Mild cognitive impairment (MCI) is a condition in which people have more memory or thinking problems than other people their age. The symptoms of MCI are not as severe as those of Alzheimer’s disease or a related dementia. People with MCI can usually take care of themselves and carry out their normal daily activities.
People with MCI are at a greater risk of developing Alzheimer’s disease or a related dementia. Estimates vary as to how many people who have MCI will develop dementia. Roughly one to two out of 10 people age 65 or older with MCI are estimated to develop dementia over a one-year period. However, in many cases, the symptoms of MCI stay the same or even improve.
Research on sleep disorders and the importance of regular shut-eye has deepened our understanding of the link between sleep and brain health.
February 2023
Overall, there are more than 80 sleep disorders, ranging from the mildly annoying to the potentially deadly. The best known is probably insomnia; about 10 percent of the general population has chronic insomnia, an inability to fall asleep for multiple nights over a period of months.
Addressing sleep disorders “is paramount to not only protecting the brain down the road but also on a day-to-day basis,” says Daniel Barone, MD, associate medical director of the Weill Cornell Center for Sleep Medicine in New York City and co-author of The Story of Sleep: From A to Zzz (Rowman & Littlefied, 2023). “One of the best ways to take care of our brains is by getting quality sleep.”
Intriguing Clues
Research on sleep disorders has led to improvements in treatment for a variety of sleep and neurologic conditions. Case in point: Studies in the late 1990s on the causes of narcolepsy with cataplexy—the condition Connor was initially diagnosed with—led to the development of dual orexin receptor agonists, drugs now commonly prescribed to treat insomnia. The researchers discovered that people with narcolepsy with cataplexy often had low levels of hypocretins (orexins), brain chemicals that sustain alertness and prevent REM from happening at the wrong time.
“Once they found out, ‘If I take away your hypocretin, it makes you sleepy,’ there was a new idea of how to make a sleeping pill,” says Rafael Pelayo, MD, clinical professor of psychiatry and behavioral sciences at Stanford University School of Medicine in California and a sleep specialist at the university’s Sleep Medicine Center.
Research & review on #Alzheimers, global burden of benign prostatic hyperplasia, #WHO def of vitality capacity, IPD meta on social connection & #cognition, #oralhealth for older people & more.
Although intermittent fasting is most widely known as a weight-loss strategy, emerging research suggests that it could have benefits for brain health and cognition. But does it actually work, are there any drawbacks and how long would you have to fast to see benefits?
WSJ’s Daniela Hernandez breaks down what’s known and what’s not about the neuroscience of intermittent fasting.
Video Timeline: 0:00 Could intermittent fasting help our brains work better and longer? 0:31 How long would you have to fast to see any potential cognitive benefits? 1:04 How intermittent fasting could affect your ability to focus 2:27 Potential mood-related benefits of intermittent fasting 2:48 How intermittent fasting can affect brain health 4:03 Potential drawbacks of intermittent fasting
Opportunities for enhancing brain health across the lifespan
Published online by Cambridge University Press: 22 March 2021
Summary
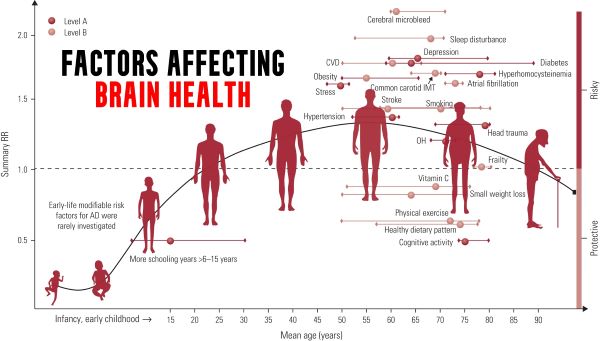
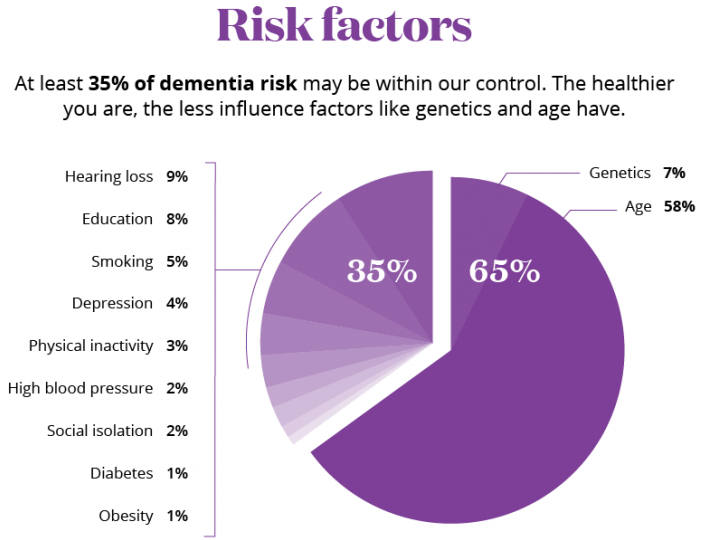
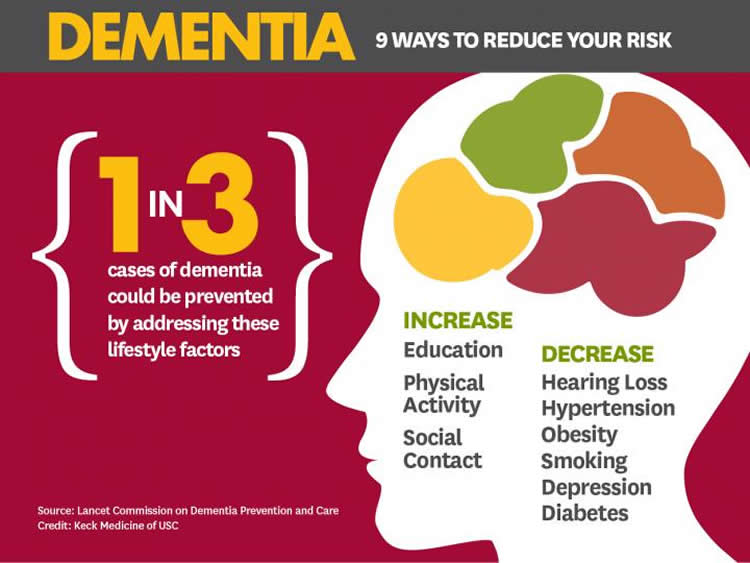
As we age, there are characteristic changes in our thinking, reasoning and memory skills (referred to as cognitive ageing). However, variation between people in the timing and degree of change experienced suggests that a range of factors determine individual cognitive ageing trajectories. This narrative review considers some of the lifestyle factors that might promote (or harm) cognitive health. The focus on lifestyle factors is because these are potentially modifiable by individuals or may be the targets of behavioural or societal interventions. To support that, the review briefly considers people’s beliefs and attitudes about cognitive ageing; the nature and timing of cognitive changes across the lifespan; and the genetic contributions to cognitive ability level and change. In introducing potentially modifiable determinants, a framing that draws evidence derived from epidemiological studies of dementia is provided, before an overview of lifestyle and behavioural predictors of cognitive health, including education and occupation, diet and activity.
We ARE our brains. Reduce the function of any other organ, and we may be sick, but reduce the function of the brain, and WE have changed.
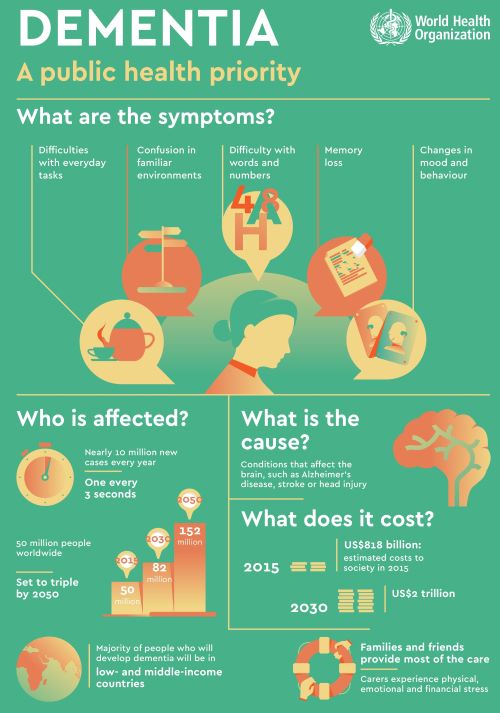
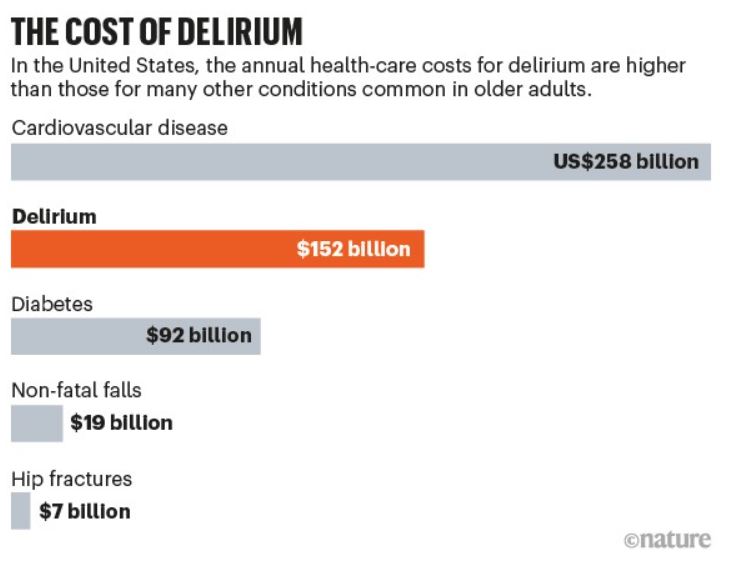
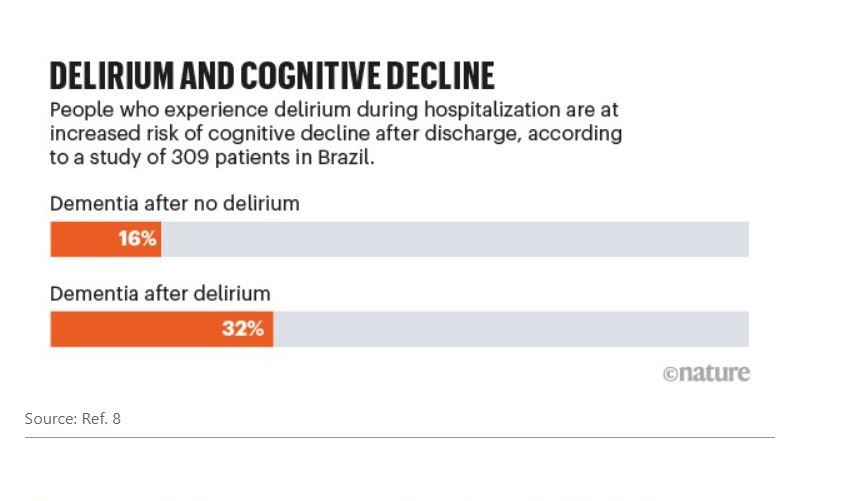
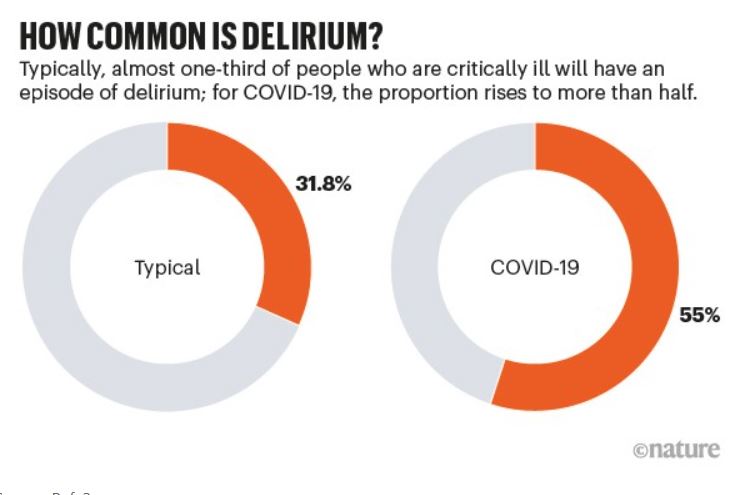
PROGRESSIVE LOSS of brain function is called DEMENTIA. A sudden, temporary (if the cause can be found) is called Delirium. A variety of bad things can cause dementia, such as infections (AIDS), toxins (lead, mercury), chemicals (alcohol), traumatic (CTE from football), diet deficiencies (B12, folic acid), Endocrine deficiencies (thyroid),Psychiatric problems (depression), drugs, and Vascular problems.
The Preceding article on dementia discussed APATHY, as opposed to the somewhat similar DEPRESSION, as a warning sign for SVD, or small blood-vessel disease. SVD is the most common VASCULAR cause of Dementia.
The most common overall cause of Dementia, especially in old age, is ALZHEIMER’S disease (AD). “Senior Moments” are so common as to be a cliche. But this problem is not limited to old age. My 3-year-old Grandson came crying to me that he lost his favorite toy. “Where was it when you last saw it”?, I asked. “It was in my hand” he answered.
He had laid it somewhere, unthinkingly. You can’t remember something unless you ENCODE it. You must be paying attention to, be “mindful” of an action if you are to remember that action.. You will not remember where you put your glasses if you wander around in “default mode”, daydreaming, preoccupied. Everybody occasionally forgets a name, or item which hangs on “the end of my tongue”.
These things, especially “short term memory” do DETERIORATE AS WE GET OLDER. It is common to wonder if we, or a loved one. are getting Alzheimer’s disease, as our mental powers wane.It is often difficult to distinguish the normal forgetfulness of age from DEMENTIA, including Alzheimer’s Disease (AD) It might be a source of REASSURANCE to realize that if you are worried about getting AD YOURSELF, you almost certainly don’t have it; It takes a lot of mental functioning to contemplate that possibility.
Most often, you will be wondering about the possibility in a loved one having AD. There are 2 ideas that I ran across in my reading that might help you do a little evaluation Yourself.
BCGuidelines.ca has a 21 item questionnaire that you can score yourself. 4 points or less is considered normal, so common is forgetfulness. 5-14 points suggests mild cognitive impairment. 15 or more points suggests Dementia, of which AD is the most common type.
The test I really liked was the “Clock Test”. In this test, you draw a large circle. You then ask your loved one to draw a clock, with all the numbers and hands that will indicate 10 minutes after 11. If it is drawn correctly, you can with reasonable certainty EXCLUDE Dementia.
If incorrect, further tests are warranted. I consulted with a Neurologist regarding a friend of mine who has marked memory loss, but is very sweet, is physically capable, takes care of herself personally, doesn’t wander around, has no apparent anxiety, depression or other psychological problems.
I asked if it was reasonable to just watch without any medical intervention. The neurologist said that she should have a blood test, a metabolic panel, TSH (thyroid), LFTs, folic acid and B12 tests, and a CT to rule out NPH (normal pressure hydrocephalus). It is rare to find anything treatable, but a shame to neglect it if present.
If you do see a doctor about a Spouse or Parent with possible dementia, you might request that they discuss the possibilities with you, but ask them not to write the diagnosis of “Alzheimer’s “ in the chart. Private Assisted Living Homes CHARGE A LOT MORE for that Diagnosis– locked facilities, more personnel and the like. BDNF- brain derived neurotrophic factor- can fend off Dementia.
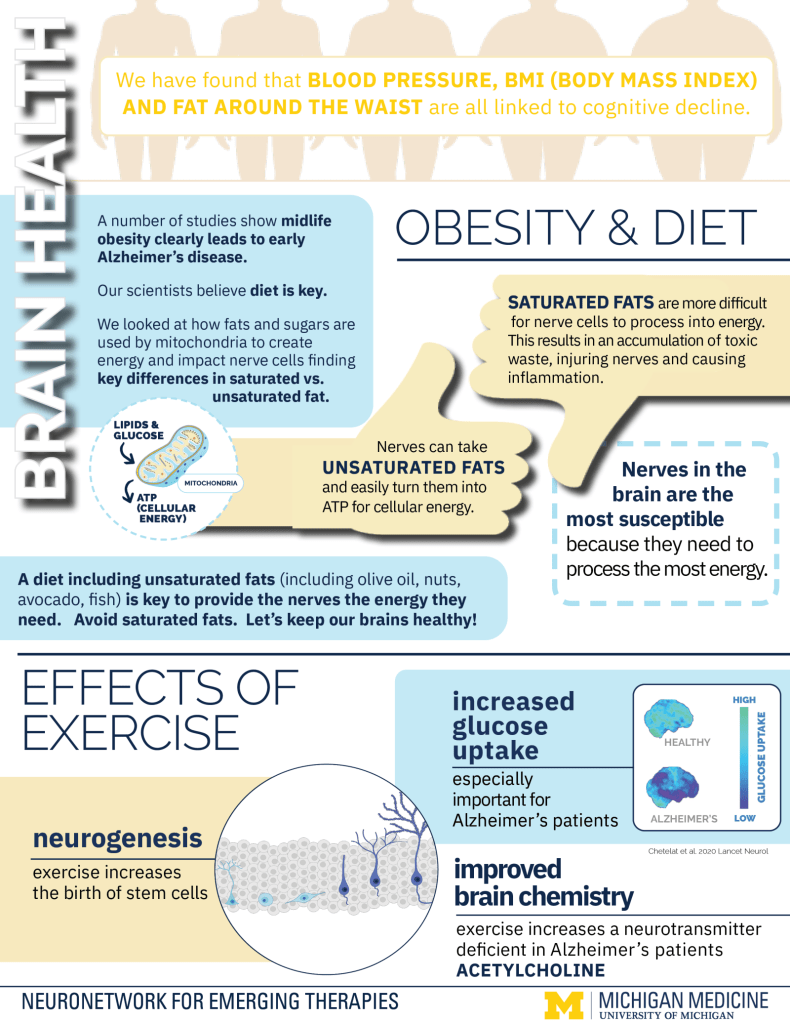
That is the good news. The bad news is that it takes effort and discipline to increase your level od BDNF.; I’m sure medical science is hot on the trail of a pill. But until then, our old friends, Sleep, Diet and Exercise ride to the rescue. Sleep, both N3 and REM stages, increases BDNF. Dietary polyphenols and butyrate increase BDNF. exercise of all kinds will do it.
The BDNF gene codes for the BDNF protein, which promotes the survival, expansion, and differentiation of Neuronal stem cells, and promotes neuronal PLASTICITY, neuronal response to experience. Grit your teeth and develop the HABIT of exposing your Postmodern Body to 3 of the most ICONIC and NATURAL things mandated by Evolution, Treat your Body to the Health-giving Benefits of SLEEP, DIET and EXERCISE!
–Dr. C
Empowering Patients Through Education And Telemedicine