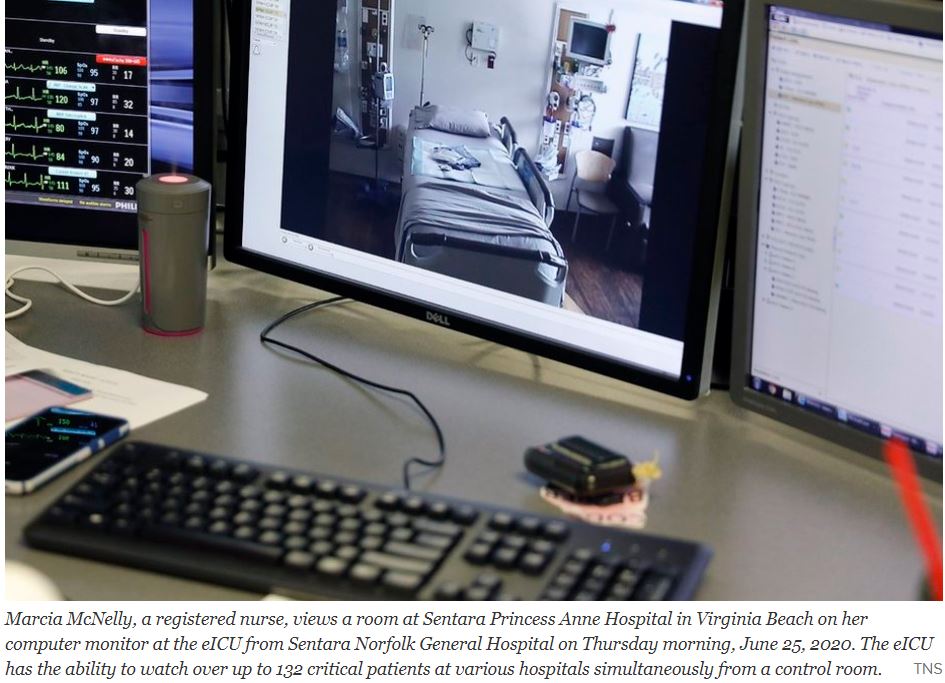
The hospital system — the first in the country — wired bedside video cameras and microphones on a secure network in 2000 so a medical team could monitor patients at multiple hospitals’ intensive care units from one command center around the clock.
When Sentara Healthcare first launched its “eICU,” the plan was to provide an extra set of eyes on critical patients, especially overnight when staffing was down to a skeleton crew.
Before the coronavirus arrived in Virginia, the average number of telemedicine visits within Sentara Medical Group was about 20 a day. Now, it is more than 2,000 a day, according to the company. Between March and June 21, its clinicians had 314,000 total patient visits, with about 51 percent of them happening virtually.
Telemedicine has been slowly developing for 10 or 20 years. The models have been developing according to the requirements of their local areas.
Dartmouth deals with a rural area and has sophisticated aid to it’s associated hospitals and transportation systems to bring Stabilized patients to the main hospital.
Sentara deals with a more urban area and has a central brain aiding the peripheral hospitals in the delivery of treatment locally.
The Tele intensive care unit system of Santara features a central ” Mission Control” With patients in multiple peripheral Intensive care units connected by telemetry. This efficient system allows the peripheral ICUs to operate at a higher level with less staff.
Such telemetry could allow convalescent hospitals and even nursing homes to improve medical care.
With such excellent models one can hope that American medicine will rapidly improve in the post Covid era, riding the wave of telehealth advances.
On the 100th anniversary of the Band-Aid, Tufts engineer Sameer Sonkusale is working to make “smart” bandages.
COMMENTARY
The Tuft’s video talks about transforming the Band-Aid into a detector that can warn of infection, or even exude the proper antibiotic. This would certainly be Applicable to Convalescent homes where people can’t monitor their own healing.
I am Looking forward to the time when the bandage will provide a matrix for the body’s regenerative cells to spread out and cover the wound more rapidly. Possibly someday the regenerative cells themselves can be applied.
An increasing number of hospitals are now equipping emergency vehicles to treat stroke patients while en route to the ER. UCHealth is a health system in Colorado that has a tricked-out ambulance, the Mobile Stroke Treatment Unit. A neurologist at the hospital is connected wirelessly through telehealth to the vehicle. First responders’ gear includes portable CT scanners and tPA.
Currently, there are also more than two dozen telestroke networks in the United States. At the hub of each is a large hospital with on-call neurologists, and broadband that connects the hospital directly to satellite hospitals and clinics. There’s always a neurologist on call to guide the smaller hospital staffs’ treatment of a stroke patient.
When I had a stroke five years ago at 10:20 on a Saturday night, telehealth saved my life. At the time, only 3% to 5% of people in the United States were able to get the “clot-busting” drug called tPA in time to avoid brain damage.
In addition to offering telestroke capabilities, healthcare providers should equip emergency vehicles with portable ultrasound devices and defibrillators. Rural communities can consider strategically deploying high-powered wired and wireless hotspots in case patients need immediate medical attention while still en route to the hospital. Following natural disasters such as earthquakes or floods, mobile hotspots configured for telehealth could be helicoptered into isolated communities.
SPEED is especially important when a blood clot blocks an artery servicing an important organ. Our Heart and BRAIN top the list of vital organs. TELESTROKE showcases Telemedicine at its best.
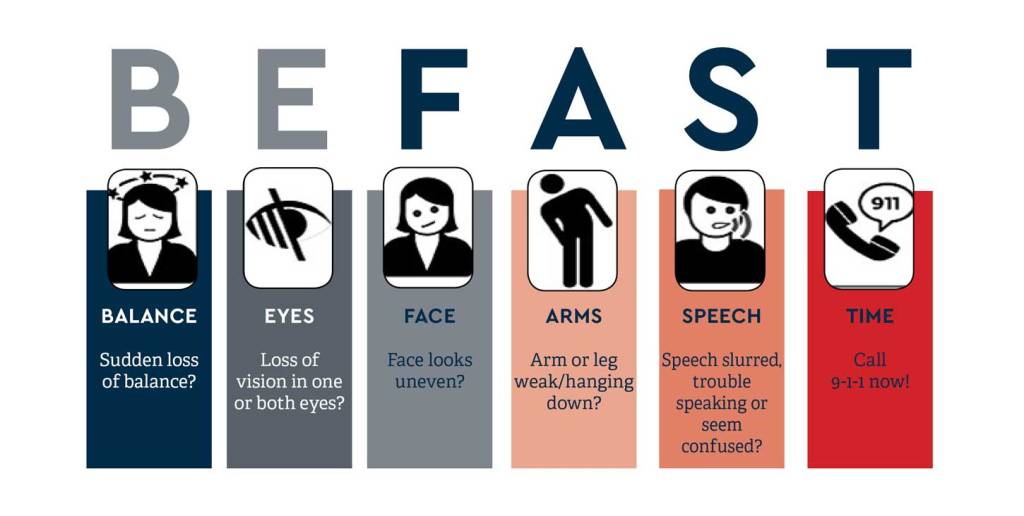
RECOGNITION of a stroke is a weak link in the chain of prompt Brainsaving treatment, and a Mnemonic helps.
—Facial assymetry or drooping —Arm or leg weakness on one side —Speech disturbance —Time is all important
FAST is a good mnemonic, and adding B for balance and E for Eye, or vision loss, for BEFAST gives 2 more parameters to think about.
Living alone adds to the challenge, so be as focused as you can. I was interested to hear that some TELESTROKE ambulances are adding mobile CT and drug (tpa) capabilities, in addition to TELECONFERENCING with a NEUROLOGIST. Treating a stroke within 15 minutes is becoming a possibility.
So particularly if you have risk factors such as hypertension, diabetes or obesity, be on the alert for symptoms of stroke.
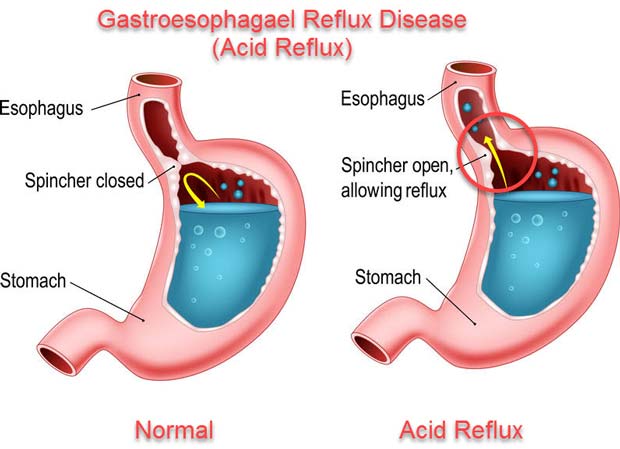
I have been having Heartburn for more than 40 years. The cause of Heartburn is leakage of acid from the stomach, where tissues have evolved to tolerate the highly acidic conditions, into the esophagus, where they haven’t.
The young body has an efficient, functional gate, or sphincter, keeping the food, once swallowed into the stomach, from coming back up. As you eat, you chew your food well to aid digestion. Your taste buds, sensing chemicals in the delicious food, activate saliva.
The salivary enzymes start the digestion of the carbohydrates in the food. If you eat slowly enough, you may be able to appreciate the digestion of tasteless starch, like in bread, into sweet sugar, right in your mouth.
You then swallow the food, which slips past another gate, called the epiglottis, diverting the bolus of food past your windpipe. This gate sometimes does not shut tight, and you choke on the food or drink. The food is then conducted into the highly acidic environment of the stomach.
The stomach evolved to be an acidic, “fiery pit”, inhospitable to any bacteria that came in with the food, thus protecting the stomach from infection. In the old days, there were a lot of bacteria, and the acidity of the stomach was useful, and evolutionarily conserved.
These days, the “fiery pit” tends to be a problem. As you get older, the gate that keeps food in the stomach gets more floppy and relaxed, and allows food to come back up into the esophagus, and sometimes, most often at night when you would rather be sleeping, all the way up to your throat, and is inhaled into your windpipe and lungs in what is called “gastroesophageal reflux”, or GERD.
Even if the food, and acid, doesn’t make it all the way up, and stops at the esophagus, which has not evolved to tolerate acid, you will have “heart burn”. Of course it is not the heart that is burning, but the esophagus, which runs right past the back of the heart as it goes all the way from the throat to the stomach.
When I first developed Heartburn, all that was available was the flavored chalk, Calcium Carbonate, sold as Tums. It works right away, and is a source of Calcium, but can cause trouble, like kidney stones, if you take too much. The relief didn’t last long enough for me, and I had to take more in the middle of the night.
My next medicine was Xantac, a medication that blocks histamine from stimulating acid production in the stomach. The H2 blockers have recently been recalled because of NDMA contamination. I sometimes used H2 blockers like Xantac when my patients would get a bad allergic reaction. In such cases BOTH an H1 blocker like Benadryl, and an H2 blocker are called for.
Zantac was not strong enough for me, and I soon graduated to Prilosec,which directly blocks the secretion of acid in the stomach.
Prilosec was then very expensive, but now is available as the inexpensive GENERIC Medication, Omeprazole. It seems that no medication is without side effects.
Omeprazole, by reducing stomach acid, makes stomach and GI infections more likely, and interferes with the absorption of B12, and Calcium.
If you have had a lot of heartburn over a long period of time, you should check with a Gastroenterologist, who may scope you to rule out Barritt’s esophagus, which can lead to Cancer.
It is interesting that the antacid Tums in excess can cause too MUCH Calcium in the body, and can cause kidney stones and other kidney problems like MAS, and Omeprazole, by interfering with absorption can cause too LITTLE absorption of Calcium, leading to OSTEOPOROSIS.
The best rule is to take as low a dose of ANY medication as possible, preferably none, to understand the possible side effects, and compensate for them if you can.
After surveying almost 800 gastroenterology and hepatology patients and their physicians at Penn Medicine, 67 percent of both viewed their video and telephone appointments held during the peak of the COVID-19 pandemic as positive and acceptable substitutes to in-person appointments.
From March 16 to April 10, 2020, 94 percent of gastroenterology and hepatology appointments at Penn Medicine were performed using telemedicine in order to mitigate risks of COVID-19 spread while continuing to advance care as patients self-isolated at home. A telemedicine visit meant either a video visit (similar to FaceTime or Skype) or one via phone in which clinicians largely performed routine and non-urgent care.
On a Friday afternoon last summer, a patient, “Barb,” texted me: “Call me. I can’t breathe.” As a heart failure nurse serving rural patients, getting messages like Barb’s launches my adrenaline. I called her immediately.
A month earlier, I’d trained Barb to send daily vital signs via my clinic’s digital portal—blood pressure, weight, heart rate, and oxygen saturation.
Barb was suffering from a congestive heart failure exacerbation: her lungs were filling with fluid. If we didn’t remove it, she’d need to be hospitalized or worse.
Once I was sure she wasn’t in emergency distress, I called the clinic’s cardiologist for instructions. Then I phoned Barb’s pharmacy and ordered a new diuretic to add to her regimen—a water pill so powerful in its fluid off-loading effect that I’ve nicknamed it the Bellagio. Within two hours, Barb had taken the pill and begun to urinate out the fluid flooding her lungs. By the next morning, she was breathing comfortably.
Without access to a telehealth program, Barb would probably have gone to the emergency room, then to the intensive care unit for expensive intravenous medications.
Lynsay Ayer, senior behavioral scientist with the RAND Corporation, describes how task sharing helps fill the need for more mental health care providers.