The normal adult heart beats almost as regularly as a metronome, between 60 and 100 beats per minute. I say ALMOST, because when you let your breath out, the VAGUS nerve slows the normal heart slightly.
This is called Sinus Arrhythmia; SINUS because the electrical signal for the heart to contract originates in the usual place, the SINUS NODE.
ARRYTHMIA refers to the irregularity of the beat. Normally, the sinus node originates the electrical impulse, automatically generating the rhythm. The impulse spreads in an organized fashion throughout the Atria causing them to contract and send the collected blood to the ventricles.
The AV node is then activated, and after a slight delay, to allow the ventricles to fill, the impulse spreads to the Ventricles, causing them to contract, The heart is designed to be most efficient above 50 beats per minute, and below about 120. The rate is higher in the young and athletic. Athletes often have an efficient resting pulse in the 40s.
The arrhythmias usually cause the heart to beat too FAST. The most common arrhythmia is ATRIAL FIBRILLATION. In this condition, the upper chambers, the Atria, do not beat in a coordinated manner. The sinus node no longer regularly originates the electrical impulse because the electrical activity is continuously traveling in a disorganized way throughout the upper chambers in a self-propagating manner.
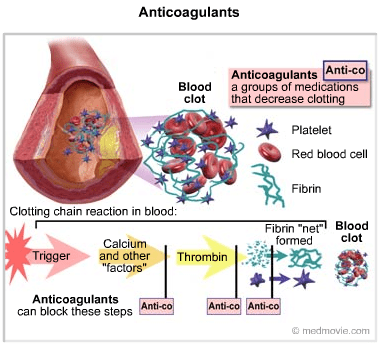
This quivering of the Atria allows the blood to pool in an area called the Atrial Appendages. This stagnant, pooled blood tends to clot, particularly if there is inflammation already present in the heart from vessel damage, obesity, or simply old age.
These CLOTS may find their way into the systemic circulation, and cause a STROKE. Another symptom of Atrial fibrillation is related to the irregular beats, which creates the sensation of PALPITATIONS, which causes you to be AWARE of your heart beating, and can be disturbing.
ATRIAL FLUTTER, and SUPRAVENTRICULAR TACHYCARDIA are other Arrhythmias. Some conditions cause the heart rate to be too SLOW. SICK SINUS SYNDROME is when the sinus node, the PACEMAKER, becomes more and more disordered, sometimes causing the heart to slow excessively, and produce FAINTING, sometimes producing a rapid heart rate.

Heart block is where the signal from the atria don’t reach the ventricles properly, sometimes not at all. The unsignaled ventricles still beat, but more slowly by an intrinsic, “idioventricular” rhythm.
My own experiences with ATRIAL FIBRILLATION will illustrate the problem and it’s treatment. A RAPID HEART BEAT was my introduction into arrhythmias. The rate was 140, and the EKG showed ATRIAL FLUTTER.
My Doctor gave me some PROPAFENONE to attempt a “chemical conversion” but it didn’t work, and i was given a CARDIOVERSION in the ER. The Arrhythmia returned in the form of ATRIAL FIBRILLATION within a couple of weeks. Back to the ER, and another cardioversion.
I was given propafenone, but that didn’t hold me much longer. A RADIOFREQUENCY ABLATION, where the focal points of aberrant electrical activation were isolated kept me in SINUS RHYTHM for a couple of years.
When the Fibrillation returned, Propafenone worked for a while, after which another Ablation, more propafenone, bood level regulation of propafenone to peak at night ( I invariably started fibrillation at night) and so on. With periodic trips to the ER for Cardioversion, I got by for a Decade.
Finally, when regulating the Propafenone couldn’t hold me in Sinus Rhythm longer than a month, I gave up, let myself go on fibrillating, and started taking ELEQUIS to PREVENT EMBOLI AND STROKE. Back when I first started fibrillating I had 2 main reasons for wanting to return to sinus rhythm..
First, I wanted to avoid ANTICOAGULANTS, which initially meant WARFARIN, and regular blood checks. At least, when I finally resigned myself to Fibrillation, Eliquis was available.
The second reason was to avoid medications, including beta blockers,which would be necessary to keep my heart rate in the acceptable range, 80 or below. By the time I gave up on controlling the AF, my rate was in the 70s, going down into the 50s, even while fibrillating.
This good fortune may have been caused another mild heart aberration I had all along, a Partial BUNDLE BRANCH BLOCK, which slowed down the electrical signals to my ventricles. Sometimes you get lucky, and 2 “wrongs” sometimes DO make a “right”. But don’t count on it.
Keep yourself as healthy as possible. Atrial fibrillation is more common with obesity and heart disease. SLEEP APNEA is also a cause, and should be ruled out if you develop Atrial fibrillation. I had a Sleep study, which showed that I had Sleep Apnea, which will be a story i will tell later.