

Osteoarthritis (OA) was considered a Degenerative disease when I went to Med School in the late 50s. I am more interested in OA since I have developed it myself.
There is a 40-60% hereditary component. My father’s mother had arthritis badly in her hands, as did my mother’s mother, and so on. A lot of genome-correlation work has shown many different genes involved,
But without a single big contributor, OA appears to be “multifactorial”, similar to a lot of common diseases like Diabetes l. Trauma can be a factor. Old sports injuries, like an ACL tear, that you thought a thing of the past, may come back to haunt you in later years.
INFLAMMATION, the most popular explanatory cause of the decade, may be operating in OA. For instance, you can imagine that OBESITY would contribute to hip and knee OA simply through the traumatic force of gravity. But obesity is also a disease of Inflammation, and increases IL-6 and other cytokines as well.
My own OA involves the classic distal 2 interphalangeal joints (go to the wikipedia manekin for a color-representation of OA classic locations). The base of my thumb, neck and back are also a problem.
Strangely, but wonderfully, my “wheels”, the Hips and Knees, are spared. I have exercised a lot in my life. Clearly, you can’t “wear out” your joints with ordinary exercise.
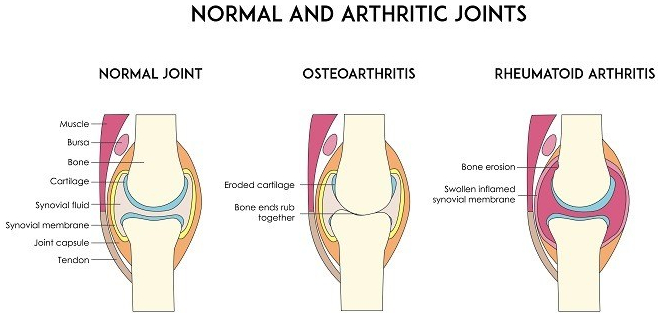
Our joints have evolved to allow us to move. Since bone has a lot of pain fibres, it would be painful to move the joints, directly bone-on-bone. So we have cartilage on the ends of the bones and discs between the vertebrae. The cartilage is slick to reduce friction.
Cartilage has no blood to supply it with nutrients. Instead, it relies on the joint (synovial) fluid. The cartilage is like a sponge. Walking alternately compresses and relaxes the spongy cartilage, increasing the synovial fluid circulation, thus improving the nutrition of the cartilage. If the Cartilage disappears, there is pain.
I am not a fan of pain medication. My belief was strengthened by the side effects of the study of a medication designed to genetically block pain transmission by injection into the painful joints. The side effect was virtual dissolution of the joints in a fraction of those treated. I felt more comfortable with my pain after reading the article.
Although Acetaminophen helps a little, NSAIDs usually work better, perhaps because of their anti-inflammatory action.
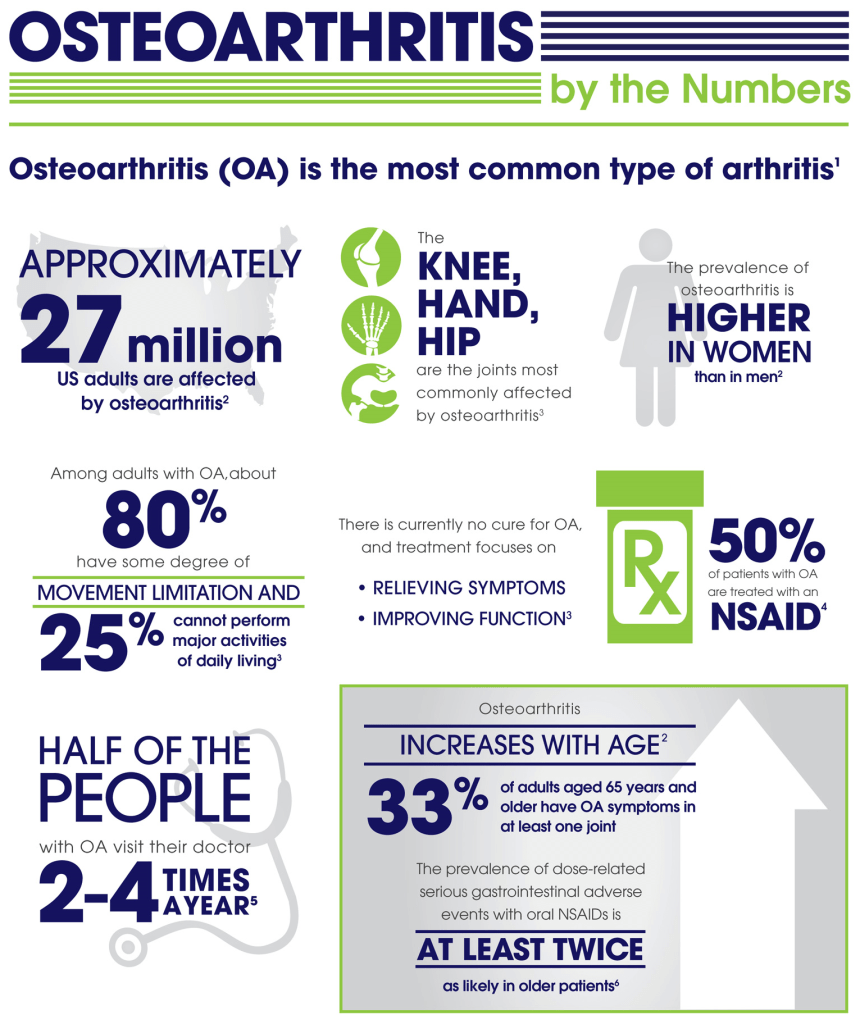
If, like me, you have stomach issues, there are the COX-2 inhibitors like Celebrex. The one dose I recently took was almost magical in its effects. Maybe if you don’t use pain Meds much, they work better.
I do take Glucosamine-Chondroitin, thinking that providing building blocks for cartilage couldn’t hurt. Along this line I also EAT CARTILAGE whenever I eat Chicken or ribs, being careful not to damage my teeth in the act of of exercising my jaws.
I also take Curcumin, hoping to relieve some pain, in spite of the fact that it is poorly absorbed (some brave souls take it by injection). I don’t know if any of this helps, How can you know in such a variable disorder, in the absence of controlled studies.
And pain has no OBJECTIVE markers, and is notoriously hard to study. We literally know more about the surface of mars than we know about Pain.
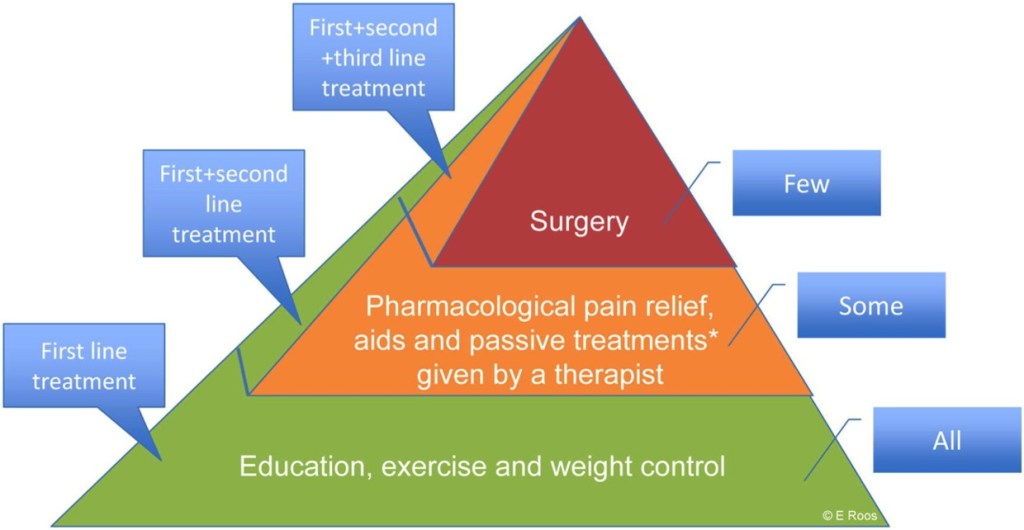
SLEEP, DIET, and EXERCISE, by minimizing OA factors kike OBESITY and INFLAMMATION are the best bet for preventing and treating OA at present.


