From 2019 to 2020, there was a substantial increase in the proportion of older adults who reported that their health care providers offered telehealth visits. In May 2019, 14% of older adults said that their health care providers offered telehealth visits, compared to 62% in June 2020.
Similarly, the percentage of older adults who had ever participated in a telehealth visit rose sharply from 4% in May 2019 to 30% in June 2020. Of those surveyed in 2020, 6% reported having a telehealth visit prior to March 2020, while 26% reported having a telehealth visit in the period from March to June 2020.
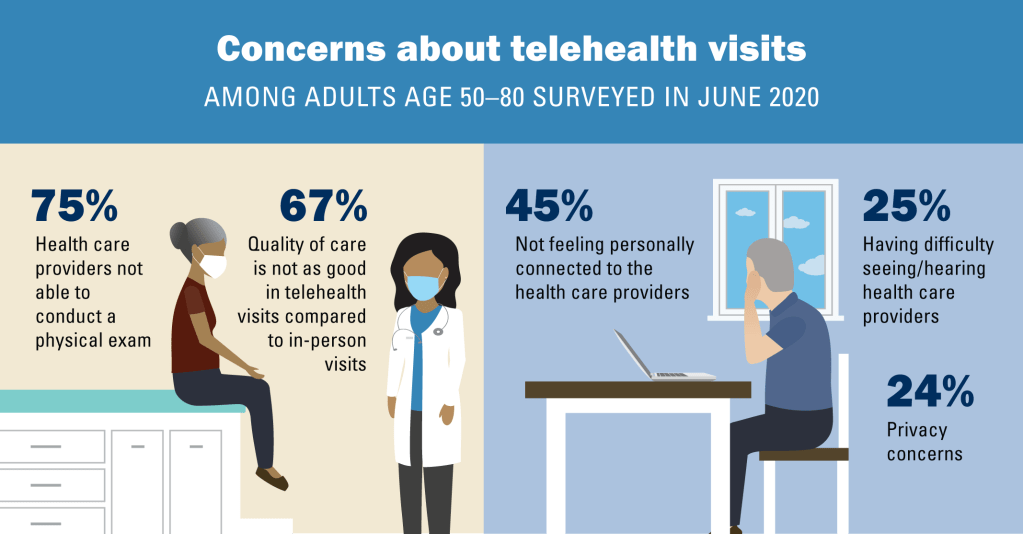
Over the past year, some concerns about telehealth visits decreased among adults age 50–80 whether or not they had a telehealth visit. Older adults’ concerns about privacy in telehealth visits decreased from 49% in May 2019 to 24% in June 2020, and concerns about having difficulty seeing or hearing health care providers in telehealth visits decreased from 39% in May 2019 to 25% in June 2020. Concerns about not feeling personally connected to the health care provider decreased slightly (49% to 45%).
JAMA NETWORK (AUG 5, 2020): 2020 American Diabetes Association (ADA) guidelines recommend that after a trial of metformin, doctors add additional drugs based on the presence of cardiovascular and kidney-related comorbidities, risk of weight gain and hypoglycemia, and cost. In this video, Irl B. Hirsch, MD, of the University of Washington in Seattle, explains the rationale for starting insulin next for patients with persistent HbA1c elevation above 9-9.5% despite lifestyle changes and metformin.
The normal adult heart beats almost as regularly as a metronome, between 60 and 100 beats per minute. I say ALMOST, because when you let your breath out, the VAGUS nerve slows the normal heart slightly.
This is called Sinus Arrhythmia; SINUS because the electrical signal for the heart to contract originates in the usual place, the SINUS NODE.
ARRYTHMIA refers to the irregularity of the beat. Normally, the sinus node originates the electrical impulse, automatically generating the rhythm. The impulse spreads in an organized fashion throughout the Atria causing them to contract and send the collected blood to the ventricles.
The AV node is then activated, and after a slight delay, to allow the ventricles to fill, the impulse spreads to the Ventricles, causing them to contract, The heart is designed to be most efficient above 50 beats per minute, and below about 120. The rate is higher in the young and athletic. Athletes often have an efficient resting pulse in the 40s.
The arrhythmias usually cause the heart to beat too FAST. The most common arrhythmia is ATRIAL FIBRILLATION. In this condition, the upper chambers, the Atria, do not beat in a coordinated manner. The sinus node no longer regularly originates the electrical impulse because the electrical activity is continuously traveling in a disorganized way throughout the upper chambers in a self-propagating manner.
This quivering of the Atria allows the blood to pool in an area called the Atrial Appendages. This stagnant, pooled blood tends to clot, particularly if there is inflammation already present in the heart from vessel damage, obesity, or simply old age.
These CLOTS may find their way into the systemic circulation, and cause a STROKE. Another symptom of Atrial fibrillation is related to the irregular beats, which creates the sensation of PALPITATIONS, which causes you to be AWARE of your heart beating, and can be disturbing.
ATRIAL FLUTTER, and SUPRAVENTRICULAR TACHYCARDIA are other Arrhythmias. Some conditions cause the heart rate to be too SLOW. SICK SINUS SYNDROME is when the sinus node, the PACEMAKER, becomes more and more disordered, sometimes causing the heart to slow excessively, and produce FAINTING, sometimes producing a rapid heart rate.
Heart block is where the signal from the atria don’t reach the ventricles properly, sometimes not at all. The unsignaled ventricles still beat, but more slowly by an intrinsic, “idioventricular” rhythm.
My own experiences with ATRIAL FIBRILLATION will illustrate the problem and it’s treatment. A RAPID HEART BEAT was my introduction into arrhythmias. The rate was 140, and the EKG showed ATRIAL FLUTTER.
My Doctor gave me some PROPAFENONE to attempt a “chemical conversion” but it didn’t work, and i was given a CARDIOVERSION in the ER. The Arrhythmia returned in the form of ATRIAL FIBRILLATION within a couple of weeks. Back to the ER, and another cardioversion.
I was given propafenone, but that didn’t hold me much longer. A RADIOFREQUENCY ABLATION, where the focal points of aberrant electrical activation were isolated kept me in SINUS RHYTHM for a couple of years.
When the Fibrillation returned, Propafenone worked for a while, after which another Ablation, more propafenone, bood level regulation of propafenone to peak at night ( I invariably started fibrillation at night) and so on. With periodic trips to the ER for Cardioversion, I got by for a Decade.
Finally, when regulating the Propafenone couldn’t hold me in Sinus Rhythm longer than a month, I gave up, let myself go on fibrillating, and started taking ELEQUIS to PREVENT EMBOLI AND STROKE. Back when I first started fibrillating I had 2 main reasons for wanting to return to sinus rhythm..
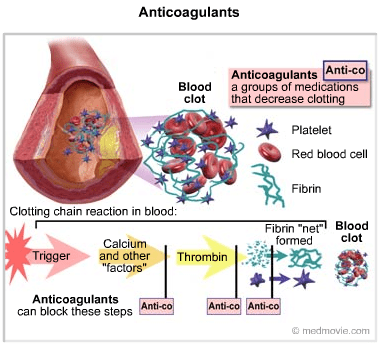
First, I wanted to avoid ANTICOAGULANTS, which initially meant WARFARIN, and regular blood checks. At least, when I finally resigned myself to Fibrillation, Eliquis was available.
The second reason was to avoid medications, including beta blockers,which would be necessary to keep my heart rate in the acceptable range, 80 or below. By the time I gave up on controlling the AF, my rate was in the 70s, going down into the 50s, even while fibrillating.
This good fortune may have been caused another mild heart aberration I had all along, a Partial BUNDLE BRANCH BLOCK, which slowed down the electrical signals to my ventricles. Sometimes you get lucky, and 2 “wrongs” sometimes DO make a “right”. But don’t count on it.
Keep yourself as healthy as possible. Atrial fibrillation is more common with obesity and heart disease. SLEEP APNEA is also a cause, and should be ruled out if you develop Atrial fibrillation. I had a Sleep study, which showed that I had Sleep Apnea, which will be a story i will tell later.
Headache has been with us since Neolithic times, and has caused enough distress to induce our ancestors to scrape holes in their skulls, perhaps to let out the causative Evil Spirits, or maybe a subdural hematoma.
When I was a practicing Allergist, i was sent many headache patients by other Doctors.This was, presumably, because the referring physician thought that their patients had “sinus” headaches. In fact, free standing headache does not commonly come from the sinuses.
Most headaches thought due to ‘sinuses” are in fact “vascular “ headaches. The theory of vascular headaches is that the average diet contains many chemicals that are active on blood vessels. Tyramine, degraded proteins and caffeine are examples. These chemicals, working on the blood vessels, cause irritation and pain. It follows,then, that avoidance of these chemicals would relieve the vascular headaches.
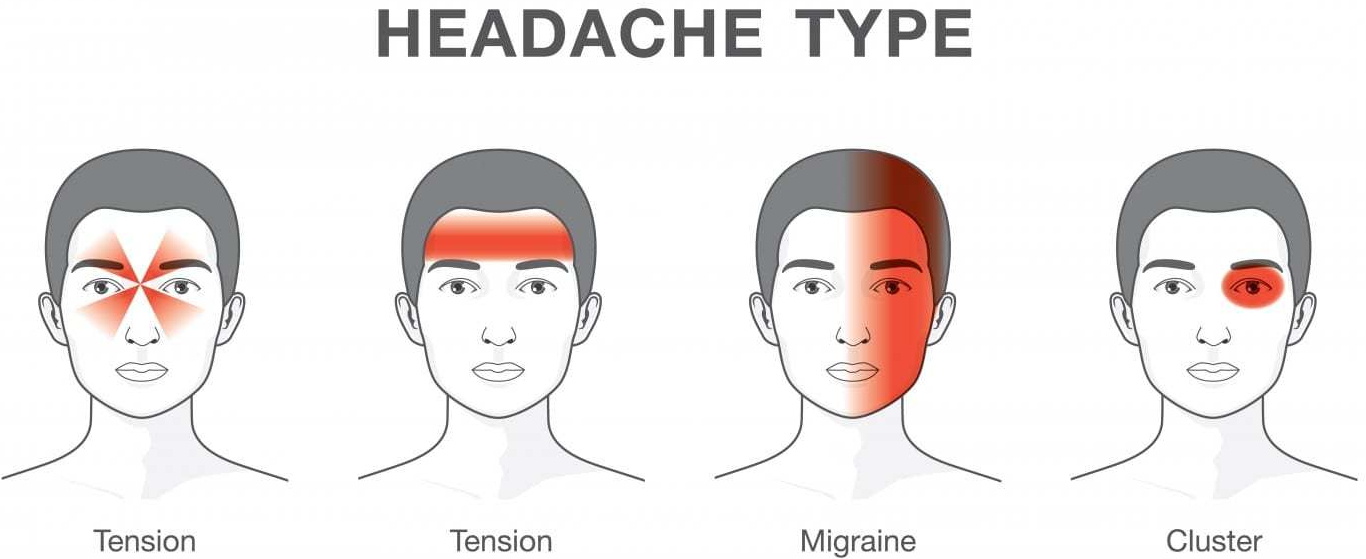
“Vascular headache”, and it’s severe cousin, Migraine headache, is now included under PRIMARY HEADACHE, which also includes Tension headache, and a variety of less common diagnoses. But it is still useful for Treatment, which is why I use the term.
My treatment was a fresh, “health food” diet which avoided preserved foods such as salami, sausages, sauerkraut, leftovers, cheeses, red wine and a variety of other foods likely to have degraded amino acids and Tyramine.
The “mold-free diet” was the published diet closest to listing the suspected foods. The benefit reported from the diet encouraged me to continue recommending it. Vascular headaches are essentially a mild variety of migraine headaches. The foods avoided in the “mold-free diet” are still, after several decades of progress still recognized as migraine triggers.
I encountered only one patient with BRAIN TUMOR in my practice. She had severe, unremitting, gradually increasing headaches over a 4 week period. I called a Neurologist, the type of doctor that treats most severe headaches, who informed me he had NEVER seen a patient with a brain tumor who presented with a headache only, so uncommon it is.
Tension Headaches are milder, and usually can be handled at home. These headaches are usually accompanied by tenderness in the muscles of the back of the neck, or in the temple region, and are brought on by stress.
Hypertension, if extremely high, can cause headache, and can be dangerous, but I never saw a case. Nor did I attend a patient with temporal arteritis, which can also be an emergency.
There are some “red flags” that indicate urgent need for evaluation:
New headache in older patient
New change in headache pattern, or progressively worsening headache
Signs and symptoms of illness ( fever, stiff neck, rash).
Headache triggered by cough or exertion.
Headache in pregnancy or postpartum period
First, worst Headache.
New headaches with AIDS, compromised immunity, or cancer.
Headaches accompanied by mental changes, weakness, or abnormal Neurological signs.
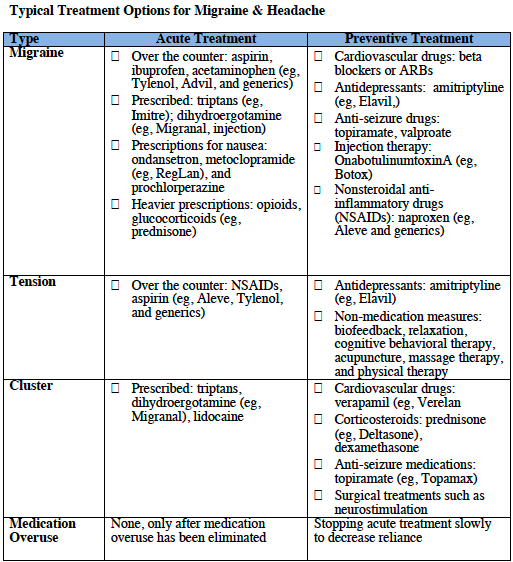
Selective medications are available for some headaches.
Preventative and abortive medications sometimes are helpful for migraine. Antidepressants, tryptans, beta blockers, and corticosteroids are medications best prescribed by specialists.
The tendency to use pain killers, especially narcotics, must be tempered. Frequent use can create additional problems, like ADDICTION. The CAUSE of the headache must be found, if possible, and specifically treated.
Of course, I did find patients with true SINUS HEADACHE, but the headache was accompanied by fever, tenderness over the sinuses, yellow nasal discharge, and other evidence of SINUSITIS, and went away when the infection was treated.
If you have a lot of headaches, and no “red flags” or “risk factors”, you might try a “mold free diet” for a few weeks. Your Nutrition and health would certainly not suffer. And you might have fewer headaches!
Please read the following article for a more complete discussion of this common and annoying problem.
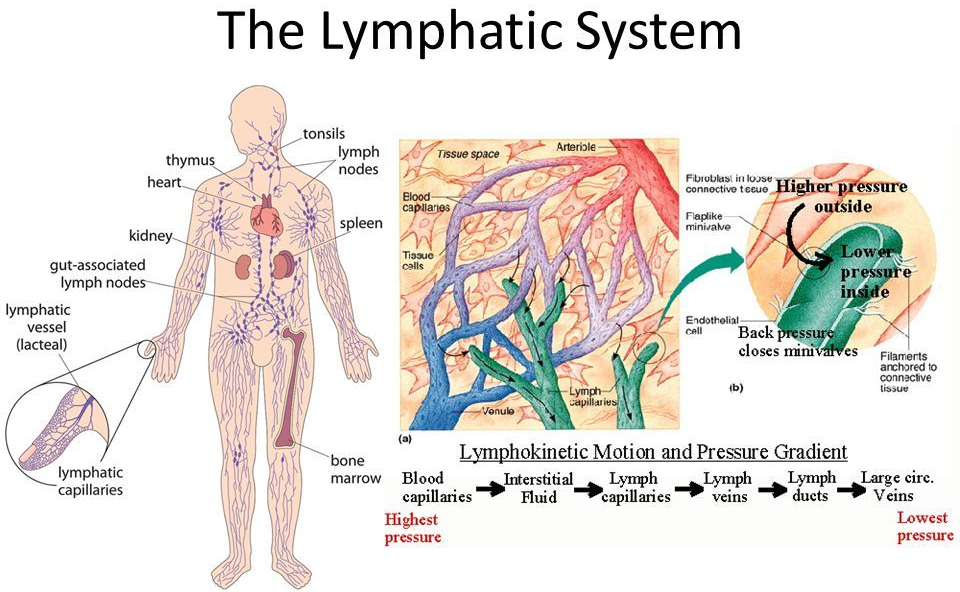
The pulmonary circuit oxygenates and the systemic arterial circuit circulates several Liters of blood per minute. As this blood trickles through the capillaries, some of it oozes out through the thin endothelial lining, becoming interstitial fluid.
Most of this flud gets back into the capillaries and returns to the heart in the venous return. About 20% of the fluid drains into the LYMPHATIC SYSTEM, through the Lymph nodes, and back into the thoracic duct, into the vena cava, and eventually back into the general blood supply, which recirculates.
The Lymphatic System
The Return of the residual interstitial fluid by the Lymphatic vessels back to the general circulation is important, and if BLOCKED by such things as surgery and parasites, produces a swelling known as LYMPHEDEMA.
But the major importance of the lymphatic vessels is their characteristic cells, LYMPHOCYTES, and their accessory structures, The THYMUS, SPLEEN, LYMPH NODES, AND LYMPHATIC TISSUES is in the development and training of the IMMUNE SYSTEM. The THYMUS can be regarded as an organ to TRAIN Lymphocytes to be functional members of the immune system.
SomeT-cells operate to Help B-cells to produce antibody. These are called Th-4 cells. Others, called Th-8 cells. function to delete cells,
The thymus POSITIVELY selects cells that are prepared to recognize pathogens, and gets rid of cells (NEGATIVELY selects) cells that recognize the body’s own cells.
Failure to do so would result in “horror autotoxicus”, or AUTOIMMUNITY. The Thymus performs most of its functions when we are young.
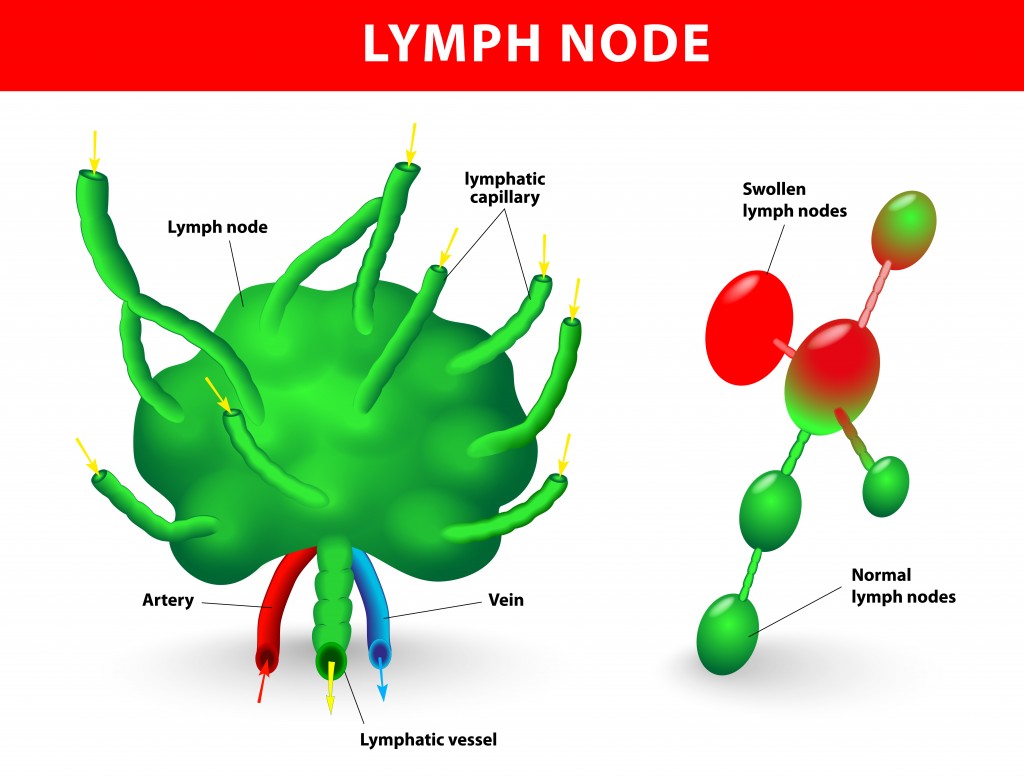
The LYMPH NODES act as a type of filter for the Lymphatic channels, and intercept most bacteria and other pathogens coming through the lymphatic channes to keep them out of the blood stream. Lymph nodes are present at predictable locations throughout the body.
The Spleen acts as a big lymph node to filter the blood directly, and can intercept organisms that have escaped the lymph nodes. The Spleen can enlarge with certain infections, as with the EB Virus that causes mononucleosis.
Rupture of the spleen is not uncommon with direct blunt trauma to the abdomen. Removal of the spleen can increase susceptibility to blood stream infection. Lymph tissue is scattered throughout the body, like in the Tonsils, adenoids and Intestinal tract.
This Lymphocyte-containing tissue can expand with exposure to infection, and can become cancerous with Lymphomas. It can also enlarge enough to produce local Blockage, as with Adenoids. Lymph tissue should not be removed wantonly, since it may provide protection. There are 2 arms of our immune system.
I have been discussing the ADAPTIVE immune system which recognizes the pathogen, and stores memory of this interaction in “memory T-cells”. The helper T-cells( Th-4) start to multiply and stimulate the B-cells to “clonally” proliferate and differentiate into Antibody-producing Plasma Cells. The Cytotoxic T-cells, which can directly kill Pathogens, also multiply.
The first time this happens with a new Pathogen, Like SARS CoV-2, this adaptive process takes a week or so. But if the same Pathogen comes later, The adaptive immune system is ready, via the Memory T-cells, and springs rapidly into action. The 2nd arm of our immune system, shared with all of our vertebrate relatives, is the INNATE immune system.
The innate system is prepared IMMEDIATELY to recognize certain foreign molecules common to many invaders, and foreign our own bodies. It usually does not have the Power of the innate immune system, but in healthy people does an amazingly good job.
Some people just don’t get sick very often. Do the best you can to be one of these healthy people by getting proper SLEEP, DIET. AND EXERCISE!
Technology is finally innovating diabetes management. With the advancement in technologies like continuous glucose monitors, traditional insulin pumps are evolving into smarter devices that can automate insulin delivery.
Medtronic and Tandem Diabetes are the only two companies to offer hybrid closed loop systems. A community of diabetics are also hacking pumps to do the same thing. CNBC’s Erin Black just switched from the hacked system to Tandem’s Control-IQ and takes a look at how insulin pumps are getting smarter.
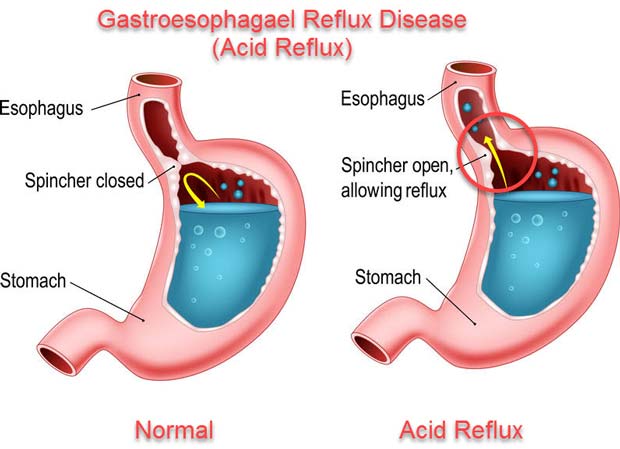
I have been having Heartburn for more than 40 years. The cause of Heartburn is leakage of acid from the stomach, where tissues have evolved to tolerate the highly acidic conditions, into the esophagus, where they haven’t.
The young body has an efficient, functional gate, or sphincter, keeping the food, once swallowed into the stomach, from coming back up. As you eat, you chew your food well to aid digestion. Your taste buds, sensing chemicals in the delicious food, activate saliva.
The salivary enzymes start the digestion of the carbohydrates in the food. If you eat slowly enough, you may be able to appreciate the digestion of tasteless starch, like in bread, into sweet sugar, right in your mouth.
You then swallow the food, which slips past another gate, called the epiglottis, diverting the bolus of food past your windpipe. This gate sometimes does not shut tight, and you choke on the food or drink. The food is then conducted into the highly acidic environment of the stomach.
The stomach evolved to be an acidic, “fiery pit”, inhospitable to any bacteria that came in with the food, thus protecting the stomach from infection. In the old days, there were a lot of bacteria, and the acidity of the stomach was useful, and evolutionarily conserved.
These days, the “fiery pit” tends to be a problem. As you get older, the gate that keeps food in the stomach gets more floppy and relaxed, and allows food to come back up into the esophagus, and sometimes, most often at night when you would rather be sleeping, all the way up to your throat, and is inhaled into your windpipe and lungs in what is called “gastroesophageal reflux”, or GERD.
Even if the food, and acid, doesn’t make it all the way up, and stops at the esophagus, which has not evolved to tolerate acid, you will have “heart burn”. Of course it is not the heart that is burning, but the esophagus, which runs right past the back of the heart as it goes all the way from the throat to the stomach.
When I first developed Heartburn, all that was available was the flavored chalk, Calcium Carbonate, sold as Tums. It works right away, and is a source of Calcium, but can cause trouble, like kidney stones, if you take too much. The relief didn’t last long enough for me, and I had to take more in the middle of the night.
My next medicine was Xantac, a medication that blocks histamine from stimulating acid production in the stomach. The H2 blockers have recently been recalled because of NDMA contamination. I sometimes used H2 blockers like Xantac when my patients would get a bad allergic reaction. In such cases BOTH an H1 blocker like Benadryl, and an H2 blocker are called for.
Zantac was not strong enough for me, and I soon graduated to Prilosec,which directly blocks the secretion of acid in the stomach.
Prilosec was then very expensive, but now is available as the inexpensive GENERIC Medication, Omeprazole. It seems that no medication is without side effects.
Omeprazole, by reducing stomach acid, makes stomach and GI infections more likely, and interferes with the absorption of B12, and Calcium.
If you have had a lot of heartburn over a long period of time, you should check with a Gastroenterologist, who may scope you to rule out Barritt’s esophagus, which can lead to Cancer.
It is interesting that the antacid Tums in excess can cause too MUCH Calcium in the body, and can cause kidney stones and other kidney problems like MAS, and Omeprazole, by interfering with absorption can cause too LITTLE absorption of Calcium, leading to OSTEOPOROSIS.
The best rule is to take as low a dose of ANY medication as possible, preferably none, to understand the possible side effects, and compensate for them if you can.
–Dr. C
Empowering Patients Through Education And Telemedicine