From a Wall Street Journal article (May 21, 2020):
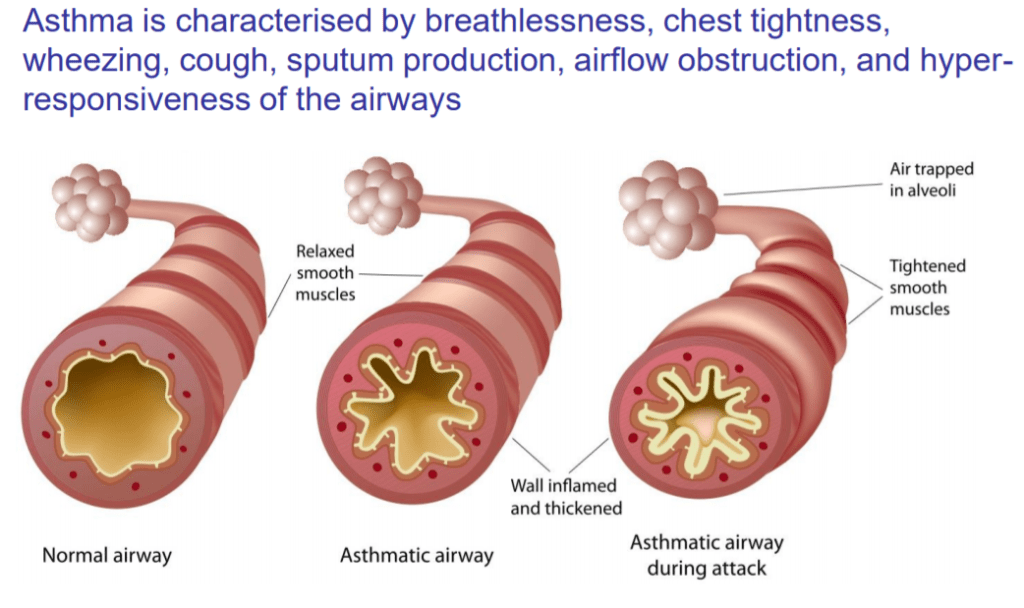
Breathing properly can allow us to live longer and healthier lives. Breathing poorly, by contrast, can exacerbate and sometimes cause a laundry list of chronic diseases: asthma, anxiety, attention deficit hyperactivity disorder, hypertension and more. Poor breathing habits can even change the physical structure of our skeletons, depleting essential minerals and weakening our bones.

Most of us misunderstand breathing. We see it as passive, something that we just do. Breathe, live; stop breathing, die. But breathing is not that simple and binary. How we breathe matters, too.
Last year, I wanted to see just how dramatically breathing habits—good and bad ones—could affect my own brain and body. I’d learned that up to 50% of us are chronic mouth breathers, a problem well described by an ancient Tao text: “The breath inhaled through the mouth is called ‘Ni Ch’i, adverse breath,’ which is extremely harmful.”
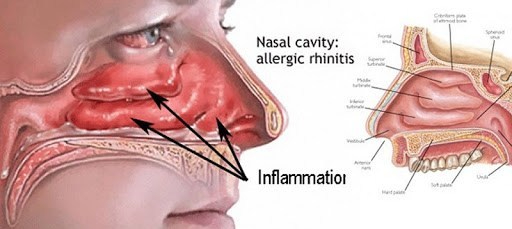
Scientists have known for decades that inhaling through this pathway saps the body of moisture, irritates the lungs and loosens the soft tissues at the back of the mouth. Mouth breathing has also been linked with neurological disorders, periodontal disease and increased risk of respiratory infection. But nobody knew how quickly this damage came on.
COMMENTARY
Breathing is something we don’t think about. It comfortably transcends the merely habitual, and there is a complex of controllers in the brain to Drive breathing should we be unable or forget to breathe voluntarily.
Breathing has it’s own poets and cults, one of which is MINDFULNESS MEDITATION, which uses our BREATHING as the focus of our consciousness, to get us outside ourselves.
With DEEP breathing, I noticed an INCREASED pO2, as registered on my Pulse Oximeter.
In the 1960’s asthma was not so well controlled as now. The mechanics of breathing were more important, so we taught our Patients how to breathe properly.
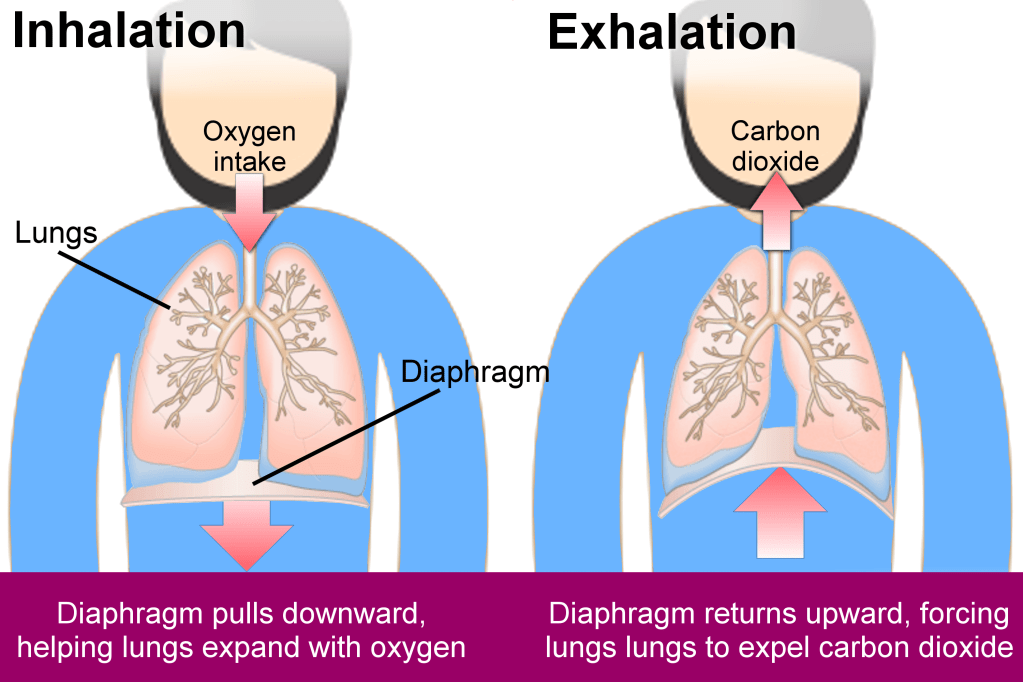
There are 2 sets of muscles we use to EXPAND our lungs, the DIAPHRAGM at the bottom of the chest, and the chest muscles themselves, the INTERCOSTALS. We refer to diaphragmatic breathing as “stomach” breathing, because the stomach bulges out as the descending diaphragm compresses the abdominal contents.
We refer to intercostal breathing as “chest” breathing because the chest expands when the inspiratory intercostals contract.
Diaphragmatic breathing is more efficient, and we encourage our asthmatic patients to Use their more efficient diaphragm to prevent them from tiring as they struggle to get their air out through their narrated airways.
You can squeeze a little extra air out of your lungs by contracting your abdominal muscles.
So to take a DEEP BREATH, see that your stomach rises and your chest expands with the breath IN, and that you squeeze both your abdomen and your chest with the breath out.
Your AIR SACS expand, your lungs are flushed with fresh air, and you blood oxygen, and BRAIN OXYGEN INCREASES with a deep breath in. The “stale air” is cleared by a full breath out.
When you are quietly breathing, letting that vital process take place automatically, notice that a deep breath, or “sigh”, occurs about once every 2 minutes. This is nature’s way to help lung surfactant PREVENT LUNG COLLAPSE and PNEUMONIA.
It is HEALTHFUL to PAY ATTENTION to your BREATHING occasionally! If uninclined to breathe deeply yourself, take a brisk walk up a hill, and let Nature do it for you.