

DR. C REVIEWS MAJOR HEALTH AND TELEMEDICAL NEWS FOR THE WEEK ENDING NOVEMBER 15, 2020.
Yearly Archives: 2020

THE DOCTORS 101 CHRONIC SYMPTOMS And CONDITIONS #23: OLD AGE / GROWING OLD
Old age is an inevitable condition if you are lucky enough to live a long life. Middle aged people say it begins at 70 years of age. According to an Elysium survey of people 40 and older, the average American FEELS old for the first time at age 47 years.
In the distant past, 50 was CONSIDERED to be old. The generally better conditions and Medicine of modern times keeps extending LIFESPAN, if not always HEALTHSPAN. Old age is certainly a Condition, and it is for sure Chronic, thereby qualifying for inclusion, but is it a Disease?
It is not considered a disease by the authorities, and so it doesn’t gather research funds like it should. What exactly IS old age? Being 88 Years old, and a physician, I feel qualified to comment. Old age is a collection of past accidents and sports injuries plus complications of past illnesses engrafted on a gradually deteriorating body.
Where does Obesity and Metabolic syndrome fit in this rubric? The Plague of our time fits in the disease category. It is definitely preventable, although with difficulty. Please search past postings for more information on this topic.
In what way does the body gradually deteriorate? Any organized, non-random high information structure gradually becomes more disordered, and “worn away” with the passage of TIME, the destroyer. Entropy (disorder) gradually increases, in the absence of corrective energy input.
Even rocks and mountains eventually erode, given enough time. One of the most interesting characteristics of life is that it maintains its integrity for an inordinate amount of time, given its complexity and furious dynamism.
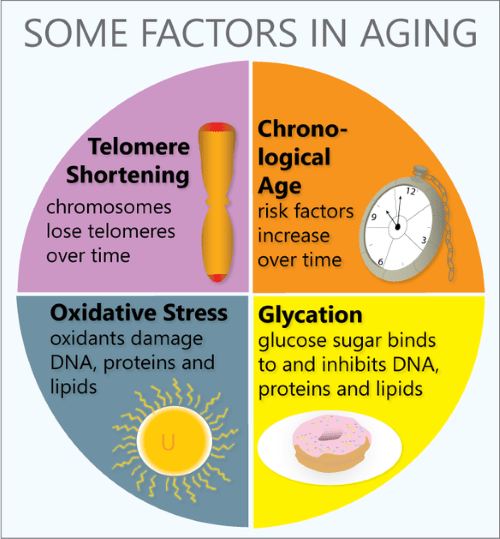
Every day our DNA sustains thousands of molecular ruptures from high energy radiation and other stressors. Proofreading and repair mechanisms are employed, at high energy cost, to repair these breaks. This corrective is especially efficient when we are young and vigorous; In our youth, our reproductive years, growth and repair predominate. Gradually, growth ceases, repair mechanisms age, and we become old.
Our Darwinian “warranty” expires. We are left with an aging body, unimportant to evolution. We are long on experience and short on future. But we still have a marvelous metabolism at our disposal, depending on our lifestyle. There are a number of metabolic pathways which affect aging, 2 of which have been more studied.
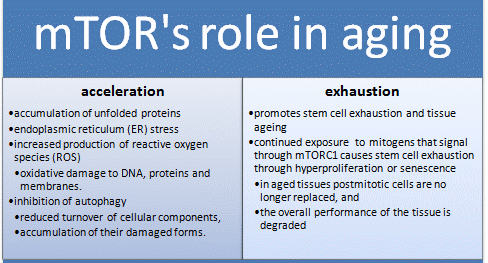
The mTOR pathway is most attuned to youth, senses nutrients and gears up for ANABOLISM, or growth. If you have not been careful to tailor your food intake to suit your decreasing requirements, your efficient metabolism stores it away for a rainy day, around your belly and in your arteries, a bad effect from an essential mechanism. Antagonistic Pleiotropy is the name for a body mechanism that can be good for one function (or age) and bad for another.
The Sirtuin system is also important in aging, and has a variety of housekeeping functions, including mitochondrial maintenance. It is activated by exercise. The cells of our bodies change with aging. In old tissues, there are less stem cells and other young, functional units. There are more damaged, dysfunctional “zombie” cells that don’t do much but promote inflammation, and hence more inflammatory cells accumulate.
Controlling the mTOR System and promoting the sirtuins help increase apoptosis and get rid of dysfunctional cells, including cancer. DOCTORS SHOULD PRESCRIBE EXERCISE, as well as SLEEP AND DIET, like they do medicine, and maybe we wouldn’t need so many pills. We might also feel better into old age.
–Dr. C.
Disease, Metabolic syndrome, Entropy, DNA, Metabolism, Apoptosis, Zombie cells

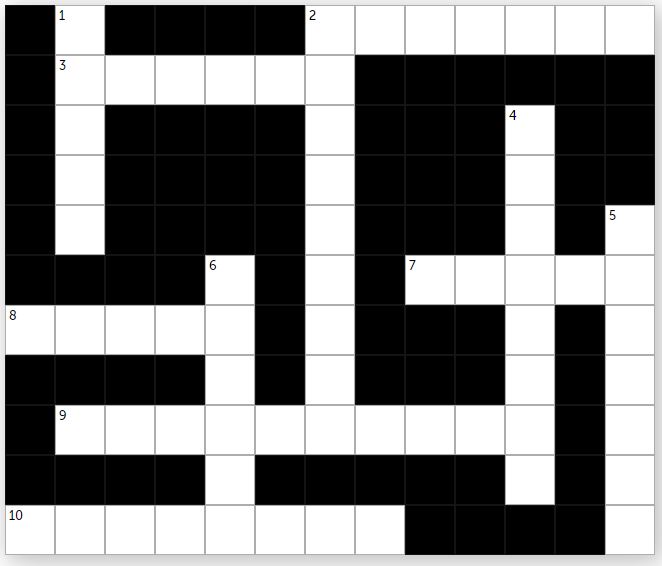
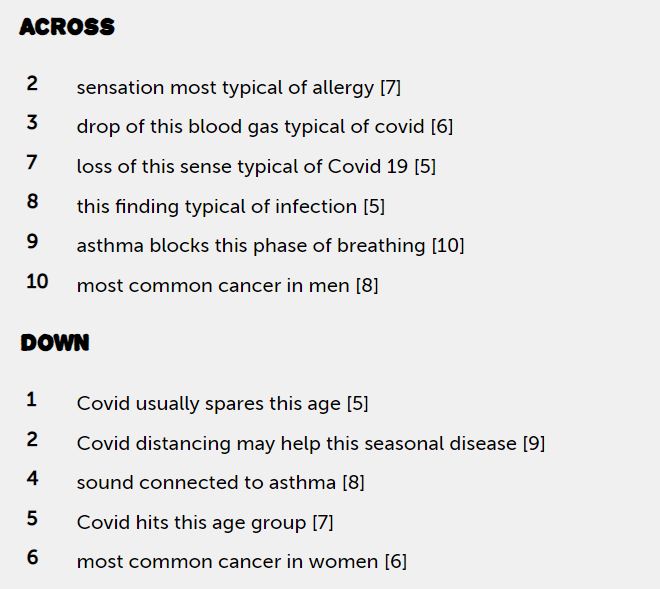
PATIENT EDUCATION: THE “2020 WEEKLY CROSSWORD PUZZLE CHALLENGE” (NOV 14)

HEALTH & RETIREMENT: A LOOK AT MEDICARE, MEDIGAP AND PART D DRUG PLANS

If you’re enrolled only in original Medicare with a Medigap supplemental plan, and don’t use a drug plan, there’s no need to re-evaluate your coverage, experts say. But Part D drug plans should be reviewed annually. The same applies to Advantage plans, which often wrap in prescription coverage and can make changes to their rosters of in-network health care providers.

“The amount of information that consumers need to grasp is dizzying, and it turns them off from doing a search,” Mr. Riccardi said. “They feel paralyzed about making a choice, and some just don’t think there is a more affordable plan out there for them.”
Is there another way?

When creation of the prescription drug benefit was being debated, progressive Medicare advocates fought to expand the existing program to include drug coverage, funded by a standard premium, similar to the structure of Part B. The standard Part B premium this year is $144.60; the only exceptions to that are high-income enrollees, who pay special income-related surcharges, and very low-income enrollees, who are eligible for special subsidies to help them meet Medicare costs.
“Given the enormous Medicare population that could be negotiated for, I think most drugs could be offered through a standard Medicare plan,” said Judith A. Stein, executive director of the Center for Medicare Advocacy.
“Instead, we have this very fragmented system that assumes very savvy, active consumers will somehow shop among dozens of plan options to see what drugs are available and at what cost with all the myriad co-pays and cost-sharing options,” she added.
Advocates like Ms. Stein also urged controlling program costs by allowing Medicare to negotiate drug prices with pharmaceutical companies — something the legislation that created Part D forbids.
COMMENTARY
Medicare is a blessing. It is a great help to retired and elderly people and generally does the job it was intended to do. There are a great variety of Medicare supplement plans and pharmaceutical purchase plans, And they jockey and change every year.
I get a headache just thinking about how to compare these plans from my individual needs and and whether their cost is worth it. The take-home message from the New York Times article is that you can get individual attention from an advisor who presumably knows the field well.
The key acronyms are SHIP and HICAP, which stands for state health insurance assist program and California health insurance counseling and advisor program respectively.
The California number is 1-800-434-0222. Be sure to write down the medications that you are taking and Your diagnosed illnesses, as well as your financial status in order to make best use of the service.
—Dr. C.

HEALTH: ‘RISKS & BENEFITS OF AI REVOLUTION IN MEDICINE’

It has taken time — some say far too long — but medicine stands on the brink of an AI revolution. In a recent article in the New England Journal of Medicine, Isaac Kohane, head of Harvard Medical School’s Department of Biomedical Informatics, and his co-authors say that AI will indeed make it possible to bring all medical knowledge to bear in service of any case.
Properly designed AI also has the potential to make our health care system more efficient and less expensive, ease the paperwork burden that has more and more doctors considering new careers, fill the gaping holes in access to quality care in the world’s poorest places, and, among many other things, serve as an unblinking watchdog on the lookout for the medical errors that kill an estimated 200,000 people and cost $1.9 billion annually.
“I’m convinced that the implementation of AI in medicine will be one of the things that change the way care is delivered going forward,” said David Bates, chief of internal medicine at Harvard-affiliated Brigham and Women’s Hospital, professor of medicine at Harvard Medical School and of health policy and management at the Harvard T.H. Chan School of Public Health. “It’s clear that clinicians don’t make as good decisions as they could. If they had support to make better decisions, they could do a better job.”
THE DOCTORS 101 CHRONIC SYMPTOMS & CONDITIONS #22: MIGRAINE HEADACHE
Migraine Headache in its classic form is a unique syndrome, or grouping of symptoms. There is often a PRODROME of anxiety, mood changes or fatigue a day or two before the Headache. There may also be an AURA, such as visual or other sensory symptoms, preceding the headache by minutes.

The Headache is often ONE-SIDED (hence the name, HeMigraine). The Headache is SEVERE, and accompanied by NAUSEA AND VOMITING, a “sick” Headache.
There are a variety of TRIGGERS, such as ripened Cheeses, Red wine, Nitrate-containing foods like hot dogs and pepperoni, and missing your cup of coffee. Stress and Hormonal Changes (menstrual periods) may trigger Migraine.
Migraine often has a FAMILY HISTORY. If one parent has migraine, the risk is 50%, and if both parents, 75%. It is more common in women. During the Headache, Migraine sufferers often seek out a quiet, dark room, and avoid stimulation.
My own experience with Migraine is with isolated OPHTHALMIC MIGRAINE. I have the aura, but luckily have no pain. In my day, 50 years ago, Migraine was considered a Vascular Headache Problem, with Vasodilation being the cause. Many triggers result in Vasodilation.
After a half century of intense study, including the discovery of Calcitonin Gene Related Product (CGRP) in the blood during Migraine, It is now considered a NEUROVASCULAR Headache Problem, and there is optimism for future progress.
TREATMENT can be to abort, to shorten the attack after the warning Prodrome or Aura start. If the attacks are too frequent, such as several times a week,
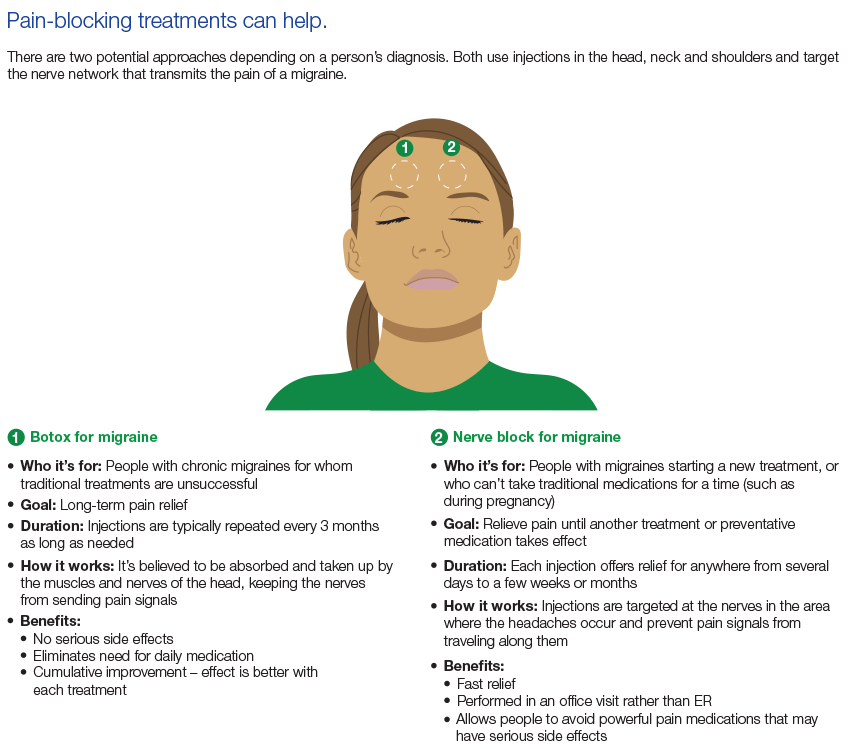
PREVENTATIVE treatment may be needed. Medications include a host of chemicals, including Hormones, and most recently, CGRP. Many of these chemicals are vasoconstrictors, which narrow blood vessels.
Please refer to the Mayo Clinic article for more information.
–Dr. C
PATIENT EDUCATION: THE “2020 WEEKLY CROSSWORD PUZZLE CHALLENGE” (NOV 10)
DR. C’S PODCAST: WEEKLY MEDICAL NEWS (NOV 9)
DR. C REVIEWS MAJOR HEALTH AND TELEMEDICAL NEWS FOR THE WEEK ENDING NOVEMBER 9, 2020.

INFOGRAPHIC: EXERCISE FOR ‘CLAUDICATION’ (BMJ STUDY)
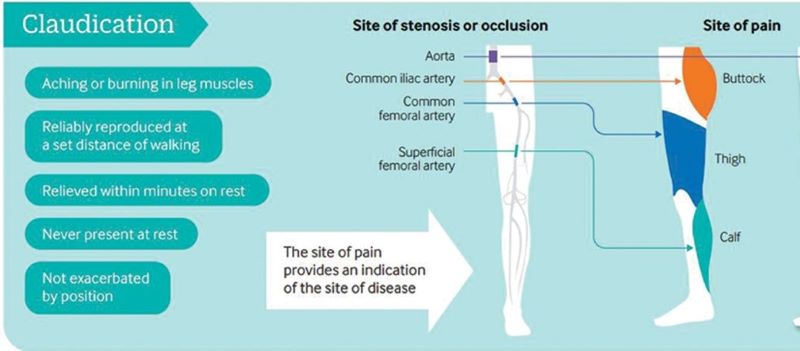
Exercise training is a safe, effective and low-cost intervention for improving walking ability in patients with IC. Additional benefits may include improvements in QoL, muscle strength and cardiorespiratory fitness. Clinical guidelines advocate supervised exercise training as a primary therapy for IC, with walking as the primary modality.
However, evidence is emerging for the role of various other modes of exercise including cycling and progressive resistance training to supplement walking training. In addition, there is emerging evidence for home-based exercise programmes. Revascularisation or drug treatment options should only be considered in patients if exercise training provides insufficient symptomatic relief.
Abstract
Peripheral artery disease (PAD) is caused by atherosclerotic narrowing of the arteries supplying the lower limbs often resulting in intermittent claudication, evident as pain or cramping while walking. Supervised exercise training elicits clinically meaningful benefits in walking ability and quality of life. Walking is the modality of exercise with the strongest evidence and is recommended in several national and international guidelines. Alternate forms of exercise such as upper- or lower-body cycling may be used, if required by certain patients, although there is less evidence for these types of programmes. The evidence for progressive resistance training is growing and patients can also engage in strength-based training alongside a walking programme. For those unable to attend a supervised class (strongest evidence), home-based or ‘self-facilitated’ exercise programmes are known to improve walking distance when compared to simple advice. All exercise programmes, independent of the mode of delivery, should be progressive and individually prescribed where possible, considering disease severity, comorbidities and initial exercise capacity. All patients should aim to accumulate at least 30 min of aerobic activity, at least three times a week, for at least 3 months, ideally in the form of walking exercise to near-maximal claudication pain.

COVID-19 VIDEO: ‘CRITICAL CORONAVIRUS-BUSTING THERAPIES EXPLAINED’
Health experts say having a vaccine is just one front in a two-front battle against COVID-19. The other is effective treatments for those who are already sick with the disease. WSJ breaks down the three most promising types in development. Photo Illustration: Jacob Reynolds/WSJ.
