NEW ENGLAND JOURNAL OF MEDICINE (JULY 23, 2020): A large body of evidence suggests that consumption of caffeinated coffee, the main source of caffeine intake in adults in the United States, does not increase the risk of cardiovascular diseases and cancers. In fact, consumption of 3 to 5 standard cups of coffee daily has been consistently associated with a reduced risk of several chronic diseases.
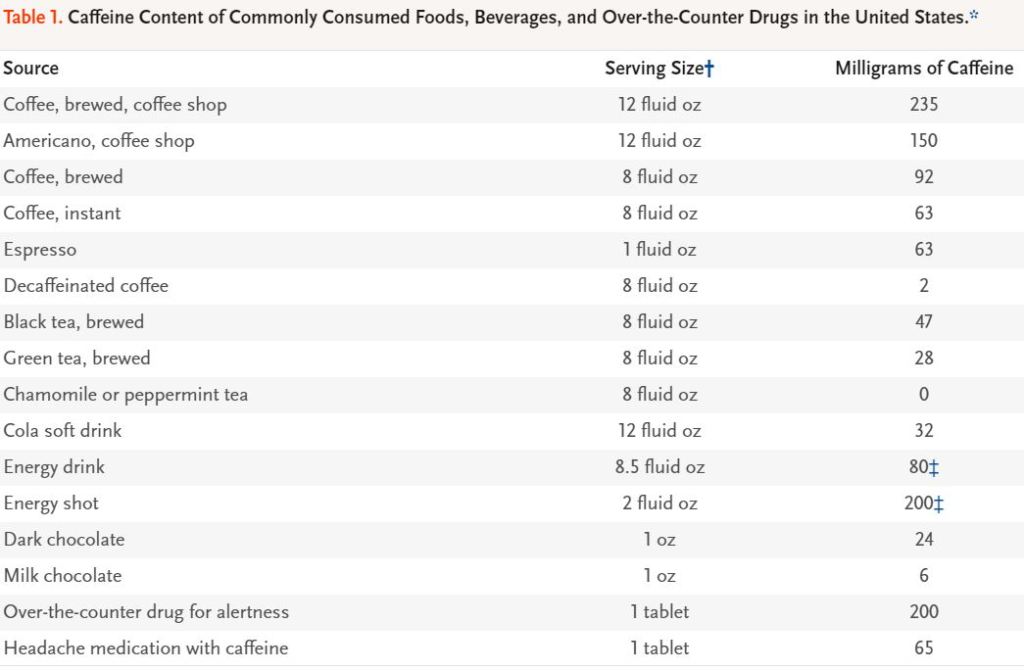
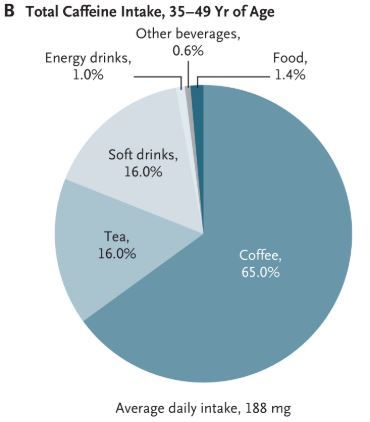
Coffee and tea have been consumed for hundreds of years and have become an important part of cultural traditions and social life.5 In addition, people use coffee beverages to increase wakefulness and work productivity. The caffeine content of commonly used sources of caffeine is shown in Table 1. For a typical serving, the caffeine content is highest in coffee, energy drinks, and caffeine tablets; intermediate in tea; and lowest in soft drinks. In the United States, 85% of adults consume caffeine daily,6 and average caffeine intake is 135 mg per day, which is equivalent to about 1.5 standard cups of coffee (with a standard cup defined as 8 fluid oz [235 ml]).7 Coffee is the predominant source of caffeine ingested by adults, whereas soft drinks and tea are more important sources of caffeine ingested by adolescents,
The pulmonary circuit oxygenates and the systemic arterial circuit circulates several Liters of blood per minute. As this blood trickles through the capillaries, some of it oozes out through the thin endothelial lining, becoming interstitial fluid.
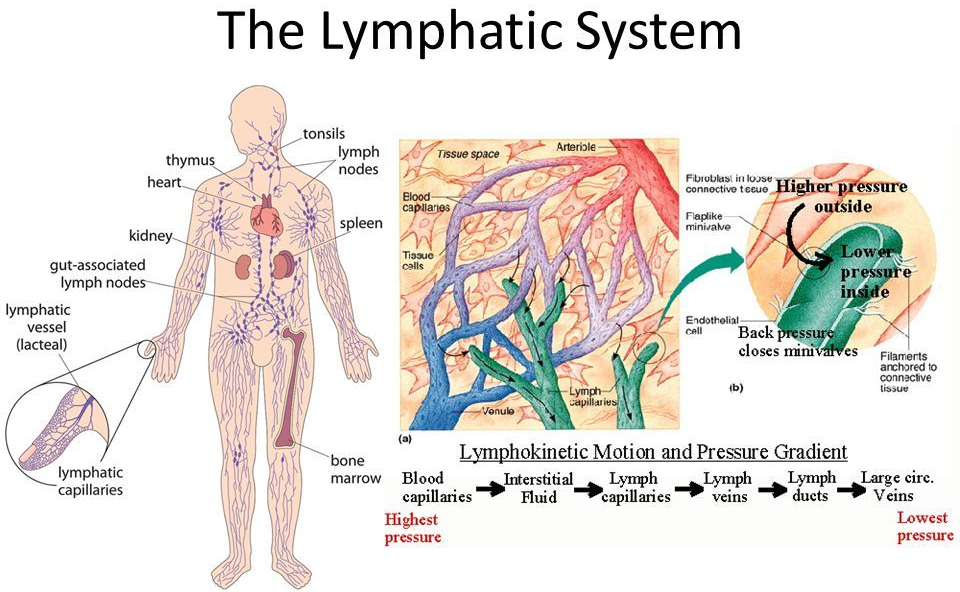
Most of this flud gets back into the capillaries and returns to the heart in the venous return. About 20% of the fluid drains into the LYMPHATIC SYSTEM, through the Lymph nodes, and back into the thoracic duct, into the vena cava, and eventually back into the general blood supply, which recirculates.
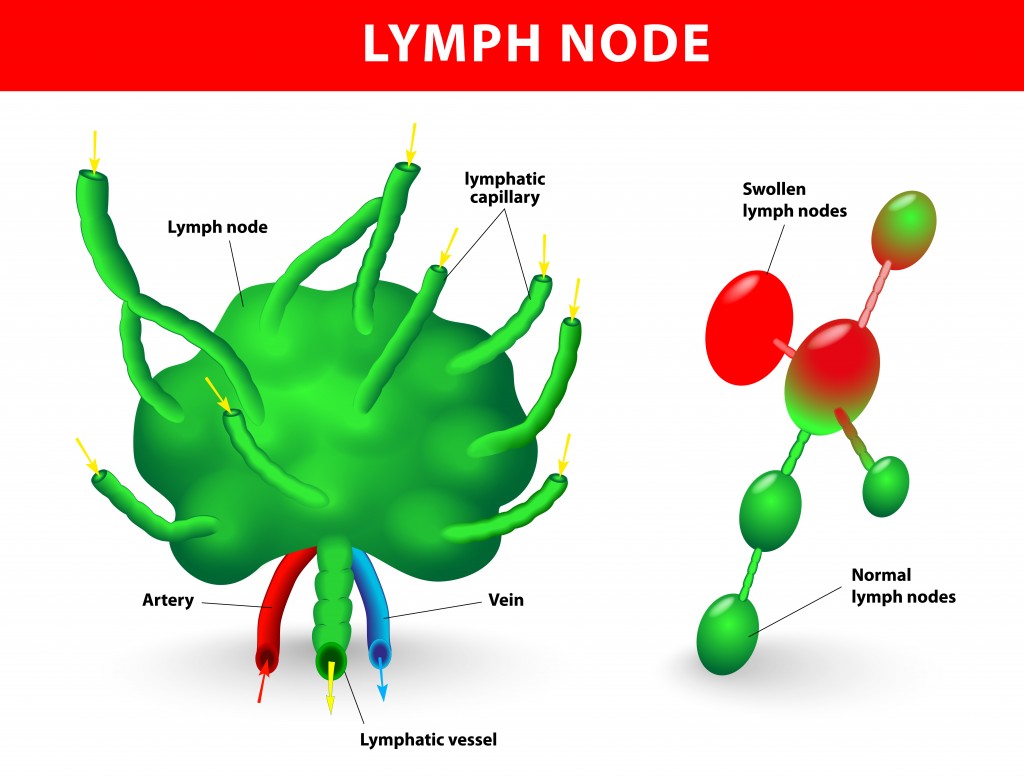
The Lymphatic System
The Return of the residual interstitial fluid by the Lymphatic vessels back to the general circulation is important, and if BLOCKED by such things as surgery and parasites, produces a swelling known as LYMPHEDEMA.
But the major importance of the lymphatic vessels is their characteristic cells, LYMPHOCYTES, and their accessory structures, The THYMUS, SPLEEN, LYMPH NODES, AND LYMPHATIC TISSUES is in the development and training of the IMMUNE SYSTEM. The THYMUS can be regarded as an organ to TRAIN Lymphocytes to be functional members of the immune system.
SomeT-cells operate to Help B-cells to produce antibody. These are called Th-4 cells. Others, called Th-8 cells. function to delete cells,
The thymus POSITIVELY selects cells that are prepared to recognize pathogens, and gets rid of cells (NEGATIVELY selects) cells that recognize the body’s own cells.
Failure to do so would result in “horror autotoxicus”, or AUTOIMMUNITY. The Thymus performs most of its functions when we are young.
The LYMPH NODES act as a type of filter for the Lymphatic channels, and intercept most bacteria and other pathogens coming through the lymphatic channes to keep them out of the blood stream. Lymph nodes are present at predictable locations throughout the body.
The Spleen acts as a big lymph node to filter the blood directly, and can intercept organisms that have escaped the lymph nodes. The Spleen can enlarge with certain infections, as with the EB Virus that causes mononucleosis.
Rupture of the spleen is not uncommon with direct blunt trauma to the abdomen. Removal of the spleen can increase susceptibility to blood stream infection. Lymph tissue is scattered throughout the body, like in the Tonsils, adenoids and Intestinal tract.
This Lymphocyte-containing tissue can expand with exposure to infection, and can become cancerous with Lymphomas. It can also enlarge enough to produce local Blockage, as with Adenoids. Lymph tissue should not be removed wantonly, since it may provide protection. There are 2 arms of our immune system.
I have been discussing the ADAPTIVE immune system which recognizes the pathogen, and stores memory of this interaction in “memory T-cells”. The helper T-cells( Th-4) start to multiply and stimulate the B-cells to “clonally” proliferate and differentiate into Antibody-producing Plasma Cells. The Cytotoxic T-cells, which can directly kill Pathogens, also multiply.
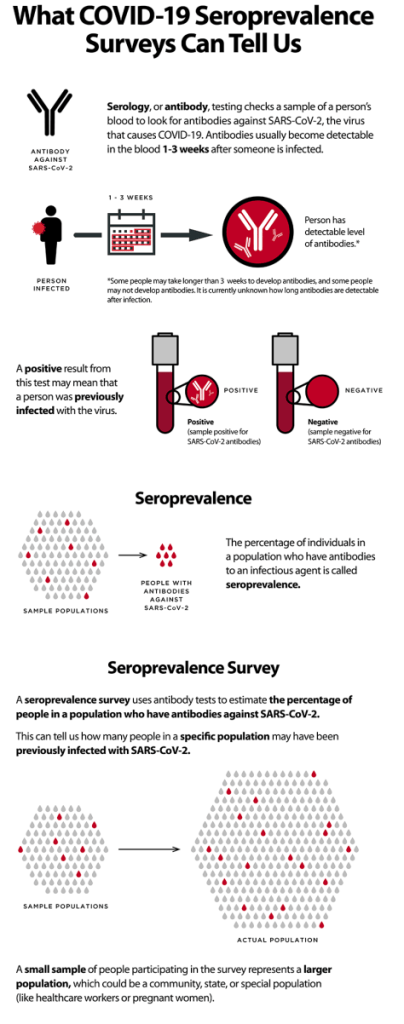
The first time this happens with a new Pathogen, Like SARS CoV-2, this adaptive process takes a week or so. But if the same Pathogen comes later, The adaptive immune system is ready, via the Memory T-cells, and springs rapidly into action. The 2nd arm of our immune system, shared with all of our vertebrate relatives, is the INNATE immune system.
The innate system is prepared IMMEDIATELY to recognize certain foreign molecules common to many invaders, and foreign our own bodies. It usually does not have the Power of the innate immune system, but in healthy people does an amazingly good job.
Some people just don’t get sick very often. Do the best you can to be one of these healthy people by getting proper SLEEP, DIET. AND EXERCISE!
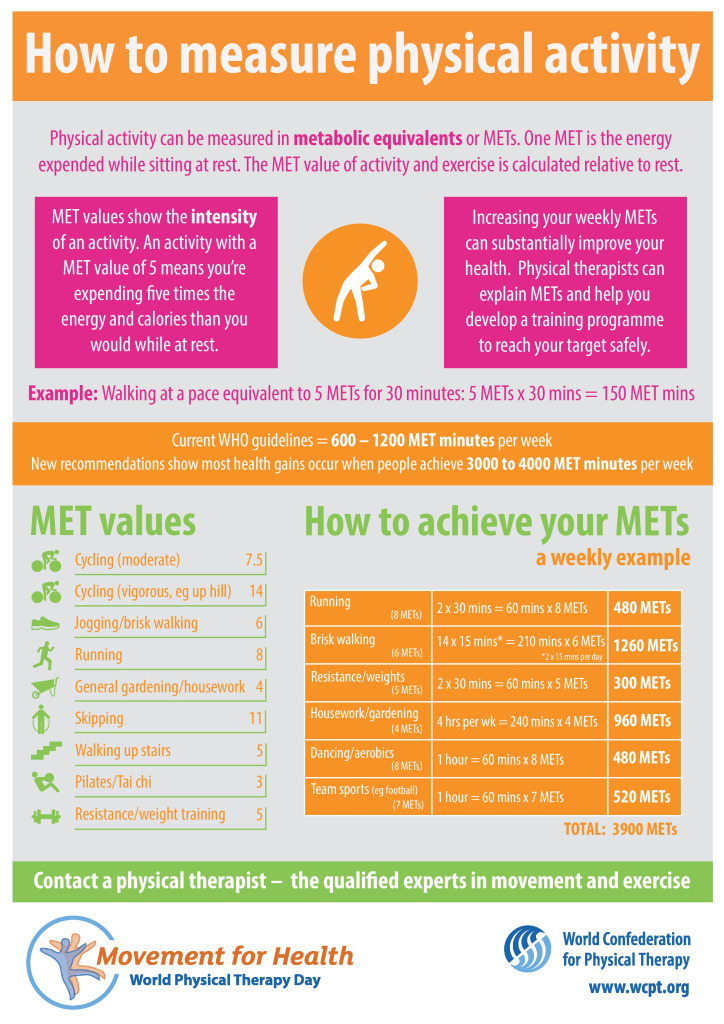
The idea of “METS” as a unit of energy expenditure is interesting and practical. I agree that EXERCISE IS IMPORTANT.
Frank Wilczek, in an article on Dyson Freeman, talked about another unit that I find even more interesting . He proposed that 100 Watts be the unit of energy expenditure. This is (approximately) the energy used in an old 100 Watt incandescent light bulb. It is also the amount of energy used by the “average” human on a 2000 Calorie diet.
Using this unit, the average U.S. Citizen uses 95 units, compared to a 25 unit world average. The suns output is 5 X ten to the fourteenth power, of which 1X ten to the fourth power units lands on earth. Good cocktail information.
I also read that a professional cyclist has an output of only 400 watts, vs. the 14 Mets mentioned in the article.but when I read that the human body is only 20-25% efficient in converting Calories to Watts of Output, 14 Mets made more sense.
I have heard the same story over and over. You get older, you trip over your dog or on the edge of a rug, you fall and break your hip, and in treatment or convalescence, you get a pneumonia and die, or at least you get weaker, setting you up for the next fall. Your course is downhill.
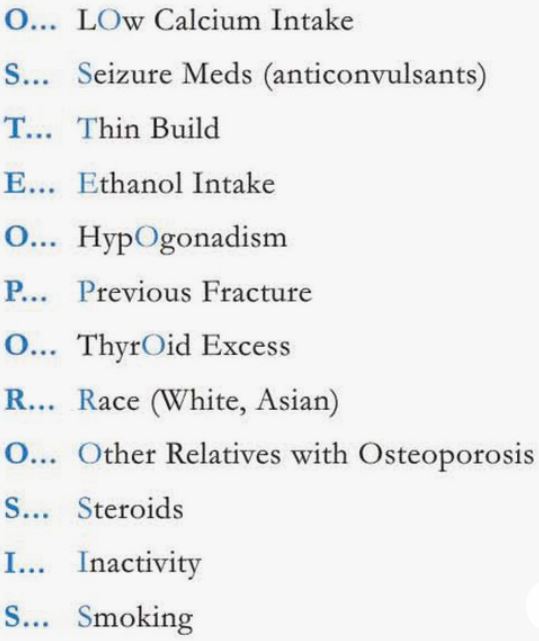
The culprit is often OSTEOPOROSIS. Osteoporosis is a disease characterized by loss of bone mass, as opposed to Osteomalacia, discussed in a recent podcast on this site, which is softening of bone The word itself is a MEMONIC for the RISK FACTORS; Then comes WHAT TO DO.
The RISK FACTORS and Prevention Strategies can be remembered in the following mnemonic:
Osteoporosis prevention begins when you are a child, with healthy diet rich in Calcium, and lots of exercise. Your bone mass peaks in the early 20s. While you are young, in your reproductive years, your reproductive hormones, Estrogen and Testosterone protect you.
Women should develop a Preventative strategy during menopause. Being THIN, like i am, is generally a marker of good health, much better than being Fat.
But especially as you get older and Lose muscle mass, Osteoporosis can become a problem, maybe because your bones don’t get the stress required to keep them strong.
BONE DENSITY DECLINES WITH AGE. I get a DEXASCAN as often as my insurance allows, about every 2 years, and am due this summer.
More and more treatments for Osteoporosis are emerging, if your bone loss becomes severe enough.
From The Lancet Diabetes & Endocrinology (June 2020):
Our findings show that the intensive lifestyle intervention led to significant weight loss at 12 months, and was associated with diabetes remission in over 60% of participants and normoglycaemia in over 30% of participants. The provision of this lifestyle intervention could allow a large proportion of young individuals with early diabetes to achieve improvements in key cardiometabolic outcomes, with potential long-term benefits for health and wellbeing.
Type 2 diabetes is affecting people at an increasingly younger age, particularly in the Middle East and in north Africa. We aimed to assess whether an intensive lifestyle intervention would lead to significant weight loss and improved glycaemia in young individuals with early diabetes..Between July 16, 2017, and Sept 30, 2018, we enrolled and randomly assigned 158 participants (n=79 in each group) to the study. 147 participants (70 in the intervention group and 77 in the control group) were included in the final intention-to-treat analysis population. Between baseline and 12 months, the mean bodyweight of participants in the intervention group reduced by 11·98 kg (95% CI 9·72 to 14·23) compared with 3·98 kg (2·78 to 5·18) in the control group (adjusted mean difference −6·08 kg [95% CI −8·37 to −3·79], p<0·0001). In the intervention group, 21% of participants achieved more than 15% weight loss between baseline and 12 months compared with 1% of participants in the control group (p<0·0001). Diabetes remission occurred in 61% of participants in the intervention group compared with 12% of those in the control group (odds ratio [OR] 12·03 [95% CI 5·17 to 28·03], p<0·0001). 33% of participants in the intervention group had normoglycaemia compared with 4% of participants in the control group (OR 12·07 [3·43 to 42·45], p<0·0001)
President Trump’s preferred coronavirus treatment is the focus of a new study suggesting it could cause more harm than good, but not everybody agrees. We discuss the fallout as trials around the world are paused and countries diverge over policy advice.
12:12 Are we rushing science?
Coronavirus papers are being published extremely quickly, while normally healthy scientific debate is being blown up in the world’s press. Is there a balancing act between timely research and accurate messaging?
18:49 One good thing
Our hosts pick out things that have made them smile in the last week, including hedgerow brews and a trip into the past using AI.