If you have endometriosis, you’re all too familiar with the heavy periods, pain and nausea it can cause. Eating these foods might help control the pain and make all the difference.
Chapters: 0:00 Introduction 0:10 What is endometriosis? 0:45 Eating the right foods can help the body fight inflammation 1:01 Fiber rich foods 1:41 Omega-3 fats 2:10 Monounsaturated fats 2:30 Magnesium and zinc 3:25
It’s always important to eat good, healthy food Resources: The Best and Worst Foods for an Anti-Inflammatory Endometriosis Diet – https://cle.clinic/3VeYzyG
In this instructional video, Drs. Jane Leopold, Elliott Antman, William Sauer, and Paul Zei provide an overview of the classification and diagnosis of atrial fibrillation, management strategies, and mitigation of stroke risk with anticoagulation therapy.
Video timeline:0:00 Pathophysiology and Symptoms 3:11 Stroke Risk, Anticoagulants, and Arrhythmia Control 6:32 Catheter Ablation 10:11 Post-Procedural Monitoring and Care
The video also focuses on the new rhythm-control strategy of catheter ablation therapy, with attention to the success rate, potential complications, postprocedural monitoring for recurrence of atrial fibrillation, and consideration of ongoing anticoagulation therapy in these patients. The New England Journal of Medicine is the world’s leading general medical journal.
Continuously published for over 200 years, the Journal publishes peer-reviewed research along with interactive clinical content for physicians, educators, and the global medical community at https://NEJM.org.
COMMENTARY:
This is a very good video well worth watching by general physicians and interested patients. There are several general and some specific comments I would like to make.
First, in my opinion, the best physician is none too good. In any operative or serious procedure, the decision to operate should be made by the patient in conjunction with a physician that does not do the operating. In my case, as a physician, I consulted an electrophysiologist.
Second, in my opinion, a good medicine is better than surgery. For atrial fibrillation, there has been no new medication treatment for decades. The main drugs are still amiodarone and Propafenone. The latter is less consistently effective, but has a better long-term safety profile; amiodarone often produces ‘floaters” in the eye, and Propafenone merely a bitter taste which you’ll get used to.
Third, it must be realized that catheter ablation is often not curative, especially as you get older, which was rather glossed over in this video. Ablation also requires a great deal of expensive equipment, which is constantly evolving, hence the importance of getting your ablation at a major center where it is done all the time. These major centers have less complications such as atrial wall perforation; Yes, you can rarely wind up worse off after any operation.
I am a physician, currently 90 years old. I developed atrial fibrillation of the persistent type when I was in my late 70s. I had a cardioversion to get me into sinus rhythm, and then tried Propafenone, which kept me in sinus rhythm for less than a month. My main motivation to get a radio frequency ablation was to stay off of anticoagulants. I had my ablation, and remained in sinus rhythm, and off anticoagulants, for three years. I could always tell when I went into atrial fibrillation from normal sinus rhythm because I produced a lot of urine and had to go to the bathroom all the time; atrial fibrillation causes release of a hormone called atrial naturetic peptide. I could also tell by taking my own pulse, which was quite irregular in comparison to my very regular sinus rhythm pulse, which ticked along with a rate in the high 50s. I had always thought my rate was low because I exercise a lot. Actually, my EKG shows a second-degree heart block which is probably partially responsible.
After three years, I returned to atrial fibrillation, and needed a another ablation. They found very few areas of abnormal electrical activity, and gave me a “touchup”, which lasted another two or three years after which I went back into atrial fibrillation. Probably as a result of my age, a fibrillated at a slow rate, and at least did not need any extra medication for rate control, although I did, of course, need to take a regular anticoagulant, in my case Eliquis.
In summary, atrial fibrillation is a common electrical storm in the upper chambers of the heart, causing a rapid, irregular beat. AF increases in frequency as you get older. In the video they mention the “substrate”, which is the structure of the atrium. In my own case, this was an enlarged atrium, and probably a tendency towards atrial fibrillation; my brother also has AF. The main complication is stagnation of blood in the atria, resulting in increased tendency toward stroke. Fibrillation therefore requires an anticoagulant.
There is some discussion about the irregular rate causing an inefficiency of cardiac action, contributing to heart failure, This is logical, but not clear cut statistically.
For women and people assigned female at birth (AFAB), taking care of your health requires more than an annual physical. You should also visit a women’s health specialist — like an Ob/Gyn, midwife or nurse practitioner — each year to keep healthy. More than just a checkup for your breasts/chest and reproductive organs; well-woman exams can also help you develop rapport with a women’s health specialist.
“Well-women exams are important for a number of reasons. No. 1 is that they help you to establish care with a specialist so that if there is a problem down the road, you have a provider that you know and feel comfortable talking to,” says Ob/Gyn Amanda Elbin, MD.
That comfort level is important, too, especially because many of us may not feel comfortable talking with just anyone about issues “down there.”
Even mild COVID-19 is at least correlated with a startlingly wide spectrum of seemingly every illness. We need a much better taxonomy to address people’s suffering.
Long Covid – Whole Body Symptoms
From The Atlantic, October 5, 2022:
The cases of long covid that turn up in news reports, the medical literature, and in the offices of doctors like me fall into a few rough (and sometimes overlapping) categories. The first seems most readily explainable: the combination of organ damage, often profound physical debilitation, and poor mental health inflicted by severe pneumonia and resultant critical illness.
This serious long-term COVID-19 complication gets relatively little media attention despite its severity. The coronavirus can cause acute respiratory distress syndrome, the gravest form of pneumonia, which can in turn provoke a spiral of inflammation and injury that can end up taking down virtually every organ. I have seen many such complications in the ICU: failing hearts, collapsed lungs, failed kidneys, brain hemorrhages, limbs cut off from blood flow, and more. More than 7 million COVID-19 hospitalizations occurred in the United States before the Omicron wave, suggesting that millions could be left with damaged lungs or complications of critical illness. Whether these patients’ needs for care and rehabilitation are being adequately (and equitably) met is unclear: Ensuring that they are is an urgent priority.
A transient ischemic attack (TIA) is sometimes called a “mini-stroke.” It is different from the major types of stroke, because blood flow to the brain is blocked for only a short time—usually no more than 5 minutes.1
Ischemic stroke
Most strokes are ischemic strokes.2 An ischemic stroke occurs when blood clots or other particles block the blood vessels to the brain.
Fatty deposits called plaque can also cause blockages by building up in the blood vessels.
Hemorrhagic stroke
A hemorrhagic stroke happens when an artery in the brain leaks blood or ruptures (breaks open). The leaked blood puts too much pressure on brain cells, which damages them.
High blood pressure and aneurysms—balloon-like bulges in an artery that can stretch and burst—are examples of conditions that can cause a hemorrhagic stroke.
Transient ischemic attack (TIA or “mini-stroke”)
For Blanche Teal-Cruise, a smoker for 40 years who also had high blood pressure, the transient ischemic attack (sometimes called a mini-stroke) she had on the way to work was a wake-up call. Read Blanche’s story.
TIAs are sometimes known as “warning strokes.” It is important to know that
A TIA is a warning sign of a future stroke.
A TIA is a medical emergency, just like a major stroke.
Strokes and TIAs require emergency care. Call 9-1-1 right away if you feel signs of a stroke or see symptoms in someone around you.
There is no way to know in the beginning whether symptoms are from a TIA or from a major type of stroke.
Like ischemic strokes, blood clots often cause TIAs.
More than a third of people who have a TIA and don’t get treatment have a major stroke within 1 year. As many as 10% to 15% of people will have a major stroke within 3 months of a TIA.1
Recognizing and treating TIAs can lower the risk of a major stroke. If you have a TIA, your health care team can find the cause and take steps to prevent a major stroke.
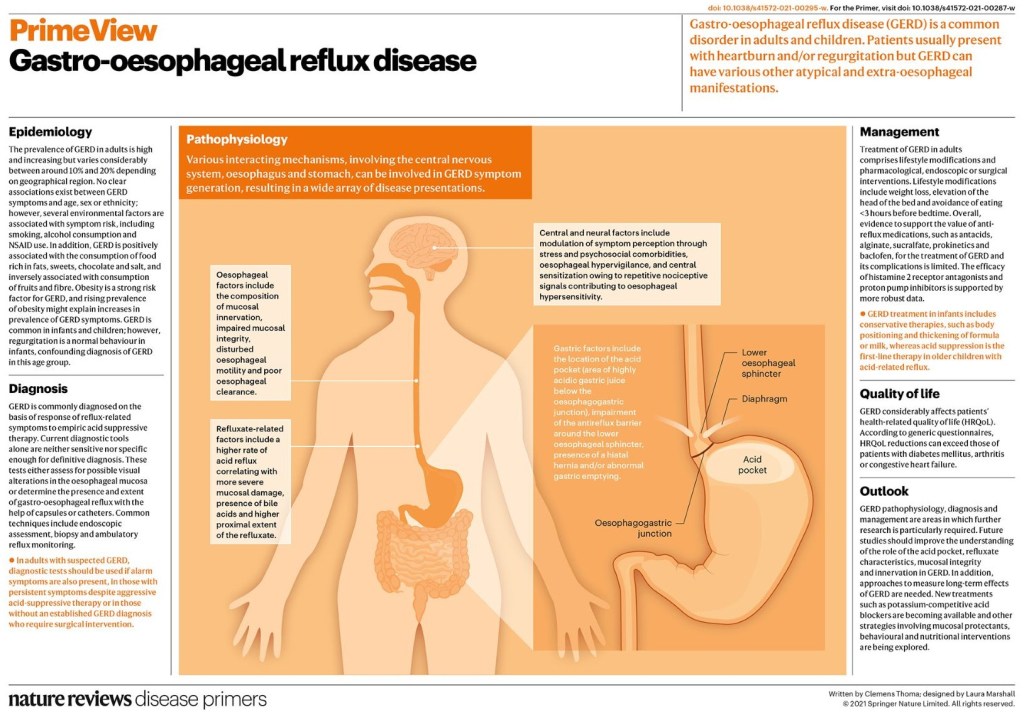
Gastro-oesophageal reflux disease (GERD) is a common disorder in adults and children. The global prevalence of GERD is high and increasing. Non-erosive reflux disease is the most common phenotype of GERD. Heartburn and regurgitation are considered classic symptoms but GERD may present with various atypical and extra-oesophageal manifestations. The pathophysiology of GERD is multifactorial and different mechanisms may result in GERD symptoms, including gastric composition and motility, anti-reflux barrier, refluxate characteristics, clearance mechanisms, mucosal integrity and symptom perception.
In clinical practice, the diagnosis of GERD is commonly established on the basis of response to anti-reflux treatment; however, a more accurate diagnosis requires testing that includes upper gastrointestinal tract endoscopy and reflux monitoring. New techniques and new reflux testing parameters help to better phenotype the condition. In children, the diagnosis of GERD is primarily based on history and physical examination and treatment vary with age.
Treatment in adults includes a combination of lifestyle modifications with pharmacological, endoscopic or surgical intervention. In refractory GERD, optimization of proton-pump inhibitor treatment should be attempted before a series of diagnostic tests to assess the patient’s phenotype.
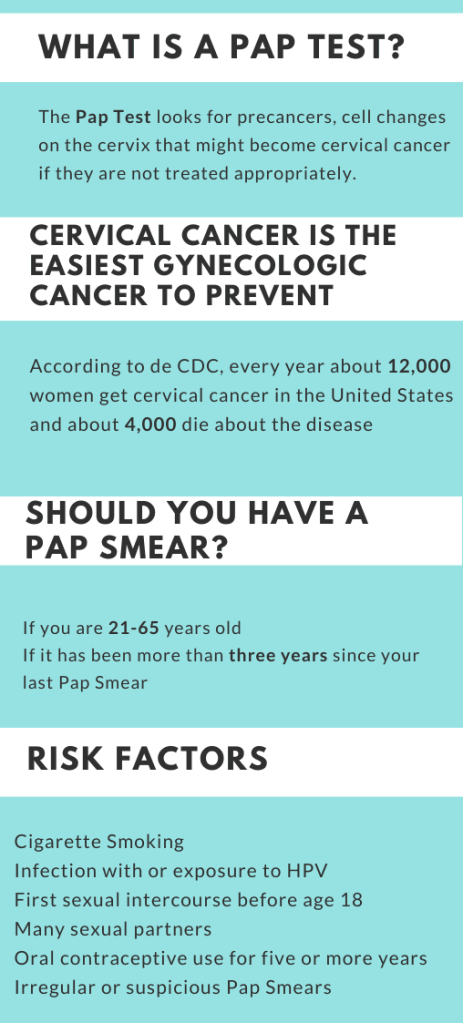
A women’s lifetime risk of developing breast cancer is one in eight. Research has shown that the earlier you detect breast cancer the more options there are for treatment and a better chance for a cure.
What is a mammogram?
A mammogram is a low-dose X-ray of breast tissue. Healthcare providers use mammograms, or mammography, to look for early signs of breast cancer before symptoms develop. This is called a screening mammogram. Providers also use mammography to look for any abnormalities if you develop a new symptom, such as a lump, pain, nipple discharge or breast skin changes. This is called a diagnostic mammogram.
Aside from skin cancer, breast cancer is the most common cancer that affects people assigned female at birth and represents 14% of all new cancer diagnoses in the United States. While breast cancer treatment therapies continue to improve and have contributed to a reduction in cancer-related deaths, early diagnosis through screening mammograms has a greater overall impact on survival rates.
Each year, medical diagnosis errors affect the health of millions of Americans and cost billions of dollars. Machine learning technologies can help identify hidden or complex patterns in diagnostic data to detect diseases earlier and improve treatments.
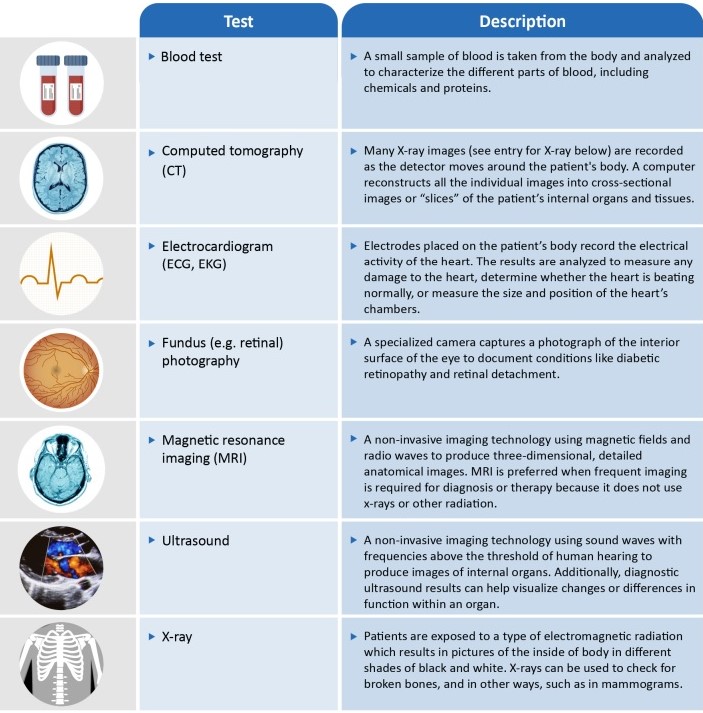
Several machine learning (ML) technologies are available in the U.S. to assist with the diagnostic process. The resulting benefits include earlier detection of diseases; more consistent analysis of medical data; and increased access to care, particularly for underserved populations. GAO identified a variety of ML-based technologies for five selected diseases
Certain cancers,
Diabetic retinopathy,
Alzheimer’s disease,
Heart disease,
COVID-19
Most technologies relying on data from imaging such as x-rays or magnetic resonance imaging (MRI). However, these ML technologies have generally not been widely adopted.