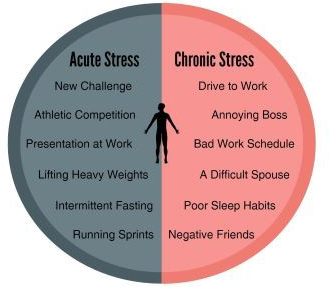
Stress in modern times most often has a BAD connotation. Stress is blamed for a raft of disorders from headaches to cardiovascular disease. Indeed, stress activates the adrenocortical “alarm reaction”, and if unremitting can indeed implement many chronic problems.
ACUTE stress, however, is often beneficial. The body responds favorably to measured amounts of brief stress, especially if it is YOUR CHOICE, and not demanded of you. It is WORK, when you would rather be doing something else. It is FUN when you are hiking up a steep but beautiful trail in the Swiss Alps. The flavor of reality takes place in the mind.
HEAT SHOCK PROTEINS (HSP) illustrates how your body works. If you get a little overheated, HSPs are produced and benefit any misfolded proteins that result. If you go hungry, a metabolic pathway burns fat and increases insulin sensitivity. If you exercise your mind, BDNF and new neurons result.
THE BODY ADJUSTS TO THE DEMANDS, and benefits flow. The body is designed to function. The trouble is that placing demands on the body is effortful, and effort requires discipline. The Paleolithic Hunter-gatherer lifestyle, the reality to which our metabolism is attuned, REQUIRED plenty of aerobic exercise, just to get food and avoid harm.
Our modern life is replete with deadlines and requirements, and hearts beat rapidly from ANXIETY rather than aerobic demand. Even the trades, which used to require physical energy expenditure have a lot of labor-saving devices. Children, insead of running, ride around on electrically propelled scooters. Little wonder that people are “out of shape” and gaining weight.
Old age is an inevitable condition if you are lucky enough to live a long life. Middle aged people say it begins at 70 years of age. According to an Elysium survey of people 40 and older, the average American FEELS old for the first time at age 47 years.
In the distant past, 50 was CONSIDERED to be old. The generally better conditions and Medicine of modern times keeps extending LIFESPAN, if not always HEALTHSPAN. Old age is certainly a Condition, and it is for sure Chronic, thereby qualifying for inclusion, but is it a Disease?
It is not considered a disease by the authorities, and so it doesn’t gather research funds like it should. What exactly IS old age? Being 88 Years old, and a physician, I feel qualified to comment. Old age is a collection of past accidents and sports injuries plus complications of past illnesses engrafted on a gradually deteriorating body.
Where does Obesity and Metabolic syndrome fit in this rubric? The Plague of our time fits in the disease category. It is definitely preventable, although with difficulty. Please search past postings for more information on this topic.
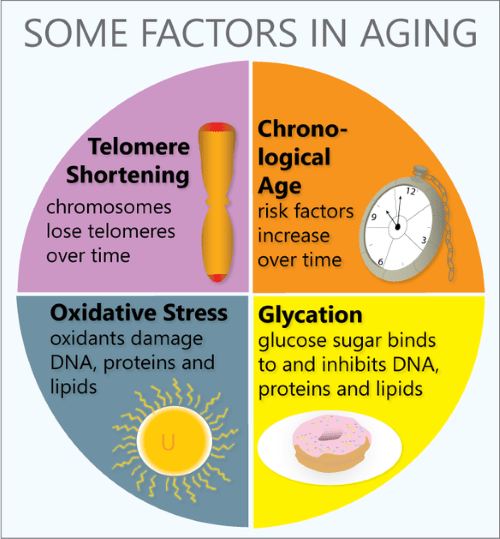
In what way does the body gradually deteriorate? Any organized, non-random high information structure gradually becomes more disordered, and “worn away” with the passage of TIME, the destroyer. Entropy (disorder) gradually increases, in the absence of corrective energy input.
Even rocks and mountains eventually erode, given enough time. One of the most interesting characteristics of life is that it maintains its integrity for an inordinate amount of time, given its complexity and furious dynamism.
Every day our DNA sustains thousands of molecular ruptures from high energy radiation and other stressors. Proofreading and repair mechanisms are employed, at high energy cost, to repair these breaks. This corrective is especially efficient when we are young and vigorous; In our youth, our reproductive years, growth and repair predominate. Gradually, growth ceases, repair mechanisms age, and we become old.
Our Darwinian “warranty” expires. We are left with an aging body, unimportant to evolution. We are long on experience and short on future. But we still have a marvelous metabolism at our disposal, depending on our lifestyle. There are a number of metabolic pathways which affect aging, 2 of which have been more studied.
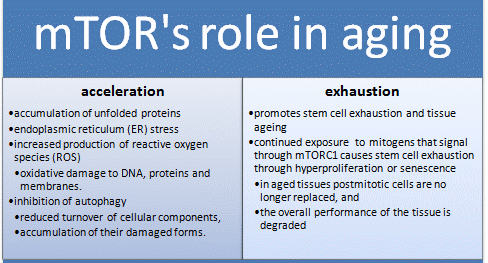
The mTOR pathway is most attuned to youth, senses nutrients and gears up for ANABOLISM, or growth. If you have not been careful to tailor your food intake to suit your decreasing requirements, your efficient metabolism stores it away for a rainy day, around your belly and in your arteries, a bad effect from an essential mechanism. Antagonistic Pleiotropy is the name for a body mechanism that can be good for one function (or age) and bad for another.
The Sirtuin system is also important in aging, and has a variety of housekeeping functions, including mitochondrial maintenance. It is activated by exercise. The cells of our bodies change with aging. In old tissues, there are less stem cells and other young, functional units. There are more damaged, dysfunctional “zombie” cells that don’t do much but promote inflammation, and hence more inflammatory cells accumulate.
Controlling the mTOR System and promoting the sirtuins help increase apoptosis and get rid of dysfunctional cells, including cancer. DOCTORS SHOULD PRESCRIBE EXERCISE, as well as SLEEP AND DIET, like they do medicine, and maybe we wouldn’t need so many pills. We might also feel better into old age.
Migraine Headache in its classic form is a unique syndrome, or grouping of symptoms. There is often a PRODROME of anxiety, mood changes or fatigue a day or two before the Headache. There may also be an AURA, such as visual or other sensory symptoms, preceding the headache by minutes.
The Headache is often ONE-SIDED (hence the name, HeMigraine). The Headache is SEVERE, and accompanied by NAUSEA AND VOMITING, a “sick” Headache.
There are a variety of TRIGGERS, such as ripened Cheeses, Red wine, Nitrate-containing foods like hot dogs and pepperoni, and missing your cup of coffee. Stress and Hormonal Changes (menstrual periods) may trigger Migraine.
Migraine often has a FAMILY HISTORY. If one parent has migraine, the risk is 50%, and if both parents, 75%. It is more common in women. During the Headache, Migraine sufferers often seek out a quiet, dark room, and avoid stimulation.
My own experience with Migraine is with isolated OPHTHALMIC MIGRAINE. I have the aura, but luckily have no pain. In my day, 50 years ago, Migraine was considered a Vascular Headache Problem, with Vasodilation being the cause. Many triggers result in Vasodilation.
After a half century of intense study, including the discovery of Calcitonin Gene Related Product (CGRP) in the blood during Migraine, It is now considered a NEUROVASCULAR Headache Problem, and there is optimism for future progress.
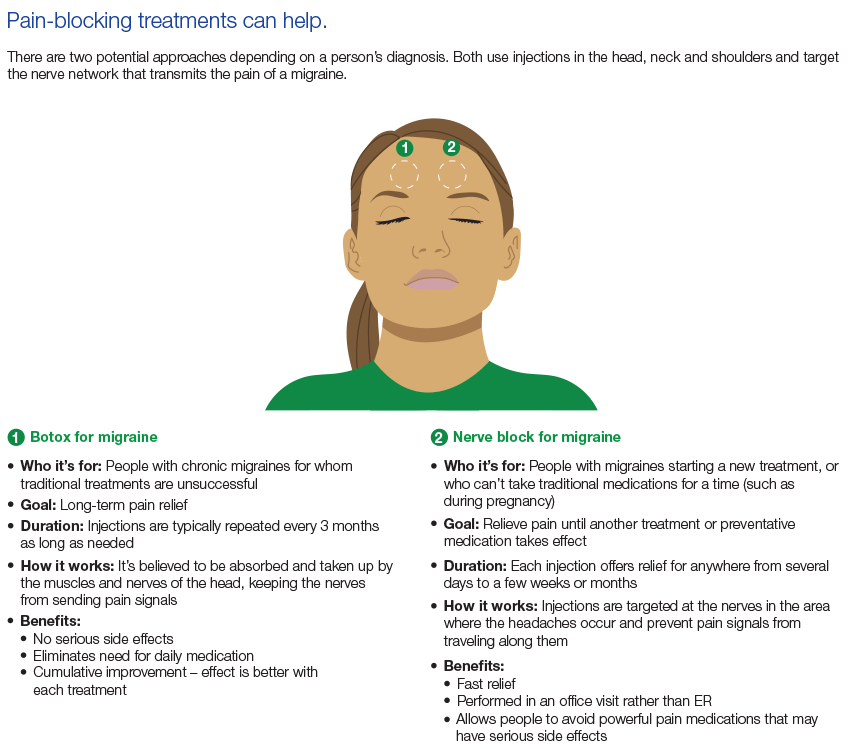
TREATMENT can be to abort, to shorten the attack after the warning Prodrome or Aura start. If the attacks are too frequent, such as several times a week,
PREVENTATIVE treatment may be needed. Medications include a host of chemicals, including Hormones, and most recently, CGRP. Many of these chemicals are vasoconstrictors, which narrow blood vessels.
The number of older people, including those living with dementia, is rising, as younger age mortality declines. However, the age-specific incidence of dementia has fallen in many countries, probably because of improvements in education, nutrition, health care, and lifestyle changes.
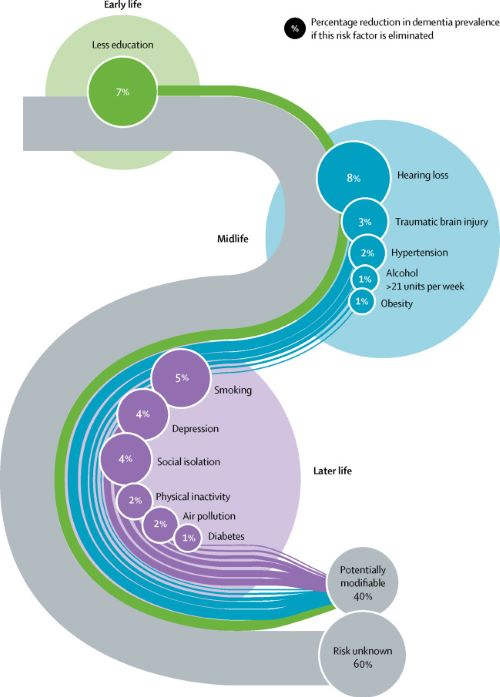
Overall, a growing body of evidence supports the nine potentially modifiable risk factors for dementia modelled by the 2017 Lancet Commission on dementia prevention, intervention, and care: less education, hypertension, hearing impairment, smoking, obesity, depression, physical inactivity, diabetes, and low social contact.
We now add three more risk factors for dementia with newer, convincing evidence. These factors are excessive alcohol consumption, traumatic brain injury, and air pollution. We have completed new reviews and meta-analyses and incorporated these into an updated 12 risk factor life-course model of dementia prevention. Together the 12 modifiable risk factors account for around 40% of worldwide dementias, which consequently could theoretically be prevented or delayed.
The potential for prevention is high and might be higher in low-income and middle-income countries (LMIC) where more dementias occur. Our new life-course model and evidence synthesis has paramount worldwide policy implications. It is never too early and never too late in the life course for dementia prevention. Early-life (younger than 45 years) risks, such as less education, affect cognitive reserve; midlife (45–65 years), and later-life (older than 65 years) risk factors influence reserve and triggering of neuropathological developments.
Culture, poverty, and inequality are key drivers of the need for change. Individuals who are most deprived need these changes the most and will derive the highest benefit.
Lancet’s 2017 Metanalysis mentions 9 Dementia risk factors. The 2020 Paper adds 3 additional factors. TRAUMATIC BRAIN INJURY, ALCOHOLISM, and AIR POLLUTION.
The inclusion of Trauma, with a 3% weighting, may be due to the increased awareness of TBE stemming from football injuries. The preventable 12 Factors are still in the minority. 60% of the factors are not preventable, since they are Genetically determined.
LESS EDUCATION, HEARING LOSS and SOCIAL ISOLATION, 3 of the original 9 factors,all lead to less brain stimulation, and can be unified under the idea of COGNITIVE RESERVE. If a person starts with less Cognition, it is reasonable to think he would be Demented sooner.
Together, less education, hearing loss, and social isolation account for almost Half of the correctable conditions. SMOKING is one of those things which impact almost every human disorder. It is amazing that cigarettes are still manufactured. In fact, their use is actually Increasing,especially the Far East, where they probably account for much of the escalating problem with Dementia in that region.
Our favorite causes, Sleep, Diet, and Exercise, apparently play only a minor role in Dementia. Sleep is completely dismissed in this report. The fact that both Sleeping less than the Ideal 7-8 hours, and more than that amount is thought to correlate with health problems is probably the main reason for the omission.
My own opinion is that people who are in poor health may need more sleep, and therefore sleep longer. My own sleep is interrupted 3-5 times per night, so it is not surprising that I need an hour extra to feel rested. Any less than 9-10 hours, and I need a nap, which in my opinion is a sign of insufficient nighttime sleep. Poor sleep may be a factor in metabolic syndrome, often leading to DIABETES, OBESITY, and HYPERTENSION, which are factors in Dementia, mentioned in the article as bit players.
PHYSICAL INACTIVITY is mentioned as a minor factor in Dementia, but exercise, studied as a treatment of dementia, was found to improve only strength. Diet is not mentioned, but does contribute to OBESITY, which is a minor factor. Dementia is a great emotional and economic burden, afflicting many otherwise happy families with misfortune.
The Lancet metanalysis is admirable. But don’t forget the healthy lifestyle emphasizing Sleep Diet and Exercise; and exercise includes cognitive exercise. Anything we can do to avoid dementia is worthwhile. –
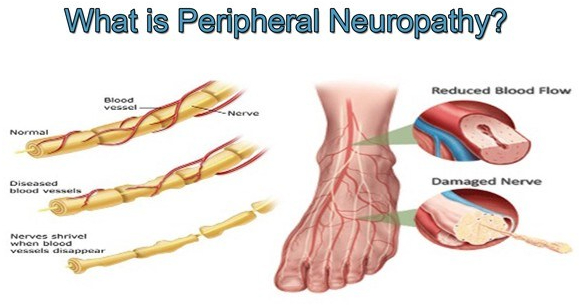
Peripheral Neuropathy is a common problem, and almost a quarter of the population will eventually suffer from it. It is very common in diabetes and metabolic syndrome, alcoholism, and in cancer therapy.
Even getting older is a risk; almost 10% of individuals 65 years old have some symptoms. There are more than 100 different types of peripheral neuropathy, and often it is just one feature of a primary illness.
Sometimes there is no known cause, such as in 2 of my older friends. I have a diminished vibratory sense in my feet, which causes me no noticeable problem. The longer nerves are more likely to be involved, except for the rare sensory ganglionopathy which is symptomatic of some cancers ( a “paraneoplastic disorder”) , some infections and autoimmune diseases.
When the sensory ganglia are involved, the numbness, tingling or pain can be more central, such as in the face or upper arm. There are 3 types of nerves that can be involved in peripheral neuropathy; Sensory, Motor and autonomic.
The sensory nerves deal with sensations, such as hot, cold, touch, pain, tingling, and numbness. Motor nerve involvement results in weakness or paralysis of an arm, leg or other area under Voluntary control. The autonomic nervous system coordinates activities beyond voluntary control, such as sweating, salivation, food propulsion and heart rate, which can be activated or inhibited.
The symptoms of neuropathy depend upon the type of nerve involved. Balance is a complex ability that can be disturbed by a lack of proper sensory nerve function (Position sense or proprioception) motor weakness, vision or coordination which involve higher centers.
The medical evaluation of peripheral neuropathy begins with a family practitioner or internist who does a detailed history, asking about such things as diet, medications, alcohol consumption, and injuries. Vitamin intake is important, but can be overdone.
Peripheral nerve symptoms can actually be caused by excessive B6, pyridoxine. The upper limit is 100 Mg.. A physical exam checks for weakness, sensory problems, reflexes and balance. Blood tests may reveal diabetic, kidney, liver, thyroid or immune problems problems.
A major disorder associated with neuropathy may be revealed and pursued. If nothing turns up, and the neuropathy is significant, referral may be needed to a neurologist, or other appropriate specialist. Many specialized tests and treatments may be needed.
Even with the best of care, a specific “cure” may not be found. Peripheral neuropathy can often be avoided by a healthy lifestyle.
Our Kidneys and Liver have a lot in common. They are not dramatic, take-care-of-me-now organs like our Hearts and Brain, but usually do their job quietly until they lose almost all of their function. They have lots of reserve; you can donate one of your kidneys or a piece of your liver and notice no change. They are both vital organs, and you will die without them.
Since they both help clear wastes and toxins from the bloodstream and produce hormones, they SHARE SYMPTOMS such as nausea, vomiting, fatigue, and mental changes.Their performance can be checked by blood tests. Healthy habits will protect their -and your- survival.
Certain Drugs impair their operation. They are both composed of many identical functional units, the nephron in the kidney, and the hepatic lobule in the liver.
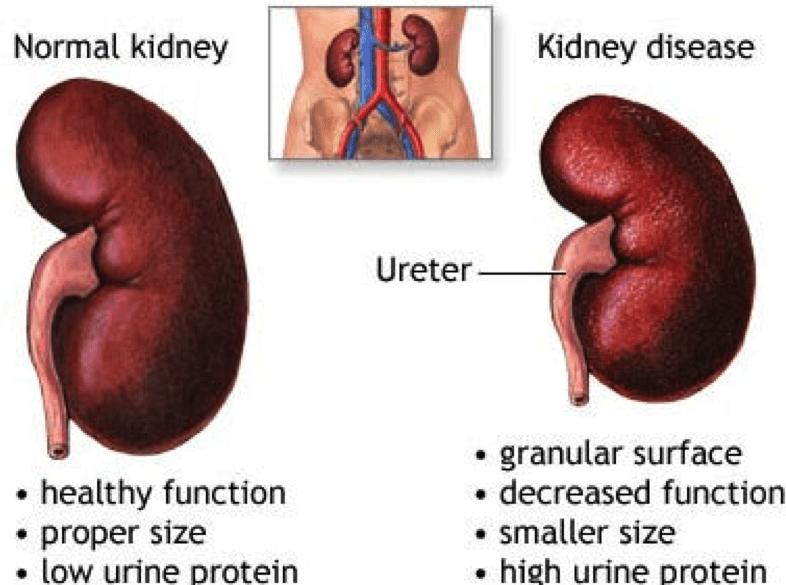
The GLOMERULUS of the Nephron is a tuft or ball of capillaries and associated kidney cells that allow the fluid and dissolved molecules of the blood to come through, while restraining the larger proteins and cells of the blood, keeping them in the vascular system. The smaller molecules of sodium, potassium, urea and other waste products leak through the glomerulus.
This filtered liquid travels through the long, folded kidney tubules, where the RIGHT AMOUNT of salt and water are REABSORBED. This keeps the vascular fluids, the internal environment, the MILIEU INTERIOR, perfectly well adjusted for proper cell function. It is when the chemical environment of the body falls out of adjustment, when the kidneys FAIL to do their job, that the cells of the body cannot function properly, and Symptoms-fatigue, lethargy etc. – develop.
BLOOD PRESSURE is intimately involved with the KIDNEYS, which has an Endocrine function. The Renin( Renal=kidneys) Angiotensin system is a major regulator of blood pressure.
You may have heard of the ACE-2 receptor as the binding site of th COVID Virus. This Angiotensin Converting Enzyme receptor is on the surface of cells all over the body and normally functions to control blood pressure.
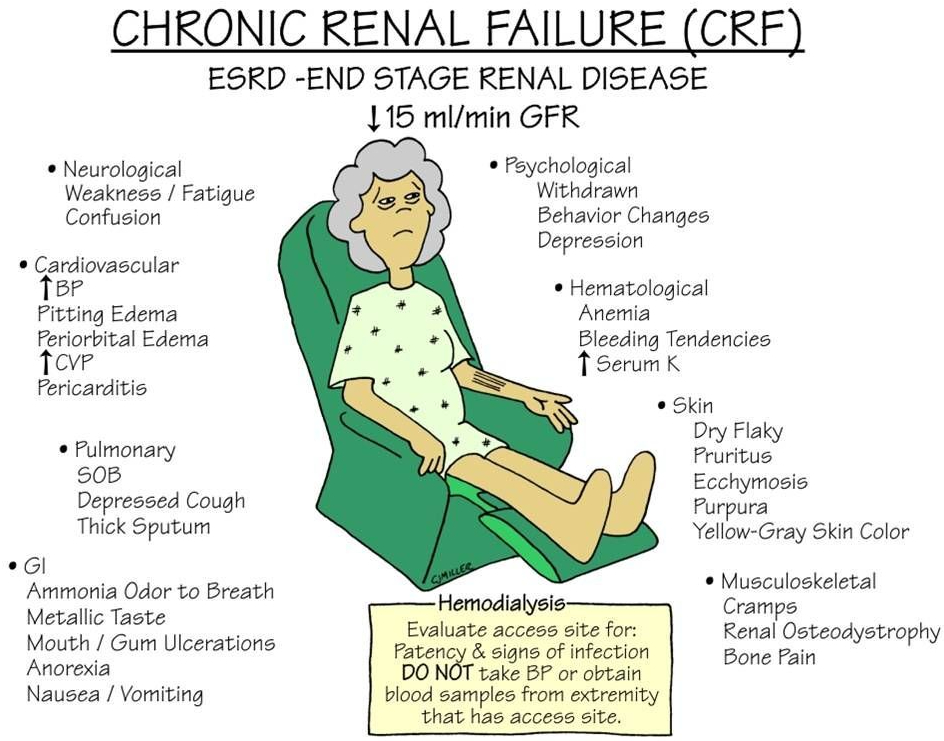
DIABETES is the most common cause of end stage renal disease (ESRD), bringing our healthy triad of SLEEP DIET and EXERCISE to our attention once again.
POLYCYSTIC KIDNEY DISEASE is an inherited condition where many nephrons fail to hook up to the urine collecting system, and the fluid builds up into cysts, which then eventually replace the rest of the kidney. Pressure from urine blockage by an enlarged prostate, or even lack of ureteral valves can also back up into the kidneys and eventually cause ESRD.
Infections and autoimmune diseases can result in ESRD. Treatment of ESRD is usually a Kidney transplant or Dialysis. There is a waiting list for the former and the latter is life-altering. You can’t beat a healthy lifestyle.
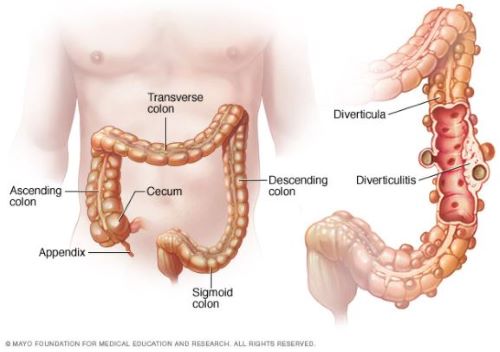
Your large bowel, or colon, is at the end of the Gastrointestinal tract. It starts on the right side of your abdomen, where the small intestine empties into the caecum. This is also where the Appendix bulges down, looking like a little finger coming from the caecum. The 5 foot long large intestine is the final processing area of your food, after the nutrients have been absorbed.
The Colon contains virtually all of the microbiome, reduces the volume of the fecal matter, and propels it to its final destination. The propelling muscles are an inner circular ring, and 3 outer longitudinal strips. These outer strips of muscle do not completely encircle the Colon, allowing for protuberances of lining membrane and circular muscle to balloon out into prominences called Taenia.
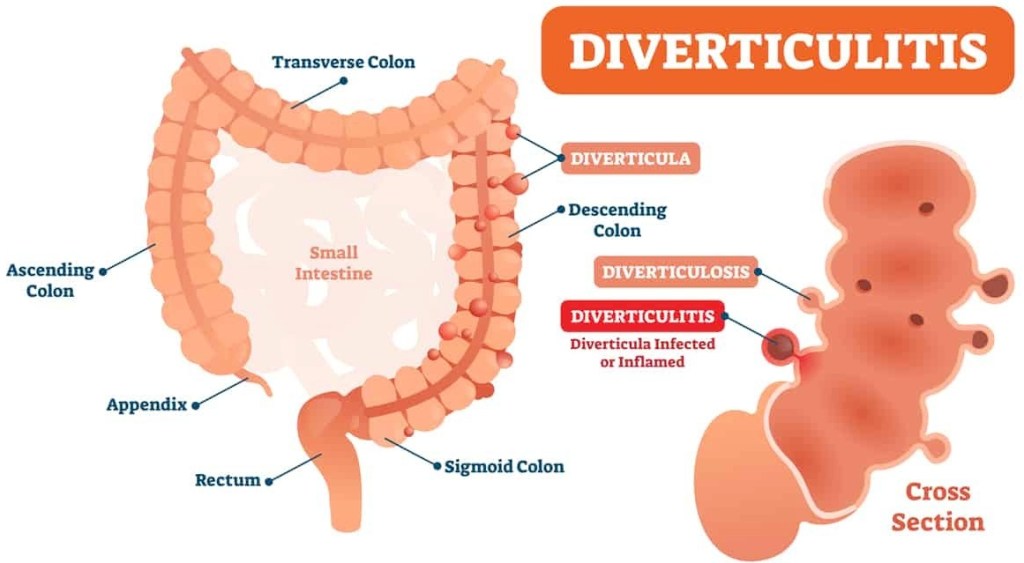
It is in these weakened areas, especially where blood vessels penetrate that little herniations form over the years. Diverticulosis occurs in 50% of people more than 60 years of age, and in almost everybody more than 80 years.
Diverticulosis is a condition where pressures up to 120 mm or mercury, generated by the colonic muscles gradually push out little pouches of lining membrane called diverticula. Nobody knows why some people get an INFLAMMED diverticulum.
Age, of course, is a factor, as are Obesity, diabetes, smoking and poor diet; a tendency toward inflammation is common in all of these risk factors. Comparing diverticulitis with Appendicitis is an interesting exercise. The symptoms are mirror images of each other. Appendicitis occurs on the right side.
Diverticulitis usually occurs on the left side, except in asian people. The asian DIET seems to favor diverticula on the right side. When asians immigrate to the U.S. and start eating more Red meat and fewer vegetables, the diverticula shift to the left side.
Signs of Diverticulitis include gastrointestinal symptoms, such as pain, tenderness,nausea, cramps, constipation, and Fever. Rectal bleeding can sometimes occur. Treatment includes antibiotics.
If the condition worsens, serious complications, such as abcess may develop and require surgery. As usual, Prevention, including diet and exercise, is better than Treatment. A HIGH FIBER DIET is the best prevention.
–Dr. C.
Article #1 to read – Diverticular disease of the colon: New perspectives in symptom development and treatment
Article #2 to read – Management of Colonic Diverticulitis | Effective Health Care Program
Empowering Patients Through Education And Telemedicine