Chronic back pain and sciatica are very common, and increasing in prevalence. The human back does not seem to have been designed for obesity coupled with sedentary habits. I have had both back pain and sciatica . My wife had surgery in an attempt to control her back pain, my son successfully controlled his back pain with medical treatment, and an 87 year old friend recently had successful micro-neurosurgical treatment.
I will summarize these stories and will finish with some generalizations I believe will help those wanting to avoid a lot of misery. The sooner you start the better.
My back pain developed after an ill-advised use of a shovel to get rid of some grass intruding on my asphalt driveway, and caused me to miss work for the only day in 35 years of practice. Sciatica then developed on my left side. I could not sleep flat, and would sit all night in a comfortable chair. A hospital bed helped me outlast the impressive calf pain.
My wife developed severe back pain eventually leading to a “laminectomy and fusion”. Some level of back pain and incapacity plagued her the rest of her life.
My son developed severe sciatica and went to an Orthopedist. After a CAT scan revealed a rupture disc, he was penciled in for surgery. When asking about alternative treatments, the doctor told him, half laughingly, to lose 20% of his body weight and to start swimming. He went on a 30 day, 1000 calorie/day diet and lost 30 lbs. He has been swimming daily for the past 10 years. He has had no more back pain.

My 87 year old friend developed sciatica on his right side, had no luck with PT and pain meds including opioids. Microsurgery by a neurosurgeon successfully removed his ruptured disc, and he has had little or no pain after the first week.
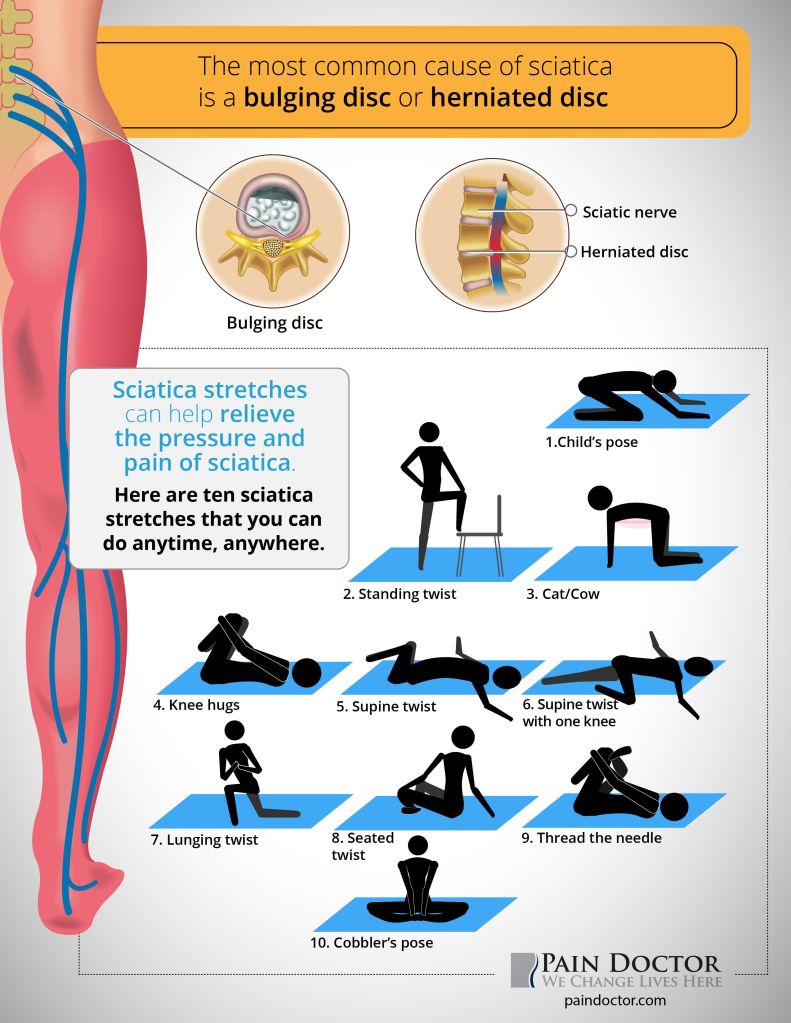
Sciatica at least has a well defined cause: something is irritating that long nerve which starts in the small of the back and travels to its’ destination in the foot. That something is often an extrusion from an intervertebral disc, a cushion between the block-like vertebral bodies.
This herniation can be confirmed by a CAT scan or MRI, and removed by minimally invasive microsurgery. Beyond that model problem, down through spinal stenosis and ending in chronic back pain, the understanding gets progressively more fuzzy, treatment ever more contrived.
Prevention sounds better and better. The most important thing in preventing back pain is to MAINTAIN A NORMAL WEIGHT. Our backs were not designed for vertically compressive forces. The lock-step increasing incidences of obesity and back/sciatic problems support this idea.
REGULAR EXERCISE is very important. Swimming and walking are 2 of the best forms of exercise. Exercises like running on hard surfaces, jumping in volleyball, and weight lifting seem less optimal.
The ABDOMINAL MUSCLES stabilize the spine, and prevent excessive motion. Walking and swimming both exercise and strengthen the abdominals.
Maintaining FLEXIBILITY and RANGE OF MOTION are important. flexibility will help prevent those unplanned, sudden motions from throwing your back out of alignment, or maybe generating a painful muscle tear.
Finally, getting into the habit of BENDING YOUR LEGS and tensing the stabilizing abdominals when you pick up something on the floor is a help.
I question the wisdom of back surgery for back pain alone, especially if accompanied by spinal fusion. Even when there is sciatica, the statistics show that treatment with surgery is no better than medical therapy after 2 years.
The development of microsurgical techniques may give surgery an edge, however. At the risk of cliche, AN OUNCE OF PREVENTION IS WORTH A POUND OF CURE.