUED, you drink a LITTLE coffee, and it wakes you right up. Caffeine works by displacing ADENOSINE, which causes Fatigue as it increases through the morning, peaking at SIESTA (or tea) time,at about 2 PM. OMEPRAZOLE, which I take to prevent HEARTBURN, also is related to fatigue especially if it blocks MAGNESIUM for long enough. DEPRESSION overlaps with fatigue, as does SLEEPINESS, to increase the complexity of the situation.
Many chronic LUNG, KIDNEY and LIVER diseases are associated with fatigue as a secondary concern. STAY HEALTHY!
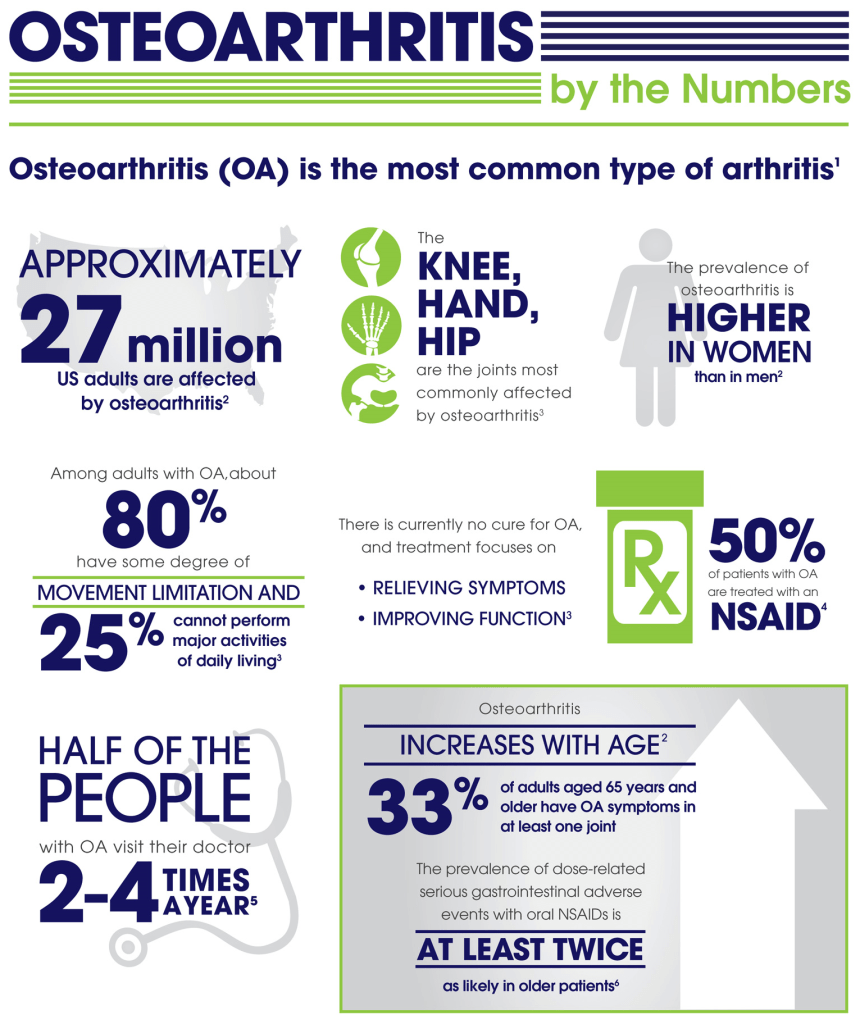
Osteoarthritis (OA) was considered a Degenerative disease when I went to Med School in the late 50s. I am more interested in OA since I have developed it myself.
There is a 40-60% hereditary component. My father’s mother had arthritis badly in her hands, as did my mother’s mother, and so on. A lot of genome-correlation work has shown many different genes involved,
But without a single big contributor, OA appears to be “multifactorial”, similar to a lot of common diseases like Diabetes l. Trauma can be a factor. Old sports injuries, like an ACL tear, that you thought a thing of the past, may come back to haunt you in later years.
INFLAMMATION, the most popular explanatory cause of the decade, may be operating in OA. For instance, you can imagine that OBESITY would contribute to hip and knee OA simply through the traumatic force of gravity. But obesity is also a disease of Inflammation, and increases IL-6 and other cytokines as well.
My own OA involves the classic distal 2 interphalangeal joints (go to the wikipedia manekin for a color-representation of OA classic locations). The base of my thumb, neck and back are also a problem.
Strangely, but wonderfully, my “wheels”, the Hips and Knees, are spared. I have exercised a lot in my life. Clearly, you can’t “wear out” your joints with ordinary exercise.
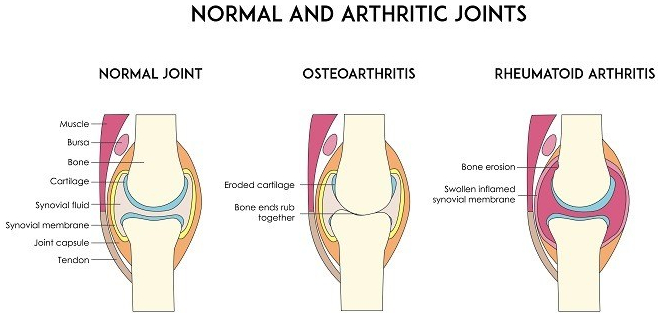
Our joints have evolved to allow us to move. Since bone has a lot of pain fibres, it would be painful to move the joints, directly bone-on-bone. So we have cartilage on the ends of the bones and discs between the vertebrae. The cartilage is slick to reduce friction.
Cartilage has no blood to supply it with nutrients. Instead, it relies on the joint (synovial) fluid. The cartilage is like a sponge. Walking alternately compresses and relaxes the spongy cartilage, increasing the synovial fluid circulation, thus improving the nutrition of the cartilage. If the Cartilage disappears, there is pain.
I am not a fan of pain medication. My belief was strengthened by the side effects of the study of a medication designed to genetically block pain transmission by injection into the painful joints. The side effect was virtual dissolution of the joints in a fraction of those treated. I felt more comfortable with my pain after reading the article.
Although Acetaminophen helps a little, NSAIDs usually work better, perhaps because of their anti-inflammatory action.
If, like me, you have stomach issues, there are the COX-2 inhibitors like Celebrex. The one dose I recently took was almost magical in its effects. Maybe if you don’t use pain Meds much, they work better.
I do take Glucosamine-Chondroitin, thinking that providing building blocks for cartilage couldn’t hurt. Along this line I also EAT CARTILAGE whenever I eat Chicken or ribs, being careful not to damage my teeth in the act of of exercising my jaws.
I also take Curcumin, hoping to relieve some pain, in spite of the fact that it is poorly absorbed (some brave souls take it by injection). I don’t know if any of this helps, How can you know in such a variable disorder, in the absence of controlled studies.
And pain has no OBJECTIVE markers, and is notoriously hard to study. We literally know more about the surface of mars than we know about Pain.
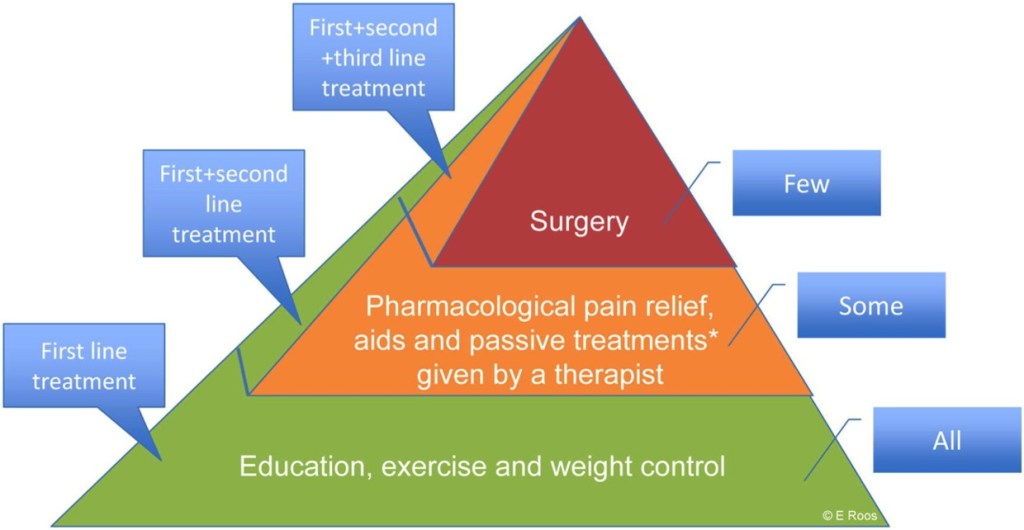
SLEEP, DIET, and EXERCISE, by minimizing OA factors kike OBESITY and INFLAMMATION are the best bet for preventing and treating OA at present.
–DR. C
Empowering Patients Through Education And Telemedicine