As levels of estrogen, a crucial chemical messenger, trend downward, women are at higher risk for severe depressive symptoms. Bone loss accelerates. In women who have a genetic risk for Alzheimer’s disease, the first plaques are thought to form in the brain during this period.

About 85 percent of women experience menopausal symptoms. Rebecca Thurston, a professor of psychiatry at the University of Pittsburgh who studies menopause, believes that, in general, menopausal women have been underserved — an oversight that she considers one of the great blind spots of medicine. “It suggests that we have a high cultural tolerance for women’s suffering,” Thurston says. “It’s not regarded as important.”
Even hormone therapy, the single best option that is available to women, has a history that reflects the medical culture’s challenges in keeping up with science; it also represents a lost opportunity to improve women’s lives.
COMMENTS:
The New York Times, Sunday magazine, posted an article by Susan Dominus entitled “the vicious cycle”, in which was a long discussion of the disease burden of menopause. It is well worth reading.
“Forever Feminine” was a book by Robert Wilson, in 1966, which promoted hormone treatment for “enjoyment of sex” in menopausal women. The use of estrogen skyrocketed.
Alarming research in 1975, which linked estrogen usage to endometrial cancer, halted the rise of the drug’s popularity.
Without hormonal treatment, the many symptoms of menopause were devalued and quietly suffered by women.
The medical profession has been slowly recovering from whiplash. New, better controlled research is being done and slowly a more nuanced approach is being taken. Women with a history of heart attack or stroke are still generally advised against hormonal therapy, but many others are being given birth control pills, which is a combination of estrogen and progesterone.
The average age of menopause is approximately 50 years of age, but symptoms can anticipate menopause by several years. An elevated FSH is the usual laboratory test to indicate perimenopause.
Early menopause can be associated with a decreased lifespan, increased likelihood of osteoporosis, cardiovascular disease and dementia, and is often treated with hormonal therapy. A delayed menopause is less likely to be treated with hormonal therapy, because of increased risk.
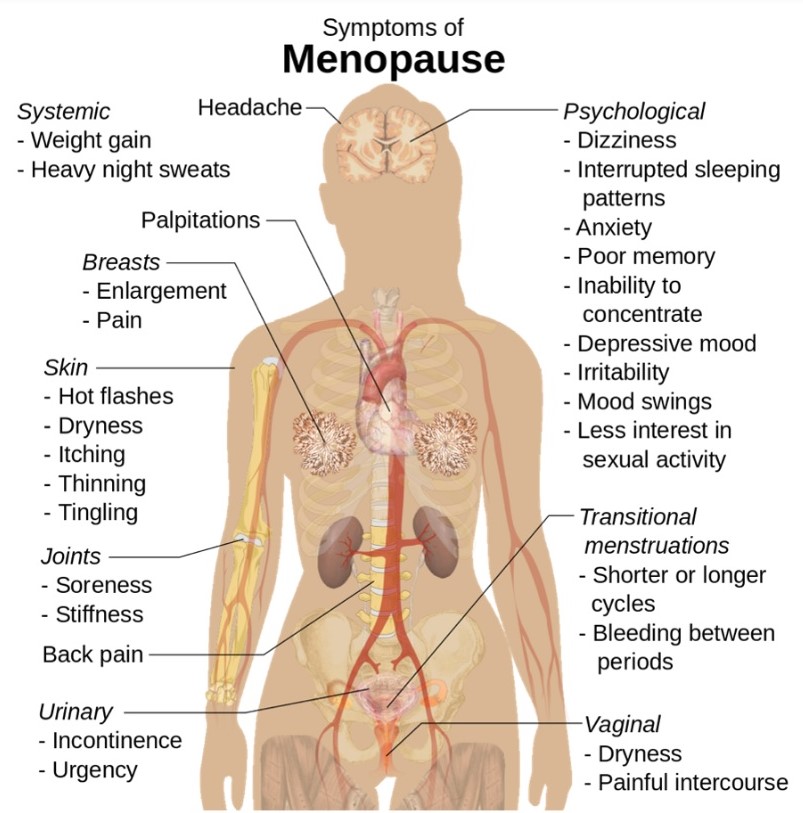
There are a lot of risk factors to be balanced against the symptoms involved, such as hot flashes and the entire panoplay of symptoms indicated in the infographic.
Some day, artificial intelligence will be used in order to make more explicit the benefits and risks involved. Until that time, the patient suffering from premenopausal or menopausal symptoms should find a Doctor Who would actually listen to her, a difficult task these days.
—Dr. C.