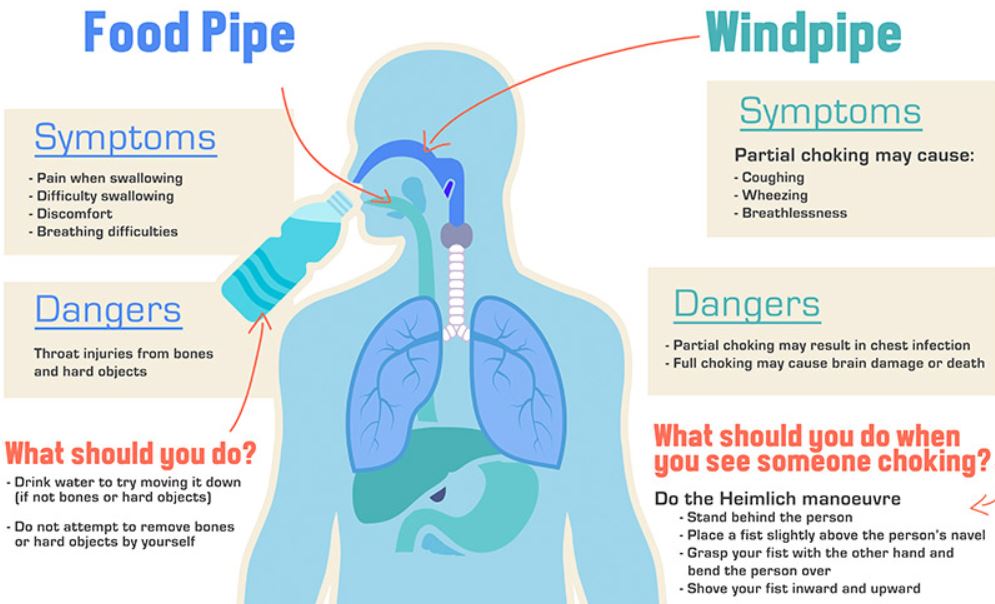
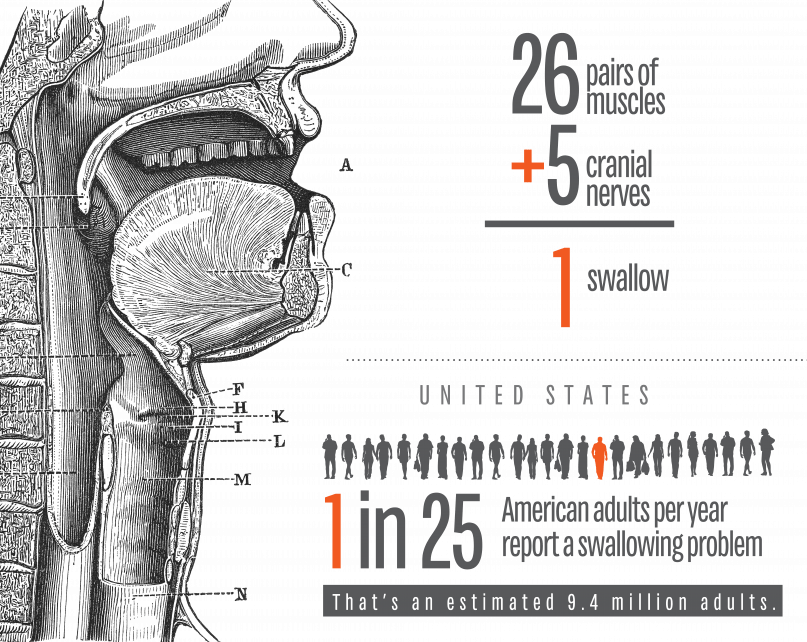
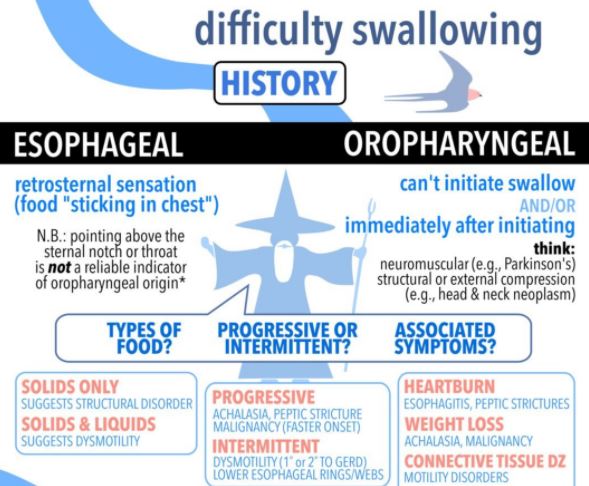
I am defining SWALLOWING TROUBLE as the difficulty in transport of food to the stomach, once clear of the throat. Problems with the initiation of the swallowing process are discussed separately.
PAIN in the mid-chest ON SWALLOWING is a worrisome symptom which can be due to inflammation of the lining of the esophagus from a variety of causes. An esophageal yeast infection, which can also involve the throat (called ‘“thrush”), often warns of immune deficiency and can be a sign of AIDS, or be caused by immune suppressing medication. If persistent, pain on swallowing can be a warning sign of CANCER.
If in the presence of GERD, it can be a sign of chronic inflammation or ulceration. In-coordination of the normally smooth muscular propulsive wave can cause a cramping, muscular pain.
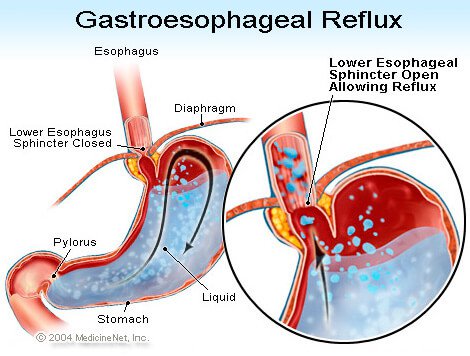
Normal “peristalsis” is so efficient, that food can be swallowed without the help of gravity, when UPSIDE DOWN. I wouldn’t recommend trying this, even to cure hiccoughs. There is a muscular “gate” at the bottom of the esophagus, just as it enters the stomach. This gate is often too relaxed, and allows for the reflux of acid and food from the stomach, or GERD. It can also Fail to open, called achalasia, and hold up the food in its journey to the stomach.
The area can be scarred by repeated acid reflux, and become NARROWED; this is called a STRICTURE, and can cause a blockage in swallowing. One of my Doctor friends had to go to the Emergency room when some Steak got stuck in the esophagus.
The ER Doctor removed the steak with a fiberoptic Scope, and then proceeded to DILATE the stricture with a “bougie”, an instrument of a precisely calibrated size designed to STRETCH the constricted area. This uncomfortable procedure had to be done repeatedly, a caution to those who would wait too long before getting such a problem evaluated and corrected.
EOSINOPHILIC ESOPHAGITIS has been diagnosed with increasing frequency, and can cause Pain in the middle of the chest, trouble swallowing, and even regurgitation of food. This special type of inflammation is more common in allergic patients, and can be caused by certain foods.
So as you can see, swallowing trouble, if persistent, is nothing to fool around with, and should be checked out by a competent doctor. Don’t wait too long.