
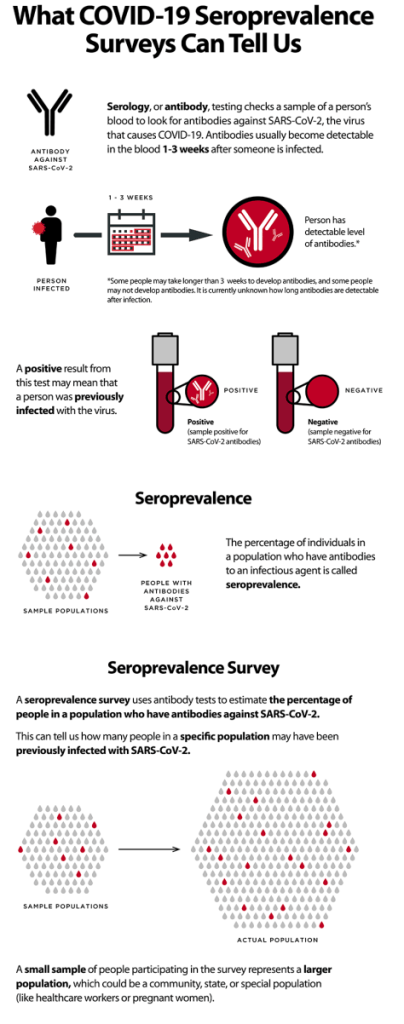
INFOGRAPHIC: “COVID-19 ANTIBODY TESTING” (CDC)


BLOOD VESSELS; it is hard to overestimate their importance. They are literally our lifelines, delivering the oxygen and nutrition necessary for life. We are as old as our blood vessels.
I will divide blood vessels into 4 components with rather separate domains: The Systemic Arterial system, the Pulmonary circulation, the Venous system, and the Lymphatic system, and will discuss these separately.
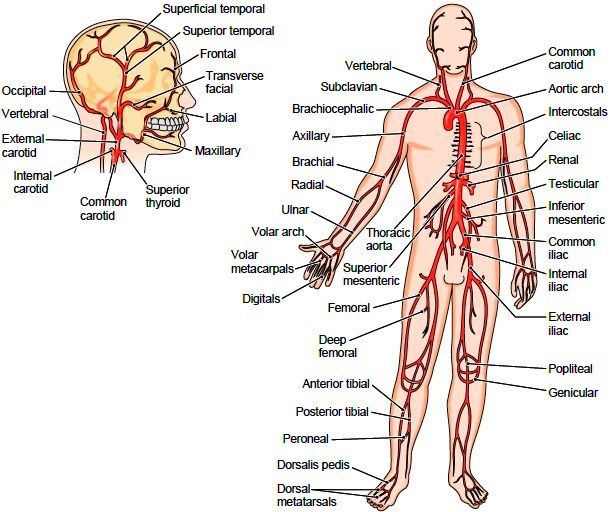
SYSTEMIC ARTERIAL SYSTEM
The Boy Scouts taught me the pressure points; The radial, at the thumb-side of the wrist, the brachial, on the inside of the upper arm, and the inguinal in the groin area. Pressure on these sites will stop arterial bleeding distally.
You should be able to locate the radial artery pulse, and begin to appreciate its strength and regularity. Strength in case you encounter a person who isn’t moving, and regularity for yourself; many older people develop an irregularity called Atrial Fibrillation, and you might be the first to discover it..
ANEURISMS are swelling of the arteries, and the swelling may thin the arterial wall so that it can burst. A Cerebral aneurysm can burst and cause a stroke-like problem. If an aortic aneurism bursts, the internal blood loss can be fatal.
RAYNAUD’S Phenomenon is fairly common, and consists of an over-reaction to cold, where arteries of the hands constrict, and the fingers get white and cold. Burger’s disease involves small arteries, and often is associated with Raynaud’s. The arteries carry the blood distally (away from the heart), continuing to divide into ever smaller arterioles which terminate in capillaries, which branch out in such an arborization as to supply all cells except cartilage and parts of the eye.
HYPERTENSION develops when the arterioles, under hormonal or neural influence, constrict, increasing the resistance to blood flow, and so the pressure. Increase in sodium retention and therefore the blood volume can also increase pressure.
ATHEROSCLEROSIS is the common disease of western life style. Excessive calories and sedentary life style combined with genetic defects in fatty metabolism produce cholesterol plaques which narrow and stiffen the arteries, often leading to BLOCKAGE of blood flow. Blockage of flow to the HEART, BRAIN, KIDNEYS, BOWEL, or EXTREMITIES each produce their separate disorders of Myocardial Infarction, Stroke, Renal artery Disease. Intestinal ischemic syndrome, and Claudication.
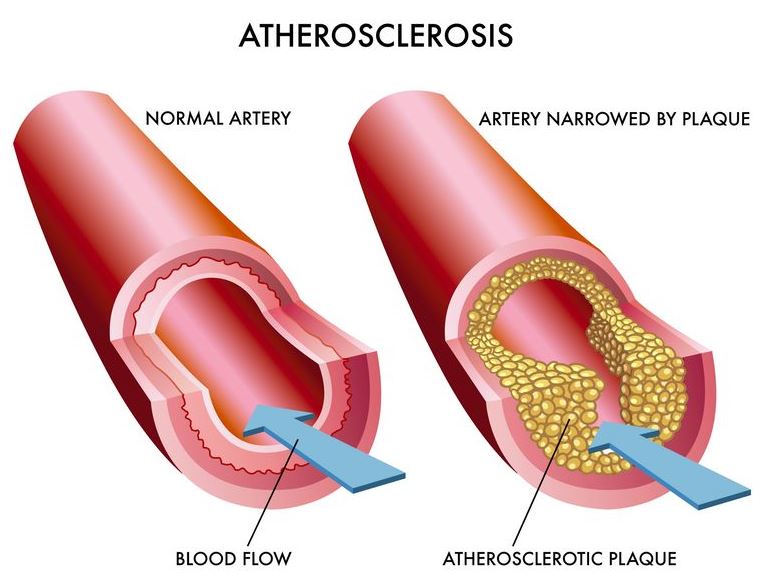
These disorders will each be separately discussed. I have always thought of vascular disease as a special class of CAUSATIVE MECHANISMS when trying to develop a DIFFERENTIAL DIAGNOSIS of a patient’s problems. Blockage to an area results in PAIN or LOSS OF FUNCTION.
Stroke is usually painless with blockage, since the brain has no pain sensors. Blockage of the renal artery often causes complex difficulties including Hypertension, because the kidney is an endocrine organ in addition to its excretory function.
A good Friend and patient showed what careful self-care can accomplish. It all started with a myocardial infarction, the first sign of his blood vessel disease. He had a complication in his workup, and had to have emergency bypass surgery. There had been damage to the heart muscle, with a large reduction in his EJECTION FRACTION.
His cardiologist gave him at most 5 years to live. That was 25 years ago, before the development of the statin drugs. He was given a draconian low cholesterol diet, which he followed exactly. One one visit to the cardiologist, he inquired 
In an orthopedist office for back pain, the orthopedist left the room, and my friend noticed in the CT scan report mention of cysts in the kidneys.
The Orthopedist cared mainly about his bones, and had overlooked the “incidental finding”. His brother had died of mesenteric artery blockage from atherosclerosis, he had stomach symptoms, and sure enough he also had arterial blockage to the intestines.
Bottom line: it pays to be an ACTIVE PARTICIPANT in our medical treatment, and even though we all have genetic determinants, we can make our health BETTER with attention to our health, especially SLEEP, DIET and EXERCISE.
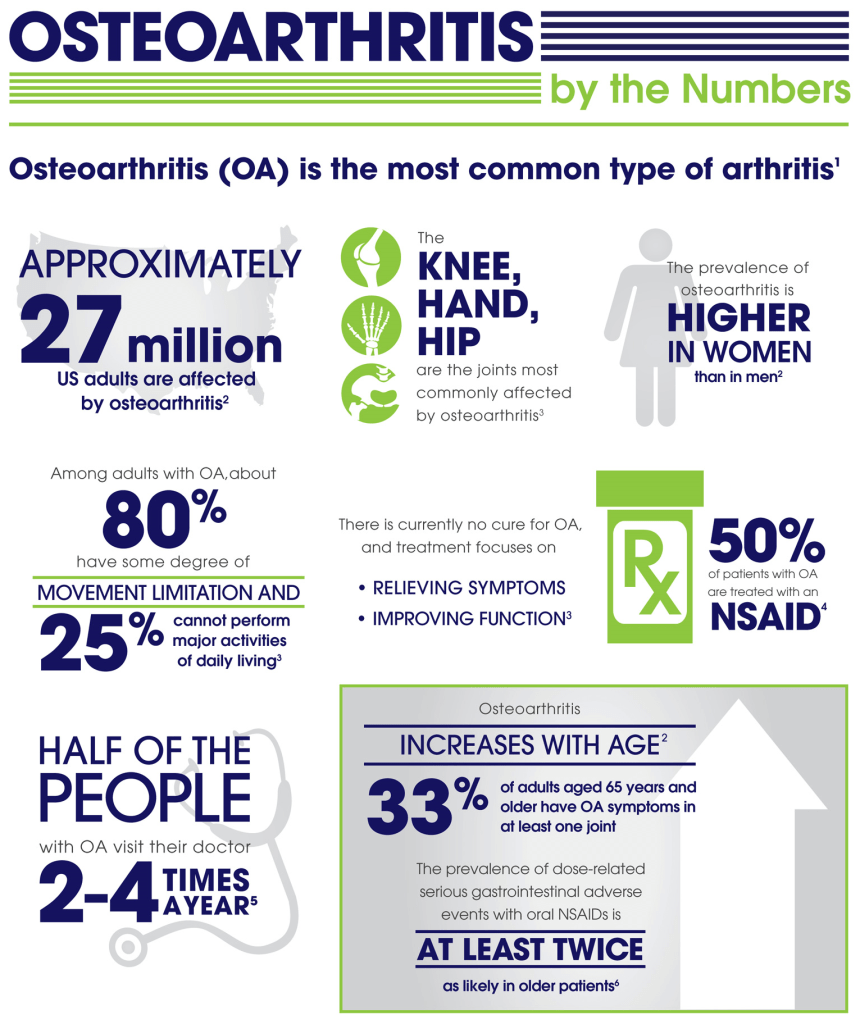
Osteoarthritis (OA) was considered a Degenerative disease when I went to Med School in the late 50s. I am more interested in OA since I have developed it myself.
There is a 40-60% hereditary component. My father’s mother had arthritis badly in her hands, as did my mother’s mother, and so on. A lot of genome-correlation work has shown many different genes involved,
But without a single big contributor, OA appears to be “multifactorial”, similar to a lot of common diseases like Diabetes l. Trauma can be a factor. Old sports injuries, like an ACL tear, that you thought a thing of the past, may come back to haunt you in later years.
INFLAMMATION, the most popular explanatory cause of the decade, may be operating in OA. For instance, you can imagine that OBESITY would contribute to hip and knee OA simply through the traumatic force of gravity. But obesity is also a disease of Inflammation, and increases IL-6 and other cytokines as well.
My own OA involves the classic distal 2 interphalangeal joints (go to the wikipedia manekin for a color-representation of OA classic locations). The base of my thumb, neck and back are also a problem.
Strangely, but wonderfully, my “wheels”, the Hips and Knees, are spared. I have exercised a lot in my life. Clearly, you can’t “wear out” your joints with ordinary exercise.
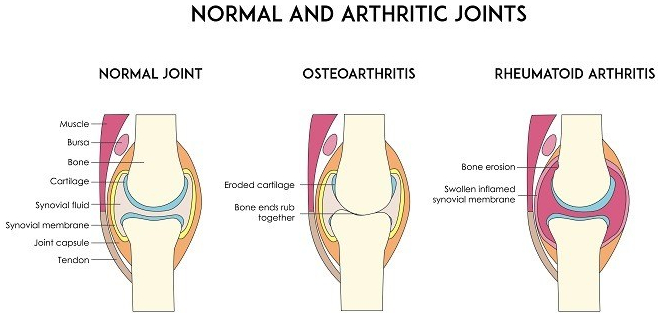
Our joints have evolved to allow us to move. Since bone has a lot of pain fibres, it would be painful to move the joints, directly bone-on-bone. So we have cartilage on the ends of the bones and discs between the vertebrae. The cartilage is slick to reduce friction.
Cartilage has no blood to supply it with nutrients. Instead, it relies on the joint (synovial) fluid. The cartilage is like a sponge. Walking alternately compresses and relaxes the spongy cartilage, increasing the synovial fluid circulation, thus improving the nutrition of the cartilage. If the Cartilage disappears, there is pain.
I am not a fan of pain medication. My belief was strengthened by the side effects of the study of a medication designed to genetically block pain transmission by injection into the painful joints. The side effect was virtual dissolution of the joints in a fraction of those treated. I felt more comfortable with my pain after reading the article.
Although Acetaminophen helps a little, NSAIDs usually work better, perhaps because of their anti-inflammatory action.
If, like me, you have stomach issues, there are the COX-2 inhibitors like Celebrex. The one dose I recently took was almost magical in its effects. Maybe if you don’t use pain Meds much, they work better.
I do take Glucosamine-Chondroitin, thinking that providing building blocks for cartilage couldn’t hurt. Along this line I also EAT CARTILAGE whenever I eat Chicken or ribs, being careful not to damage my teeth in the act of of exercising my jaws.
I also take Curcumin, hoping to relieve some pain, in spite of the fact that it is poorly absorbed (some brave souls take it by injection). I don’t know if any of this helps, How can you know in such a variable disorder, in the absence of controlled studies.
And pain has no OBJECTIVE markers, and is notoriously hard to study. We literally know more about the surface of mars than we know about Pain.
SLEEP, DIET, and EXERCISE, by minimizing OA factors kike OBESITY and INFLAMMATION are the best bet for preventing and treating OA at present.

Chest pain is a common chief complaint. It may be caused by either benign or life-threatening aetiologies and is usually divided into cardiac and non-cardiac causes. James E. Brown, Professor and Chair, Wright State University Boonshoft School of Medicine, Kettering, Ohio, gives us an overview of assessing chest pain in the emergency setting.
COMMENTARY
Dr. James E Brown of the Wright State school Of medicine in Kettering Ohio gave a very interesting discussion of chest pain.
One interesting takeaway is the value of a very experienced clinician dealing with large volumes of emergency room patients. This would make telemedicine with an emergency room hub in a teaching center a very attractive platform.
The consultant doctor in the center has the advantage of his vast experience in rapidly narrowing down the heterogeneous list of different diagnoses that must be considered- the “differential diagnosis”.
Dr. Brown mentioned the “gestalt”, the incorporation of subjective features such as facial and voice cues which add to the objective parameters in patient evaluation. This of course would be amenable to telemedicine although other old-time clinical information like the changes in breath sounds would be more favorable to conventional in-person evaluation.
Ultrasound would More easily be done locally as well.
An interesting take away from this discussion is the value of The patient’s history and past laboratory data, so undervalued by rushed modern doctors. For instance, Electronic medical records (EMR) could provide past history or a previous electrocardiogram for comparison.
Dr. Brown favors the division of chest pain causes into cardiac and non-cardiac. It is easy to develop tunnel vision and look at the patient only as a possible coronary thrombosis. In fact it is better to Rapidly consider the non-cardiac causes that would demand immediate attention while waiting for the results of the Troponin-T test.
For instance pulmonary embolism, aortic dissection, tension pneumothorax, cardiac Tamponade should be considered.
These considerations should be running through the head of the clinician as the IV, EKG, and pulse oximetry are being set up.
In addition to the Troponin-T, bedside ultrasound, and Higher “slice count” CAT machines, and higher “Tesla” MRIs are becoming available major centers which could support small emergency rooms.
If there is One place where “the Flow” would be Appropriate it would be in the mind of the emergency room doctor evaluating acute chest pain.
I have a hard time imagining artificial intelligence endangering her job.
Researchers have run numerous military-style simulations to predict the consequences of fictitious viral outbreaks. We discuss how these simulations work, what recommendations come out of them and if any of these warnings have been heeded.

24:08 One good thing
Our hosts pick out things that have made them smile in the last week, including audience feedback, the official end of the Ebola outbreak in the northeastern Democratic Republic of the Congo, and an enormous t-shirt collection.
News: World’s second-deadliest Ebola outbreak ends in Democratic Republic of the Congo
28:50 The latest coronavirus research papers
Benjamin Thompson takes a look through some of the key coronavirus papers of the last few weeks.
Chronic back pain and sciatica are very common, and increasing in prevalence. The human back does not seem to have been designed for obesity coupled with sedentary habits. I have had both back pain and sciatica . My wife had surgery in an attempt to control her back pain, my son successfully controlled his back pain with medical treatment, and an 87 year old friend recently had successful micro-neurosurgical treatment.
I will summarize these stories and will finish with some generalizations I believe will help those wanting to avoid a lot of misery. The sooner you start the better.
My back pain developed after an ill-advised use of a shovel to get rid of some grass intruding on my asphalt driveway, and caused me to miss work for the only day in 35 years of practice. Sciatica then developed on my left side. I could not sleep flat, and would sit all night in a comfortable chair. A hospital bed helped me outlast the impressive calf pain.
My wife developed severe back pain eventually leading to a “laminectomy and fusion”. Some level of back pain and incapacity plagued her the rest of her life.
My son developed severe sciatica and went to an Orthopedist. After a CAT scan revealed a rupture disc, he was penciled in for surgery. When asking about alternative treatments, the doctor told him, half laughingly, to lose 20% of his body weight and to start swimming. He went on a 30 day, 1000 calorie/day diet and lost 30 lbs. He has been swimming daily for the past 10 years. He has had no more back pain.

My 87 year old friend developed sciatica on his right side, had no luck with PT and pain meds including opioids. Microsurgery by a neurosurgeon successfully removed his ruptured disc, and he has had little or no pain after the first week.
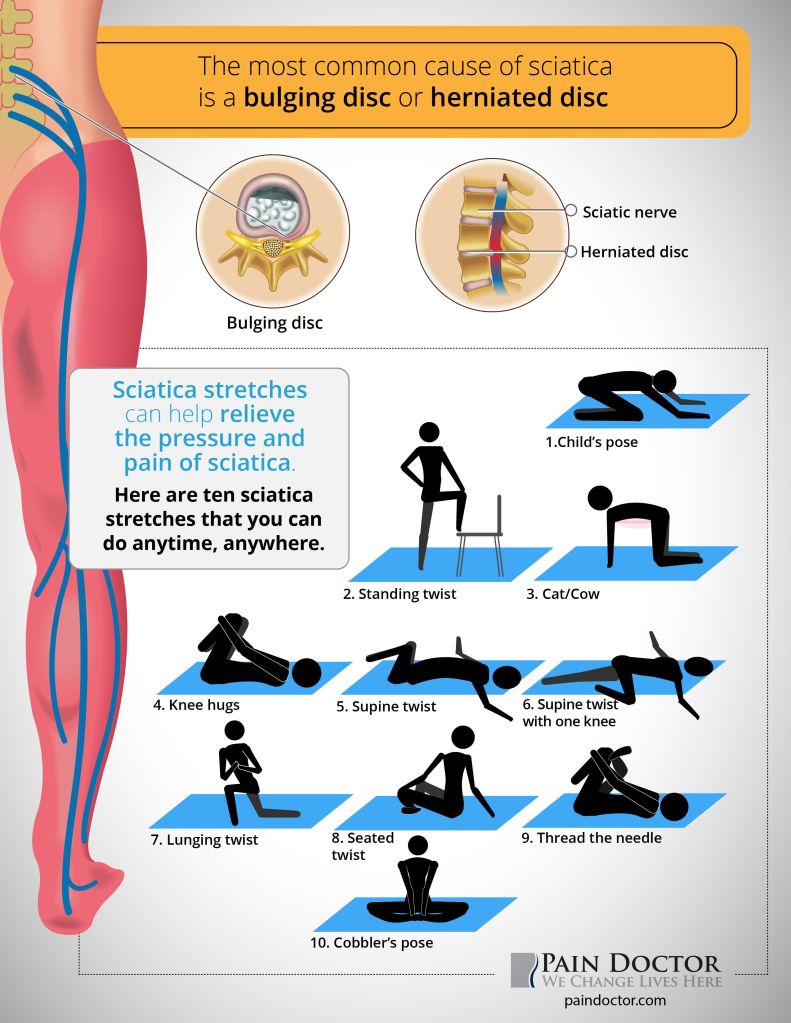
Sciatica at least has a well defined cause: something is irritating that long nerve which starts in the small of the back and travels to its’ destination in the foot. That something is often an extrusion from an intervertebral disc, a cushion between the block-like vertebral bodies.
This herniation can be confirmed by a CAT scan or MRI, and removed by minimally invasive microsurgery. Beyond that model problem, down through spinal stenosis and ending in chronic back pain, the understanding gets progressively more fuzzy, treatment ever more contrived.
Prevention sounds better and better. The most important thing in preventing back pain is to MAINTAIN A NORMAL WEIGHT. Our backs were not designed for vertically compressive forces. The lock-step increasing incidences of obesity and back/sciatic problems support this idea.
REGULAR EXERCISE is very important. Swimming and walking are 2 of the best forms of exercise. Exercises like running on hard surfaces, jumping in volleyball, and weight lifting seem less optimal.
The ABDOMINAL MUSCLES stabilize the spine, and prevent excessive motion. Walking and swimming both exercise and strengthen the abdominals.
Maintaining FLEXIBILITY and RANGE OF MOTION are important. flexibility will help prevent those unplanned, sudden motions from throwing your back out of alignment, or maybe generating a painful muscle tear.
Finally, getting into the habit of BENDING YOUR LEGS and tensing the stabilizing abdominals when you pick up something on the floor is a help.
I question the wisdom of back surgery for back pain alone, especially if accompanied by spinal fusion. Even when there is sciatica, the statistics show that treatment with surgery is no better than medical therapy after 2 years.
The development of microsurgical techniques may give surgery an edge, however. At the risk of cliche, AN OUNCE OF PREVENTION IS WORTH A POUND OF CURE.
One of my nurses who was usually in good health developed chronic complaints. She felt tired all the time and had a variety of aches and pains. She has been going through menopause for a long time but this set of problems seem different. Then she broke her arm after sustaining a minor fall. An investigation was in order. I should order some tests, but which ones?
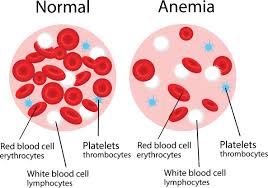
Anemia would explain the fatigue so a CBC was a no brainer. With the surprise fracture, I wanted to cast the net wider, so I ordered a comprehensive metabolic panel.
This is an automated test that was a good value for the amount of information provided, I thought.
Nobody was more surprised than I when the test provided results that were the key to her very rare diagnosis. Her serum CALCIUM was very high, and her alkaline phosphatase was also elevated.
Further evaluation showed her diagnosis to be PRIMARY HYPERPARATHYROIDISM.
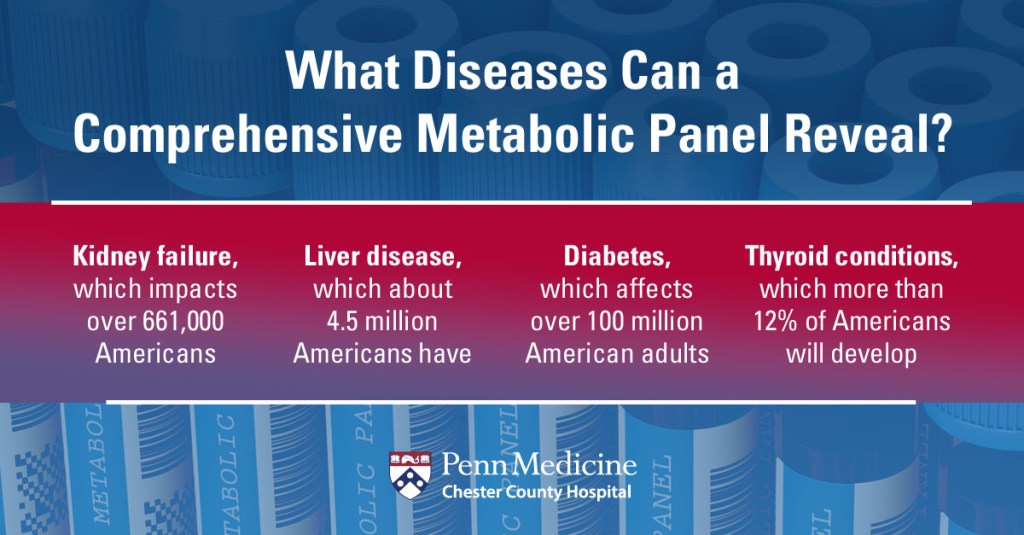
Removal of her abnormal parathyroid gland was curative. I have been a big fan of the Comprehensive Metabolic Panel ever since.
The Panel of 14 tests includes:
Type in “Comprehensive Metabolic Panel” in google, and choose from the variety of “hits” to get more information about this “ Sherlock Holmes’ Magnifying Glass” for Physicians.
Medicine would be hard pressed to do without it!
From ‘Government Technology’ (June 29, 2020):
The hospital system — the first in the country — wired bedside video cameras and microphones on a secure network in 2000 so a medical team could monitor patients at multiple hospitals’ intensive care units from one command center around the clock.
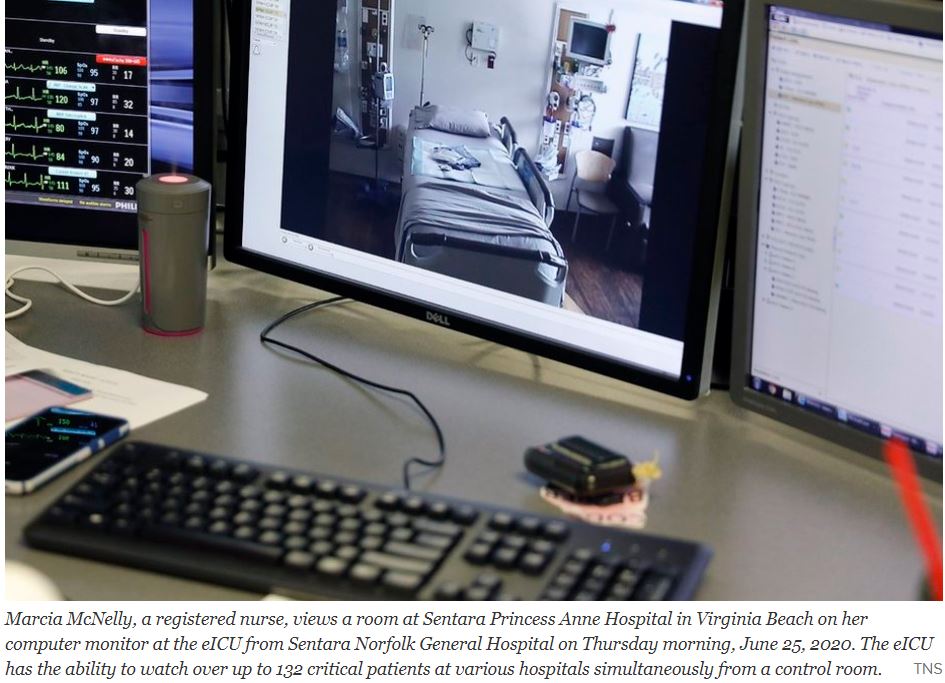
When Sentara Healthcare first launched its “eICU,” the plan was to provide an extra set of eyes on critical patients, especially overnight when staffing was down to a skeleton crew.
Before the coronavirus arrived in Virginia, the average number of telemedicine visits within Sentara Medical Group was about 20 a day. Now, it is more than 2,000 a day, according to the company. Between March and June 21, its clinicians had 314,000 total patient visits, with about 51 percent of them happening virtually.
COMMENTARY
Telemedicine has been slowly developing for 10 or 20 years. The models have been developing according to the requirements of their local areas.
Dartmouth deals with a rural area and has sophisticated aid to it’s associated hospitals and transportation systems to bring Stabilized patients to the main hospital.
Sentara deals with a more urban area and has a central brain aiding the peripheral hospitals in the delivery of treatment locally.
The Tele intensive care unit system of Santara features a central ” Mission Control” With patients in multiple peripheral Intensive care units connected by telemetry. This efficient system allows the peripheral ICUs to operate at a higher level with less staff.
Such telemetry could allow convalescent hospitals and even nursing homes to improve medical care.
With such excellent models one can hope that American medicine will rapidly improve in the post Covid era, riding the wave of telehealth advances.








