Headache has been with us since Neolithic times, and has caused enough distress to induce our ancestors to scrape holes in their skulls, perhaps to let out the causative Evil Spirits, or maybe a subdural hematoma.
When I was a practicing Allergist, i was sent many headache patients by other Doctors.This was, presumably, because the referring physician thought that their patients had “sinus” headaches. In fact, free standing headache does not commonly come from the sinuses.
Most headaches thought due to ‘sinuses” are in fact “vascular “ headaches. The theory of vascular headaches is that the average diet contains many chemicals that are active on blood vessels. Tyramine, degraded proteins and caffeine are examples. These chemicals, working on the blood vessels, cause irritation and pain. It follows,then, that avoidance of these chemicals would relieve the vascular headaches.
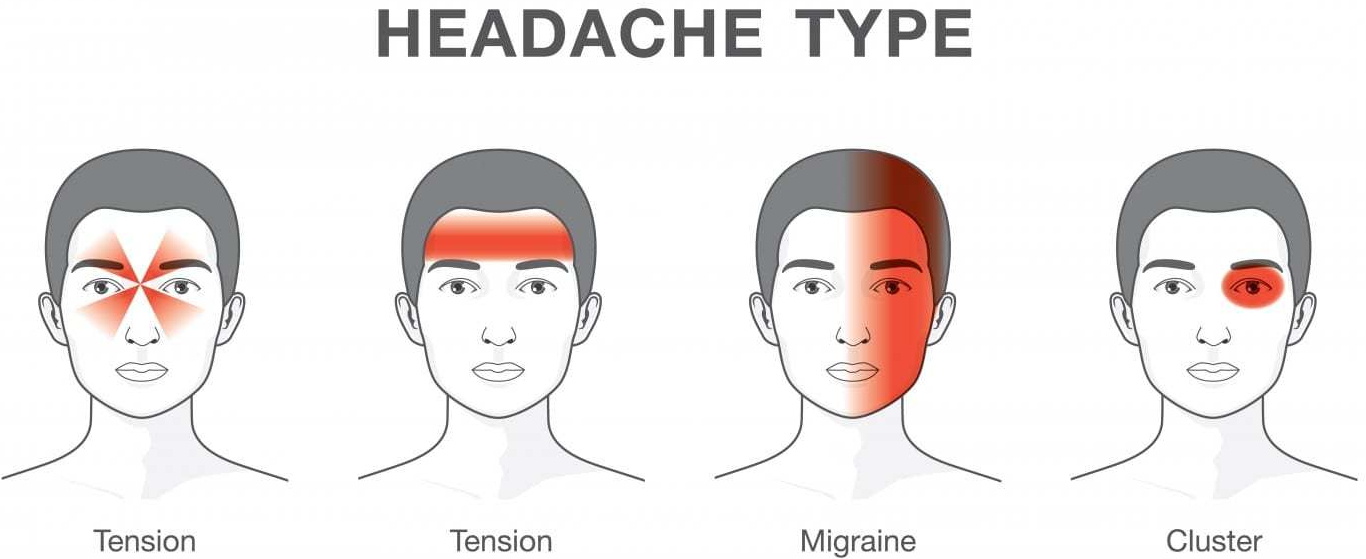
“Vascular headache”, and it’s severe cousin, Migraine headache, is now included under PRIMARY HEADACHE, which also includes Tension headache, and a variety of less common diagnoses. But it is still useful for Treatment, which is why I use the term.
My treatment was a fresh, “health food” diet which avoided preserved foods such as salami, sausages, sauerkraut, leftovers, cheeses, red wine and a variety of other foods likely to have degraded amino acids and Tyramine.
The “mold-free diet” was the published diet closest to listing the suspected foods. The benefit reported from the diet encouraged me to continue recommending it. Vascular headaches are essentially a mild variety of migraine headaches. The foods avoided in the “mold-free diet” are still, after several decades of progress still recognized as migraine triggers.
I encountered only one patient with BRAIN TUMOR in my practice. She had severe, unremitting, gradually increasing headaches over a 4 week period. I called a Neurologist, the type of doctor that treats most severe headaches, who informed me he had NEVER seen a patient with a brain tumor who presented with a headache only, so uncommon it is.
Tension Headaches are milder, and usually can be handled at home. These headaches are usually accompanied by tenderness in the muscles of the back of the neck, or in the temple region, and are brought on by stress.
Hypertension, if extremely high, can cause headache, and can be dangerous, but I never saw a case. Nor did I attend a patient with temporal arteritis, which can also be an emergency.
There are some “red flags” that indicate urgent need for evaluation:
- New headache in older patient
- New change in headache pattern, or progressively worsening headache
- Signs and symptoms of illness ( fever, stiff neck, rash).
- Headache triggered by cough or exertion.
- Headache in pregnancy or postpartum period
- First, worst Headache.
- New headaches with AIDS, compromised immunity, or cancer.
- Headaches accompanied by mental changes, weakness, or abnormal Neurological signs.
Selective medications are available for some headaches.
Preventative and abortive medications sometimes are helpful for migraine. Antidepressants, tryptans, beta blockers, and corticosteroids are medications best prescribed by specialists.
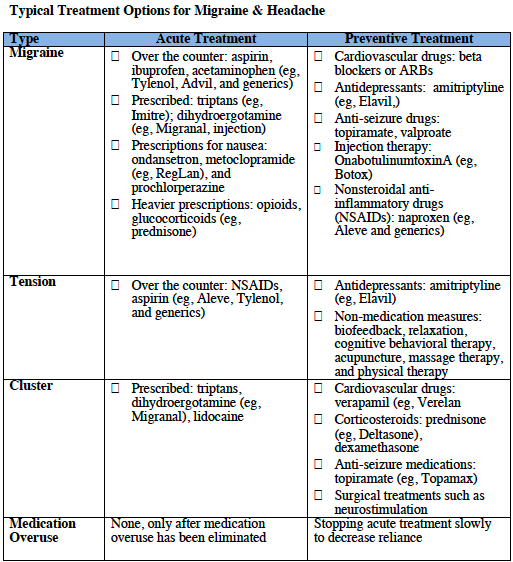
The tendency to use pain killers, especially narcotics, must be tempered. Frequent use can create additional problems, like ADDICTION. The CAUSE of the headache must be found, if possible, and specifically treated.
Of course, I did find patients with true SINUS HEADACHE, but the headache was accompanied by fever, tenderness over the sinuses, yellow nasal discharge, and other evidence of SINUSITIS, and went away when the infection was treated.
If you have a lot of headaches, and no “red flags” or “risk factors”, you might try a “mold free diet” for a few weeks. Your Nutrition and health would certainly not suffer. And you might have fewer headaches!
Please read the following article for a more complete discussion of this common and annoying problem.