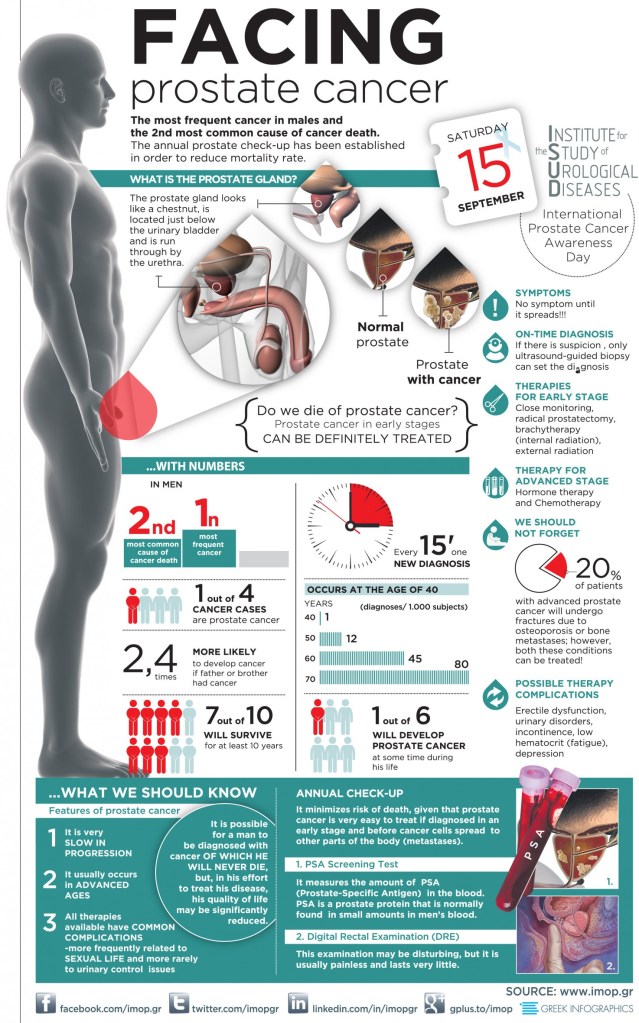
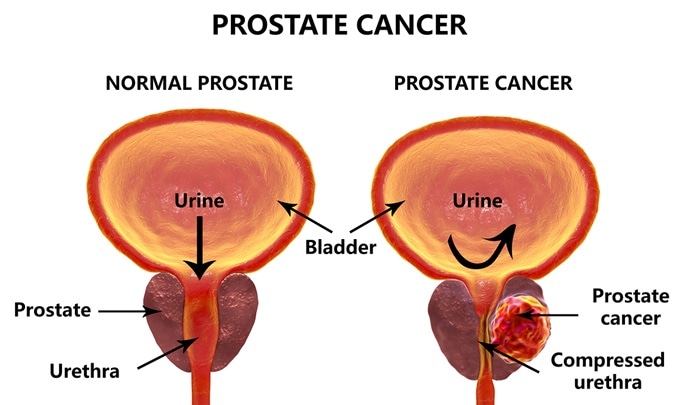
Prostate cancer is perhaps the most common cancer in men. It increases in incidence with age, and if you live long enough, most men will contract prostate cancer. A family history of cancer and obesity are also risk factors. But many times the cancer is so slow growing that it will not kill you. In the age of modern, aggressive medicine, the treatment has often been worse than the disease.
Treating Cancer EARLY is much more successful. The PSA test was one of the first really sensitive blood tests for cancer, and it was once performed routinely, on a yearly basis, usually at the time of your annual physical.
The PSA (Prostate-Specific Antigen) test is VERY sensitive,however. In responding to an elevated PSA, very slow growing tumors would often be treated aggressively, creating more morbidity than the untreated tumor would have caused.
The treatment seemed to be worse than the disease. Many physicians stopped doing the PSA test altogether, relying on symptoms, or detecting an abnormality on RECTAL EXAM to trigger an investigation. Some years ago, a physician friend of mine elected to stop PSA testing, and two years later was discovered to have METASTATIC Prostate cancer. It had already spread to his bones, and he eventually died of that cancer.
This encouraged me to continue with PSA screening, though it is still considered optional. Very recently, a test has been developed which I think tips the scales back toward annual PSA testing. EXOSOMES are little (10-120 nm.) particles that effuse from many cells, especially cancer cells.
They contain a variety of DNA, RNA, proteins and lipids which allow the cells to communicate with one another. Recently, a company, ExoDx, was created to take commercial advantage of Exosomes in the diagnosis of various diseases, by testing body fluids.
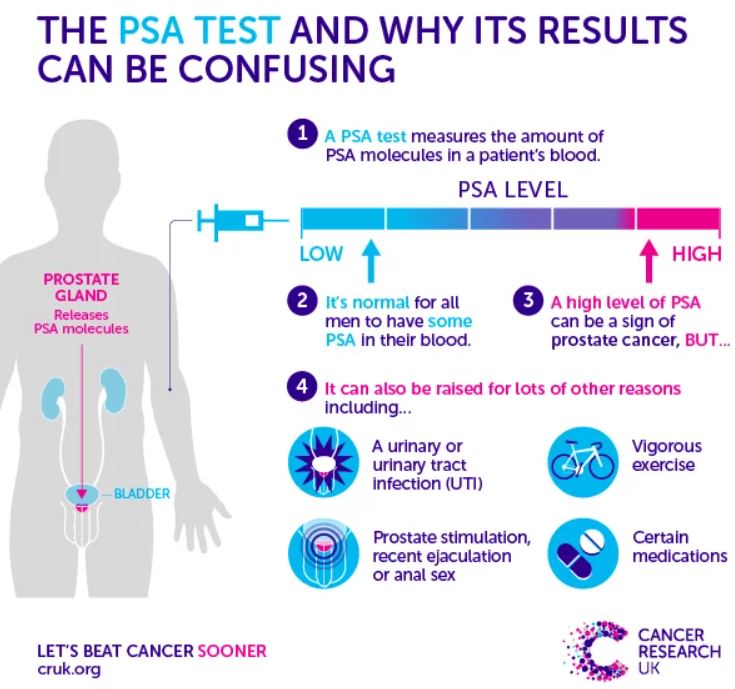
Their test, ExoRx Prostate EPI test of urine, has been shown to be helpful in distinguishing AGGRESSIVE prostate cancer from the slower growing kind, when the PSA test is in the “grey zone” between 2 and 10 ng/ml. PSA test results above 10 ng. were always acted on, especially if the numbers were increasing. I would be surprised if the PSA did not reenter the annual testing protocol.
The annual digital rectal exam in men older than 50 years will continue to be done, although it is not very sensitive, and is often not abnormal until the cancer is more advanced. Pain in the prostate area, blood in the urine or semen, and trouble urinating are symptoms worth investigating, but if cancer is detected, it may well be advanced and harder to treat. With abnormal tests,
Risk factors or suspicious symptoms, further testing is often done. Ultrasound or biopsy may be indicated. Sometimes the biopsy is guided by MRI, to increase the likelihood that the cancer, if small, is included in the tissue sample taken. Examining the cells of the biopsy sample will yield a “gleason score” which grades the aggressiveness of the cancer.
This in turn dictates the treatment, which may include different extents of surgical removal, radiation, hormonal or chemotherapy treatment. None of this is pleasant, and you are better off, of course with prevention.
Our old friends, DIET AND EXERCISE are thought to be helpful. Although not proven, eating lots of fruits and vegetables, and maintaining a healthy weight are recommended.
–DR. C