COVID 19 is a nasty disease, in case you hadn’t noticed. It is SNEAKY: you can catch it from a person who has no symptoms.
It is UNPREDICTABLE: you may develop no symptoms or Die from it. It can affect any part of your body, including HEART and BRAIN.
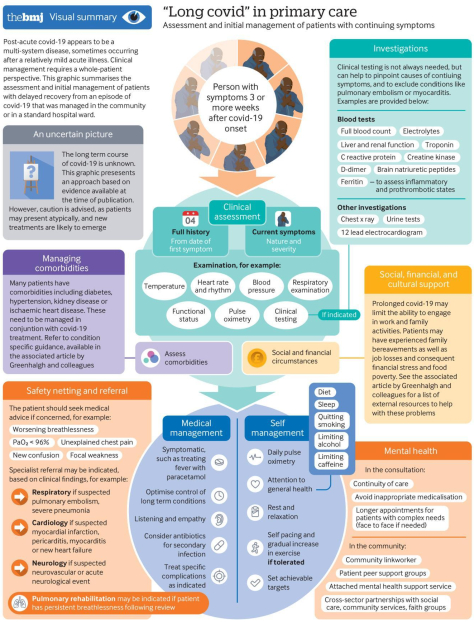
And now we hear that it can DRAG ON. The outstanding infographic, “a multi-systems disease, which is intended for PRIMARY CARE PROVIDERS, has a lot to offer patients, who can do a lot to Care for themselves:
–They can get a THERMOMETER and a PULSE OXIMETER to watch their own temperatures and oxygen saturations
–They can monitor their own COMORBIDITIES, like Diabetes and HYPERTENSION, which are common with severe Covid. In patients who get very ill .
–They can watch their GENERAL HEALTH, including SLEEP and DIET (the exercise part is relegated to DOCTORS recommendations).
You should also RESTRICT Alcohol, Caffeine and it goes without saying CIGARETTE SMOKING. Of course PREVENTION, with DISTANCING, MASKING and being Outside, coupled with SLEEP, DIET and EXERCISE is always best.
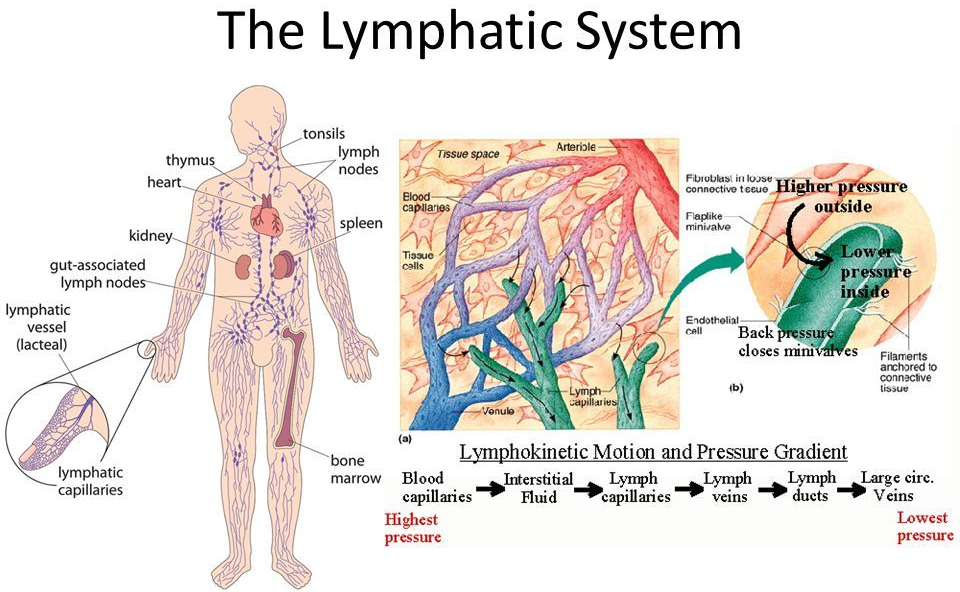
The pulmonary circuit oxygenates and the systemic arterial circuit circulates several Liters of blood per minute. As this blood trickles through the capillaries, some of it oozes out through the thin endothelial lining, becoming interstitial fluid.
Most of this flud gets back into the capillaries and returns to the heart in the venous return. About 20% of the fluid drains into the LYMPHATIC SYSTEM, through the Lymph nodes, and back into the thoracic duct, into the vena cava, and eventually back into the general blood supply, which recirculates.
The Lymphatic System
The Return of the residual interstitial fluid by the Lymphatic vessels back to the general circulation is important, and if BLOCKED by such things as surgery and parasites, produces a swelling known as LYMPHEDEMA.
But the major importance of the lymphatic vessels is their characteristic cells, LYMPHOCYTES, and their accessory structures, The THYMUS, SPLEEN, LYMPH NODES, AND LYMPHATIC TISSUES is in the development and training of the IMMUNE SYSTEM. The THYMUS can be regarded as an organ to TRAIN Lymphocytes to be functional members of the immune system.
SomeT-cells operate to Help B-cells to produce antibody. These are called Th-4 cells. Others, called Th-8 cells. function to delete cells,
The thymus POSITIVELY selects cells that are prepared to recognize pathogens, and gets rid of cells (NEGATIVELY selects) cells that recognize the body’s own cells.
Failure to do so would result in “horror autotoxicus”, or AUTOIMMUNITY. The Thymus performs most of its functions when we are young.
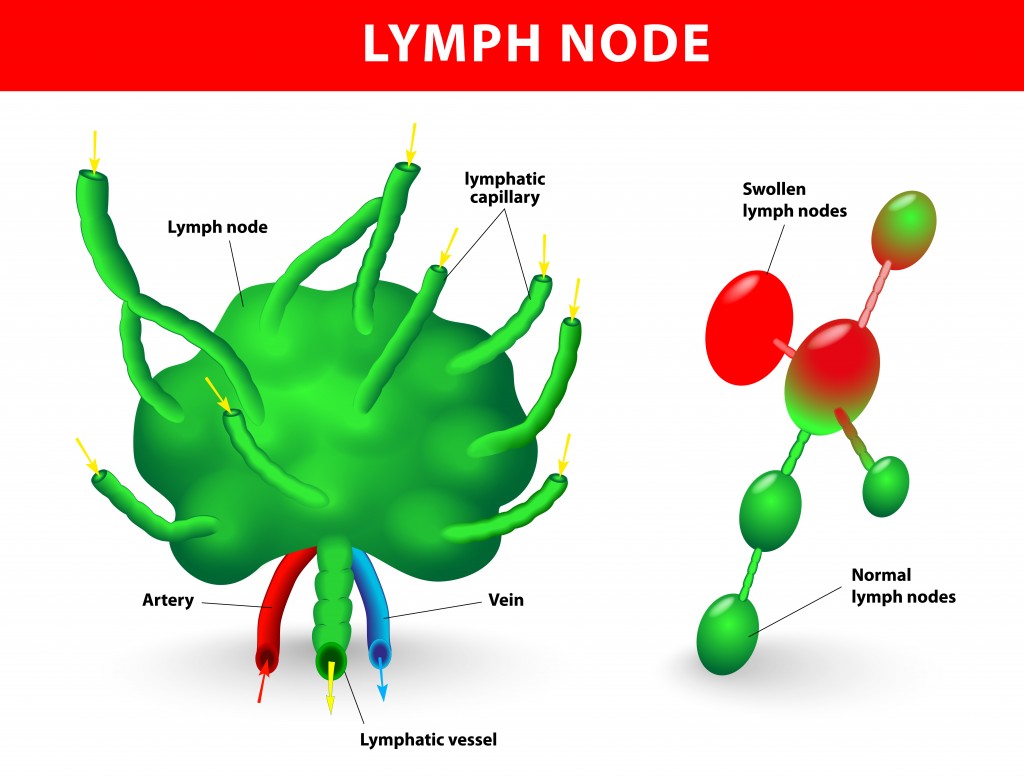
The LYMPH NODES act as a type of filter for the Lymphatic channels, and intercept most bacteria and other pathogens coming through the lymphatic channes to keep them out of the blood stream. Lymph nodes are present at predictable locations throughout the body.
The Spleen acts as a big lymph node to filter the blood directly, and can intercept organisms that have escaped the lymph nodes. The Spleen can enlarge with certain infections, as with the EB Virus that causes mononucleosis.
Rupture of the spleen is not uncommon with direct blunt trauma to the abdomen. Removal of the spleen can increase susceptibility to blood stream infection. Lymph tissue is scattered throughout the body, like in the Tonsils, adenoids and Intestinal tract.
This Lymphocyte-containing tissue can expand with exposure to infection, and can become cancerous with Lymphomas. It can also enlarge enough to produce local Blockage, as with Adenoids. Lymph tissue should not be removed wantonly, since it may provide protection. There are 2 arms of our immune system.
I have been discussing the ADAPTIVE immune system which recognizes the pathogen, and stores memory of this interaction in “memory T-cells”. The helper T-cells( Th-4) start to multiply and stimulate the B-cells to “clonally” proliferate and differentiate into Antibody-producing Plasma Cells. The Cytotoxic T-cells, which can directly kill Pathogens, also multiply.
The first time this happens with a new Pathogen, Like SARS CoV-2, this adaptive process takes a week or so. But if the same Pathogen comes later, The adaptive immune system is ready, via the Memory T-cells, and springs rapidly into action. The 2nd arm of our immune system, shared with all of our vertebrate relatives, is the INNATE immune system.
The innate system is prepared IMMEDIATELY to recognize certain foreign molecules common to many invaders, and foreign our own bodies. It usually does not have the Power of the innate immune system, but in healthy people does an amazingly good job.
Some people just don’t get sick very often. Do the best you can to be one of these healthy people by getting proper SLEEP, DIET. AND EXERCISE!
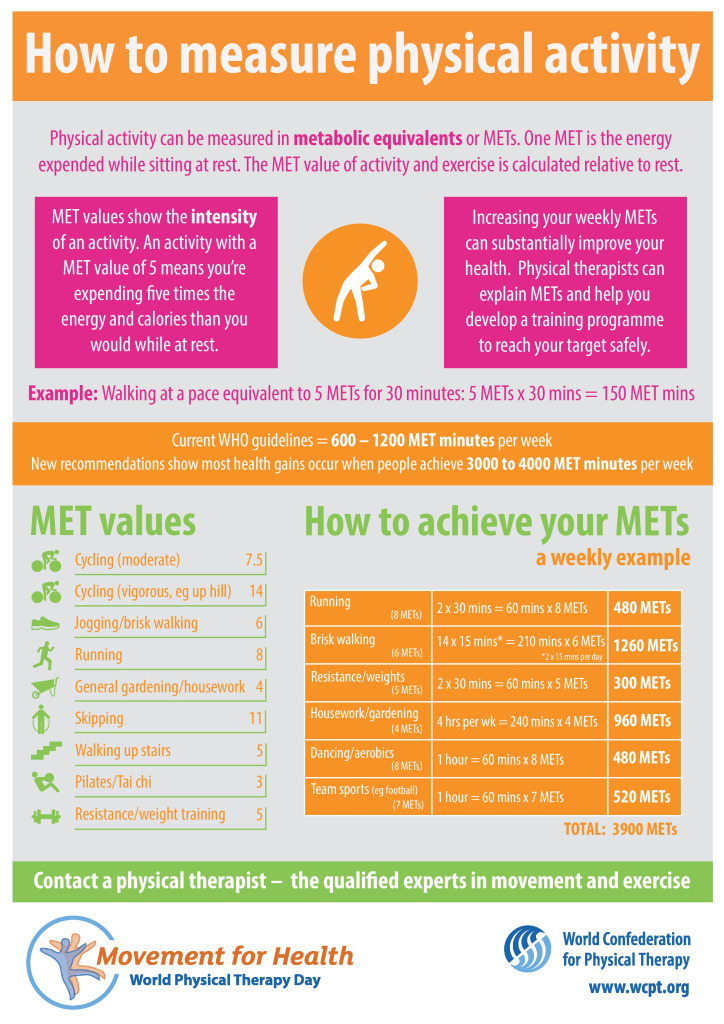
The idea of “METS” as a unit of energy expenditure is interesting and practical. I agree that EXERCISE IS IMPORTANT.
Frank Wilczek, in an article on Dyson Freeman, talked about another unit that I find even more interesting . He proposed that 100 Watts be the unit of energy expenditure. This is (approximately) the energy used in an old 100 Watt incandescent light bulb. It is also the amount of energy used by the “average” human on a 2000 Calorie diet.
Using this unit, the average U.S. Citizen uses 95 units, compared to a 25 unit world average. The suns output is 5 X ten to the fourteenth power, of which 1X ten to the fourth power units lands on earth. Good cocktail information.
I also read that a professional cyclist has an output of only 400 watts, vs. the 14 Mets mentioned in the article.but when I read that the human body is only 20-25% efficient in converting Calories to Watts of Output, 14 Mets made more sense.
By providing house calls and telemedicine from physicians at a fixed monthly fee with no copays, no deductibles, and no insurance required, Heal Pass is making affordable healthcare possible for the estimated 27 million Americans who recently lost their health insurance along with their jobs because of COVID-19.
Heal patients can register now for the new service starting at $49 per month.
Adults can add members of their household to their Heal Pass account for an additional $10 per person each month and may register up to six people to the account.
Patients spend an average of $800 out of pocket each year, in addition to $2,000 for an emergency room visit.
With Heal Pass, a family of four would receive up to 36 total appointments at an average cost of less than $27.
Individual patients can save up to $1,100 per year and the average family can save up to $2,200 per year.
Uninsured individuals and their families are fearful of getting sick and accumulating high medical bills during this time of economic uncertainty.
Heal Pass is not health insurance, but it is health assurance, giving the uninsured the comfort of knowing they can get the care they need at a fixed, low fee with no surprise bills or out of pocket costs.
The new program allows up to eight house calls or telemedicine appointments per member each year in addition to an annual physical, helping with patients’ most common needs, including primary care, preventive care, non-emergency urgent care and chronic disease management.
It also includes free next day delivery of medications prescribed by a Heal doctor. Heal doctors are highly qualified and deliver house calls and care in a way that keeps patients safe from COVID-19 exposure as the country sees a pronounced second spike with 58,618 cases per day on average over the last seven days.
Telemedicine and Covid 19 are fermenting together and creating some new ideas for medical care.
Safety is a concern, and what could be better than your own home, using telemedicine, or a futuristic telemedicine booth located at convenient locations for the busy traveler?
Convenience is another attraction, with a PREPAID aliquot of healthcare; this idea was featured by Forward Health, reviewed a couple of weeks ago, which offered a package of remote monitors and 24/7 access for $149 per month.
Now, Heal pass offers 24/7 access they call “house calls” for $49. a month, with a blizzard of statistics on what you will save. We will see.
You usually get what you pay for.
The Onmed station sounds doable, and has the advantage of self-contained units that may be available to you at the right place and time. You could conceivably even wind up with a prescription as you exit the booth.
Chest pain is a common chief complaint. It may be caused by either benign or life-threatening aetiologies and is usually divided into cardiac and non-cardiac causes. James E. Brown, Professor and Chair, Wright State University Boonshoft School of Medicine, Kettering, Ohio, gives us an overview of assessing chest pain in the emergency setting.
COMMENTARY
Dr. James E Brown of the Wright State school Of medicine in Kettering Ohio gave a very interesting discussion of chest pain.
One interesting takeaway is the value of a very experienced clinician dealing with large volumes of emergency room patients. This would make telemedicine with an emergency room hub in a teaching center a very attractive platform.
The consultant doctor in the center has the advantage of his vast experience in rapidly narrowing down the heterogeneous list of different diagnoses that must be considered- the “differential diagnosis”.
Dr. Brown mentioned the “gestalt”, the incorporation of subjective features such as facial and voice cues which add to the objective parameters in patient evaluation. This of course would be amenable to telemedicine although other old-time clinical information like the changes in breath sounds would be more favorable to conventional in-person evaluation.
Ultrasound would More easily be done locally as well.
An interesting take away from this discussion is the value of The patient’s history and past laboratory data, so undervalued by rushed modern doctors. For instance, Electronic medical records (EMR) could provide past history or a previous electrocardiogram for comparison.
Dr. Brown favors the division of chest pain causes into cardiac and non-cardiac. It is easy to develop tunnel vision and look at the patient only as a possible coronary thrombosis. In fact it is better to Rapidly consider the non-cardiac causes that would demand immediate attention while waiting for the results of the Troponin-T test.
For instance pulmonary embolism, aortic dissection, tension pneumothorax, cardiac Tamponade should be considered.
These considerations should be running through the head of the clinician as the IV, EKG, and pulse oximetry are being set up.
In addition to the Troponin-T, bedside ultrasound, and Higher “slice count” CAT machines, and higher “Tesla” MRIs are becoming available major centers which could support small emergency rooms.
If there is One place where “the Flow” would be Appropriate it would be in the mind of the emergency room doctor evaluating acute chest pain. I have a hard time imagining artificial intelligence endangering her job.
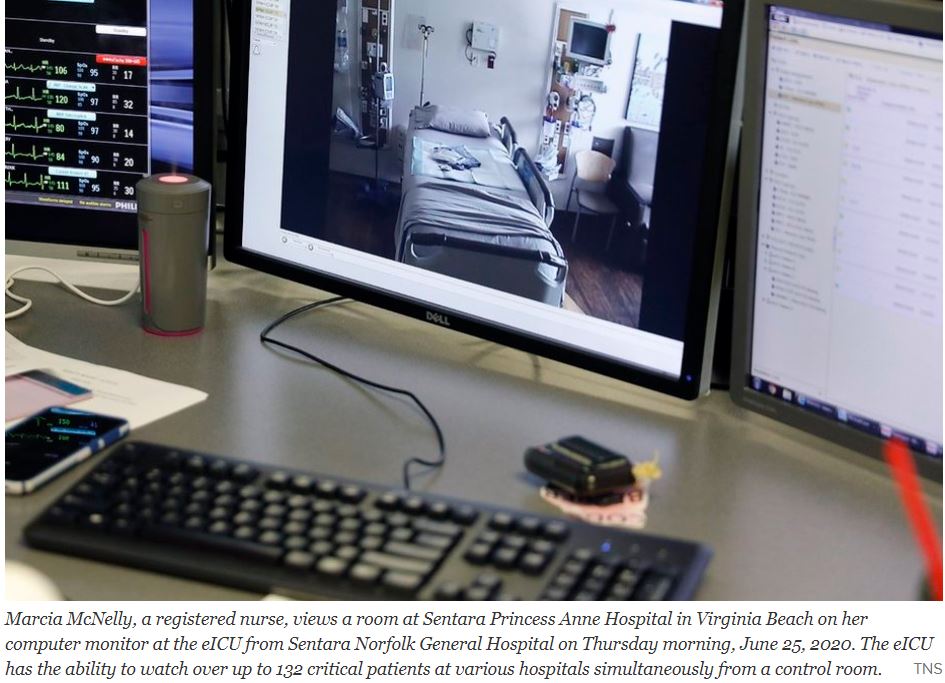
The hospital system — the first in the country — wired bedside video cameras and microphones on a secure network in 2000 so a medical team could monitor patients at multiple hospitals’ intensive care units from one command center around the clock.
When Sentara Healthcare first launched its “eICU,” the plan was to provide an extra set of eyes on critical patients, especially overnight when staffing was down to a skeleton crew.
Before the coronavirus arrived in Virginia, the average number of telemedicine visits within Sentara Medical Group was about 20 a day. Now, it is more than 2,000 a day, according to the company. Between March and June 21, its clinicians had 314,000 total patient visits, with about 51 percent of them happening virtually.
Telemedicine has been slowly developing for 10 or 20 years. The models have been developing according to the requirements of their local areas.
Dartmouth deals with a rural area and has sophisticated aid to it’s associated hospitals and transportation systems to bring Stabilized patients to the main hospital.
Sentara deals with a more urban area and has a central brain aiding the peripheral hospitals in the delivery of treatment locally.
The Tele intensive care unit system of Santara features a central ” Mission Control” With patients in multiple peripheral Intensive care units connected by telemetry. This efficient system allows the peripheral ICUs to operate at a higher level with less staff.
Such telemetry could allow convalescent hospitals and even nursing homes to improve medical care.
With such excellent models one can hope that American medicine will rapidly improve in the post Covid era, riding the wave of telehealth advances.
On the 100th anniversary of the Band-Aid, Tufts engineer Sameer Sonkusale is working to make “smart” bandages.
COMMENTARY
The Tuft’s video talks about transforming the Band-Aid into a detector that can warn of infection, or even exude the proper antibiotic. This would certainly be Applicable to Convalescent homes where people can’t monitor their own healing.
I am Looking forward to the time when the bandage will provide a matrix for the body’s regenerative cells to spread out and cover the wound more rapidly. Possibly someday the regenerative cells themselves can be applied.
—Dr. C.
Empowering Patients Through Education And Telemedicine