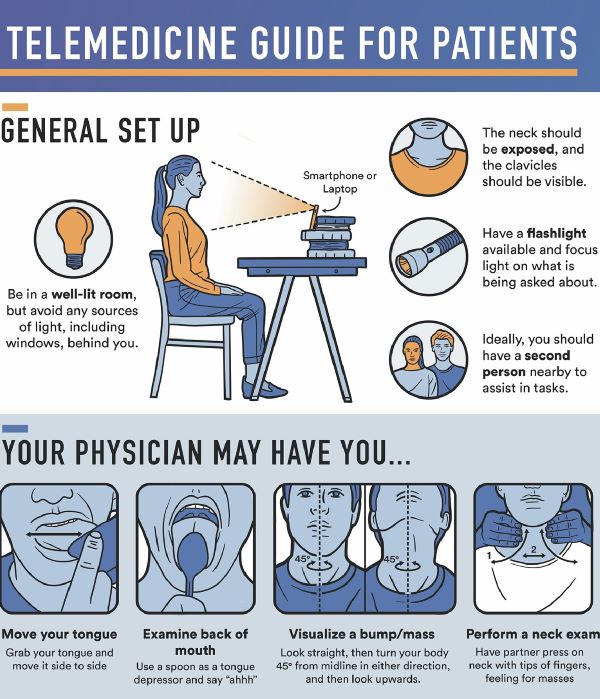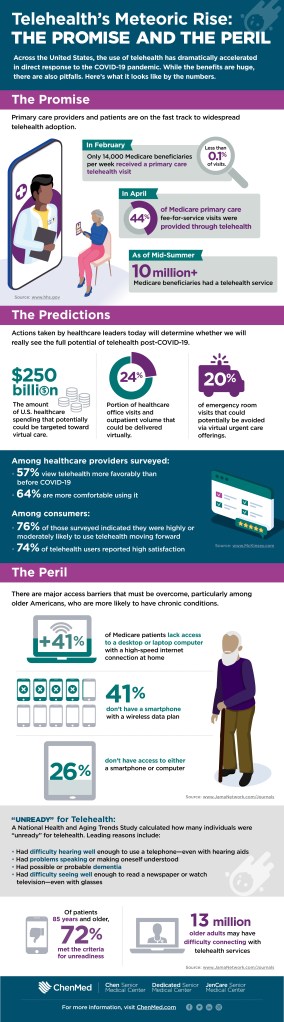
Infographic: ‘The Promise & Concerns Of Telehealth With Medicare Patients’

Diabetologia (Sept 8, 2020) – Insomnia with objective short sleep duration has been associated with an increased risk of type 2 diabetes in observational studies [27, 28]. The present MR study found strong and suggestive evidence of a causal association of insomnia and short sleep duration, respectively, with increased risk of type 2 diabetes.


The present study verified several previously reported risk factors and identified novel potential risk factors for type 2 diabetes. Prevention strategies for type 2 diabetes should be considered from multiple perspectives on obesity, mental health, sleep quality, education level, birthweight and smoking.
COMMENTARY
This was a laborious and apparently objective study.
The discovery of insomnia as a unique risk factor is no surprise, and reinforces the restorative IMPORTANCE of SLEEP.
I was surprised to see docosohexanoic and Eicosapentanoic acids in the risk column and LDL in the good column. However they were studying type 2 diabetes, and not vascular health. I will continue to take my fish oil, and enjoy my HDL, which is in the good column.
—Dr. C.
You know you need to get enough sleep, but the question remains: How much is enough? Sleep scientist Matt Walker tells us the recommended amount for adults and explains why it’s necessary for your long-term health. Sleeping with Science, a TED original series, uncovers the facts and secrets behind our nightly slumber. (Made possible with the support of Beautyrest)
Check out more: https://go.ted.com/sleepingwithscience
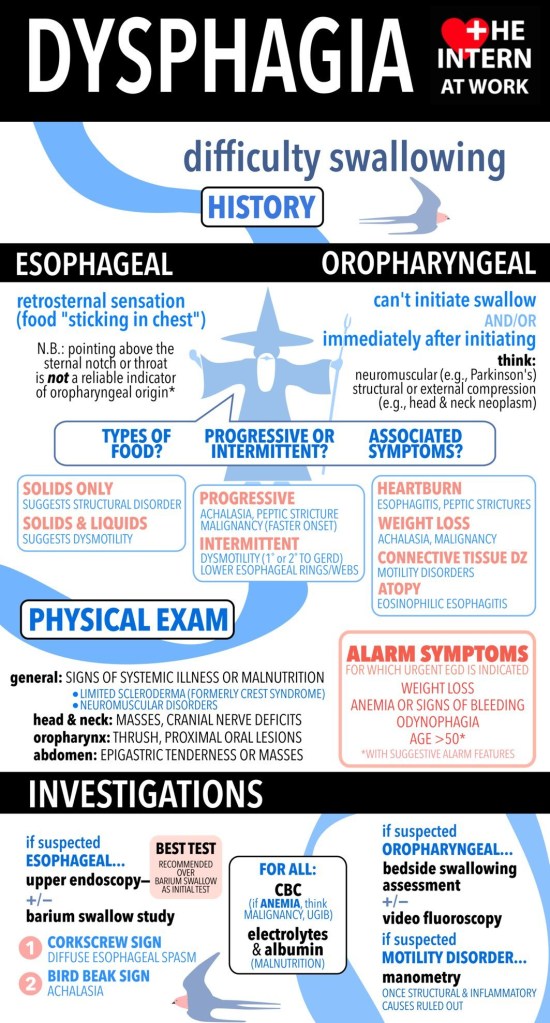
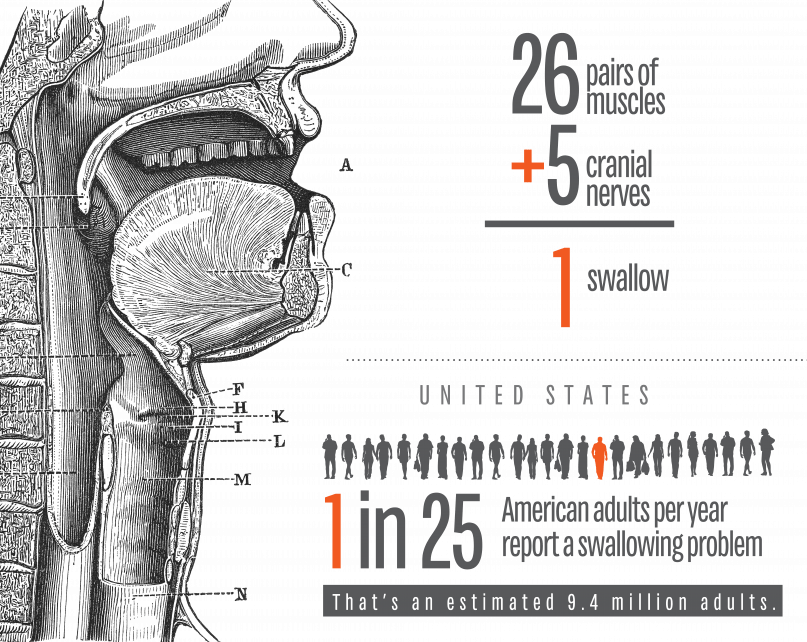
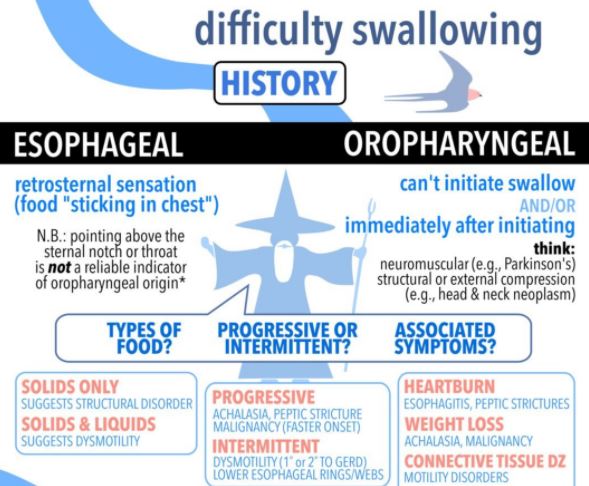
I am defining SWALLOWING TROUBLE as the difficulty in transport of food to the stomach, once clear of the throat. Problems with the initiation of the swallowing process are discussed separately.
PAIN in the mid-chest ON SWALLOWING is a worrisome symptom which can be due to inflammation of the lining of the esophagus from a variety of causes. An esophageal yeast infection, which can also involve the throat (called ‘“thrush”), often warns of immune deficiency and can be a sign of AIDS, or be caused by immune suppressing medication. If persistent, pain on swallowing can be a warning sign of CANCER.
If in the presence of GERD, it can be a sign of chronic inflammation or ulceration. In-coordination of the normally smooth muscular propulsive wave can cause a cramping, muscular pain.
Normal “peristalsis” is so efficient, that food can be swallowed without the help of gravity, when UPSIDE DOWN. I wouldn’t recommend trying this, even to cure hiccoughs. There is a muscular “gate” at the bottom of the esophagus, just as it enters the stomach. This gate is often too relaxed, and allows for the reflux of acid and food from the stomach, or GERD. It can also Fail to open, called achalasia, and hold up the food in its journey to the stomach.
The area can be scarred by repeated acid reflux, and become NARROWED; this is called a STRICTURE, and can cause a blockage in swallowing. One of my Doctor friends had to go to the Emergency room when some Steak got stuck in the esophagus.
The ER Doctor removed the steak with a fiberoptic Scope, and then proceeded to DILATE the stricture with a “bougie”, an instrument of a precisely calibrated size designed to STRETCH the constricted area. This uncomfortable procedure had to be done repeatedly, a caution to those who would wait too long before getting such a problem evaluated and corrected.
EOSINOPHILIC ESOPHAGITIS has been diagnosed with increasing frequency, and can cause Pain in the middle of the chest, trouble swallowing, and even regurgitation of food. This special type of inflammation is more common in allergic patients, and can be caused by certain foods.
So as you can see, swallowing trouble, if persistent, is nothing to fool around with, and should be checked out by a competent doctor. Don’t wait too long.
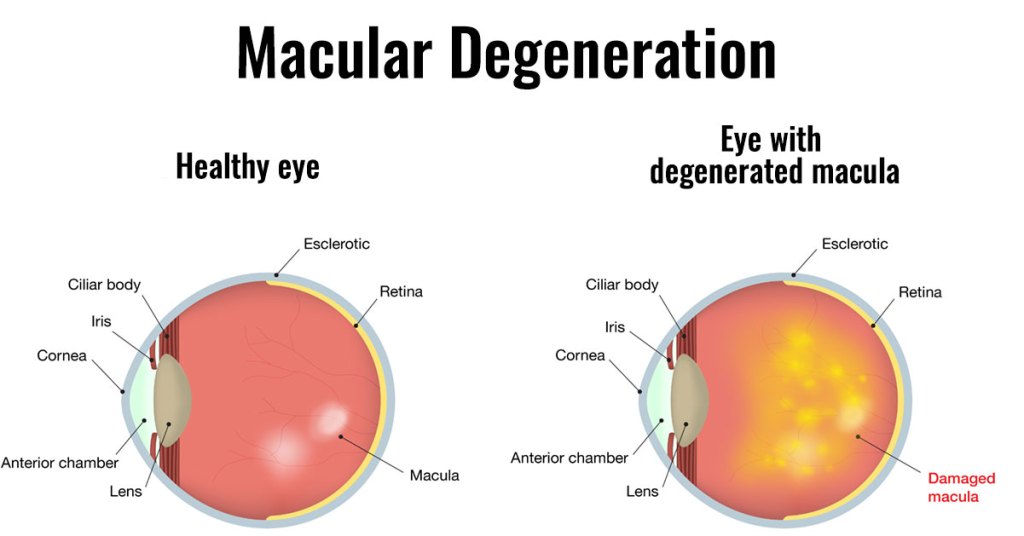
Macular Degeneration is the most common cause of blindness in the western world.as you get older, it becomes increasingly common, and almost 20% of people older than 85 years have this disease.
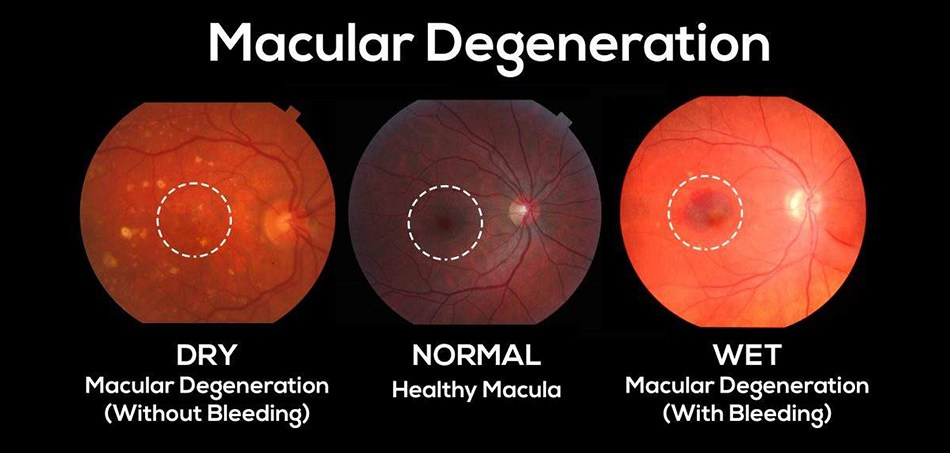
It comes in 2 types, dry and wet. Mostly it starts as the milder dry type, which develops slowly and has no definite treatment. The dry type can develop into the more rapidly progressive wet variety, however, and is important to notice and report to your ophthalmologist.
The MACULA is the center of the visual field, and has by far the most photoreceptors. It yields the sharpest vision, and is essential for reading, and even recognizing faces.
LOSS OF VISION is the commonest symptom, but is hard to notice in a slowly developing condition. A neurologist friend of mine alerted me to the AMSLER GRID, which helps in picking up the subtle distortions of this sneaky problem.
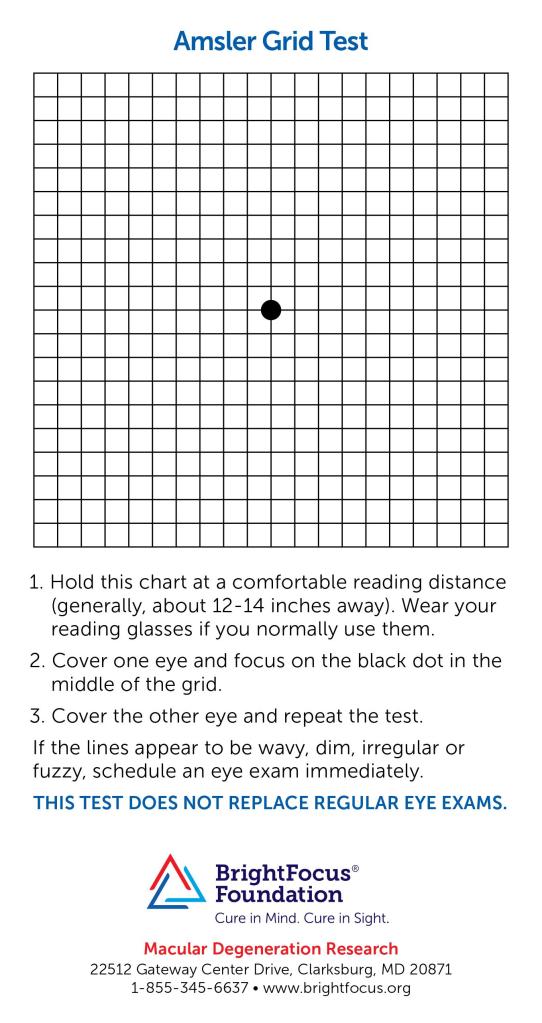
Checking your vision every few days-it takes only a few seconds- is a good idea as you age. You might be healthy in every other way, but if you are blind, the quality of life in your final years will suffer. The mechanics of the wavy lines generated by macular degeneration are deposits beneath the macula, raising it up.
The deposits are fatty in the case of the dry, and fluid in the case of the wet macular degeneration; and fluid from the abnormal blood vessels in the wet MD can collect very rapidly indeed.
Even though the cause of MD is unknown, prevention is by the same old healthy habits tiresomely mentioned in all my other postings: DIET and EXERCISE. I’m sure that good sleep doesn’t hurt either, No cigarette smoking of course, and there are some vitamins and minerals mentioned, such as lutein, zeaxanthin, zinc, and copper.
The wet MD does have a treatment to slow down the disease. Since blood vessel growth is important in causation, antibodies to VEGF, vascular endothelial growth factor, are injected into the macular area. I’m sure that more help is on the way. Some treatments to support the protective pigmented layer of the retina are currently in progress.