

INFOGRAPHIC: 7 WAYS TO REDUCE STRESS (HARVARD)

When not walking barefoot at night or on the beach, my toes have been squeezed together most of my life. Closed-toe compression stockings for my varicose veins plus inadequate space at the front of my shoes have encouraged my big toe to “scissor” and to cross over the second toe. At that point I started wearing open-toe stockings, and tried to give my toes more room in larger shoes. I also used a spacer to push the big toe out.
Walking on the beach is a wonderful place to free up your toes. For a while, I walked in the deep sand at the top of the beach, trying to get more exercise. Periodically I would get some thorns in my feet, and go to podiatrist to get them out.
During one visit, the podiatrist told me that I was getting a hammer toe in the toe right next to my big toe, and I now use a little ring shaped cushion for that second toe, incorporated with a spacer.
It is amazing how little we use the musculature of our feet, and how surprisingly well they hold up. People that are really in good athletic shape stress flexibility as being very important, and athletes often do stretching exercises before they do their workout. Practically anything that will stretch a joint is helpful, such as flexing, extending, and spreading the toes, plus flexing and extending the foot.
You can overdo it, however, as I have learned to my discomfort. You must do any exercise within the limitations of your body, beginning slowly, and working up to your desired level.
My big toe has almost no flexibility, and the joint that attaches it to the foot is enlarged and pretty fixed. I am very careful how much range and pressure I use .Even something as simple as stretching the Achilles tendon can be a problem if you do too much of it all at once. Always work slowly into your exercises to make sure that you do no harm.
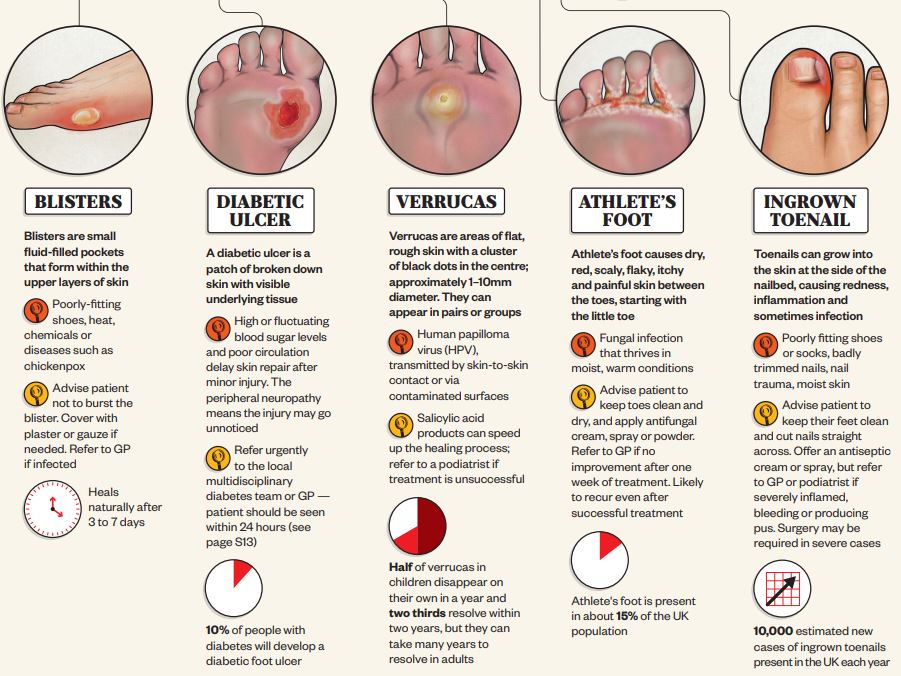
Ingrown toenails have also bothered me from time to time. I very carefully try to trim them back and avoid breaking the skin; the foot is easily infected, particularly among diabetics and older people. A podiatrist is very helpful if you let things go too far.
My toenails, particularly on my big toe, are getting white and thick with a nail fungus. This can be treated with an oral medication, dispensed by a doctor or a podiatrist. I have chosen to keep it in check with clotrimazole cream, and that seems to be working. I worry from time to time about creating a resistance factor in the fungus, but they are very slow growing, and not likely to develop a mutation.
If you would like further discussion on foot exercises, please check the following reference, one of many on the Internet.
A weekly podcast on the latest medical, science and telehealth news.
In a very good article, the Journal ‘Science’ has collated a lot of basic science regarding aerosol transmissions in viral infection generally, and Covid-19 in particular.
Early in the epidemic, I thought that large droplet transmission, which fell to the floor, and was transmitted by fomites and hand autoinoculation into the respiratory membranes, was more important. The main thesis of the article is that it is not large droplets, but aerosol particles that mainly transmit.
The secondary assertion is that aerosols can be up to 100 µm microns in diameter and still be transmitted by inhalation. they also stated that particle size of equal or less than 5 µm contain more virus particles than all the larger particles put together in spite of the greater mass of the larger particles . Normal speaking creates about 1000 aerosol particles per minute, And normal breathing about 7200 aerosol particles per liter of exhaled air. Coughing is more sporadic and tends to produce the larger droplets which don’t stay airborne as long, but I wouldn’t count on it.
There is a tremendous difference between individuals as to the number of particles they generate. It’s estimated that 10 to 20% of individuals account for 80 to 90% of the virus.
Slide number two deals with viral load and infectivity which is a function of the pH value, electrical charge, and other characteristics of the virus. An important point is that even though there is lots of viral RNA, that doesn’t mean that the virus is infective. Once again there’s a tremendous difference between the infective viable virus content of the aerosols from infected patient to patient. He stated that in one room with two Covid patients, they were 6 to 74 TCID/50 per liter, which means you’re almost certain to be infected if you don’t have a mask that filters out the virus, or some kind of purification in the room.
Slide Three was very interesting to me. The persistence in hours graphed against the aerosol particles size. 100 µm particles stay in the air only about five seconds, 5 µm particles stay in the air for 30 minutes, and one micrometer particles will stay in the air for 12 hours or more.
The fourth slide talks about factors affecting the distribution of indoor aerosols. There may be certain parts of the room where the particles congregate , depending on the ventilation type, whether natural, mechanical or filtered, flow patterns within the room, and indoor filtration and killing devices such as ultraviolet light.
Mention is made of the CO2 level in the room as a measure of air circulation. There is a higher CO2 in the air with lots of people and poor ventilation. The recommendation is that 7-8 ppm is about the highest acceptable level, and the possibility of using a portable HEPA filter would not be a bad idea for people frequenting indoor restaurants. Of course, outdoor air with its breezes, dispersion, less humidity, higher ultraviolet and usually Greater dispersion of people is preferable to indoor contact.
Some other interesting points are that children produce less aerosol particles because they have a smaller number of bronchi. I thought the bacteria were less likely to be aerosol transmitted than viruses, but they state that the R0 of tuberculosis can be as high as 4.3, vs. 7-8 for covid. The typical tuberculosis bacillus is relatively large, and yet is only 2 µm in length, well within the size of an aerosol particle.
Osteoarthritis is a “wear-and-tear” form of arthritis. Over time, the protective tissue at the ends of the bones wears down, so simple tasks like standing up or taking the stairs becomes painful. Orthopedic surgeon James Browne, MD, discusses the causes of the disease, and the many treatment options available at UVA.
Find out more at: https://uvahealth.com/services/joint-..
There are many types of cells in the human body, and any of them can mutate, and become cancerous. Cells of The immune system are no exception, ironically, even though their one of their jobs is to fight cancer.
The plasma cell is an immune system cell that develops from lymphocytes(B-cells) and specializes in producing “Gamma Globulins”, a type of antibody.
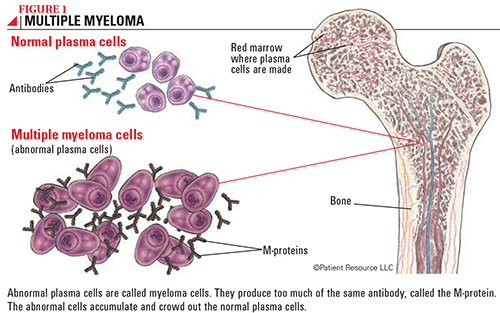
When cancer involves plasma cells In the bone marrow it tends to crowd out the other cells. This can produce bone pain and anemia.
All of the cancer cells come from a single progenitor cell and form a “clone”. This clone produces a large amount of defective protein that would normally be combined with other proteins into the making of antibodies. The large amount of the same protein can often be detected in the urine, as a “Bence Jones” protein.
In modern terminology, the condition is called a “monoclonal gammopathy”. This mass of protein gets into the bloodstream, and can deposit in various tissues, where it is called “amyloidosis”. The kidneys are often damaged in the process of excreting the overproduced, repetitious chains of useless protein.
I had a friend who was a pilot in the military during the Vietnam war. He was around “agent orange”, which was on the news a lot in the 80’s. Agent orange was contaminated by a toxic chemical called Dioxin, which is known to cause cancer. My friend developed a cancer, primary amyloidosis, which is a close relative of multiple myeloma, and in his case produces what is called light chains.
His first warning was an elevated creatinine on a metabolic panel blood test, which pointed to the kidneys. Medical investigation uncovered his plasma cell cancer, and he began treatment. His kidneys eventually started to fail.
His daughter donated one of her kidneys, and currently he’s doing well, since medical treatment curtailed the light chain production.
Please refer to the accompanying Cancer association article on multiple myeloma.
A Mayo clinic article was posted on DWWR on May 25, 2021.
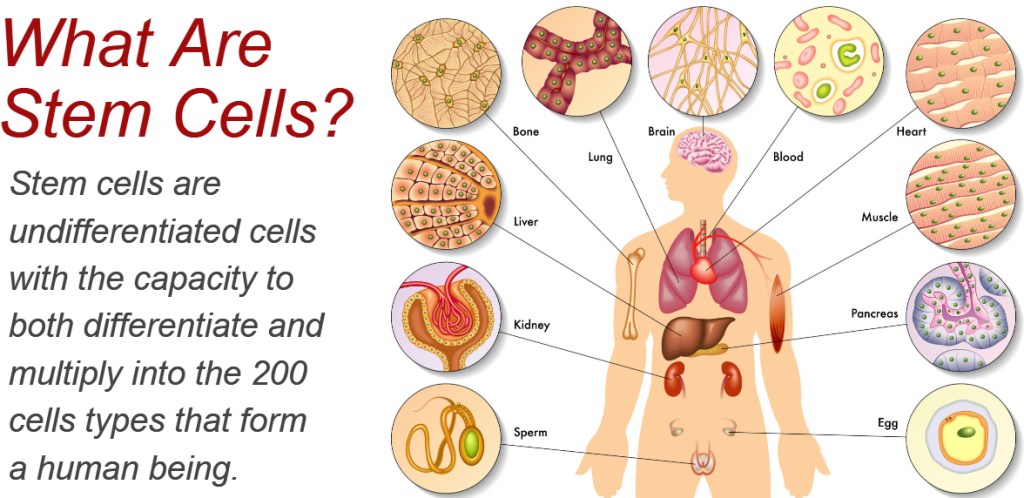
The ultimate stem cell is the fertilized egg from which we came. This omnipotent stem cell divides countless times, “differentiates”, and forms more and more specialized tissues, and our body is the eventual result. All of our tissues contain some stem cells, which grow increasingly rare as we age.
Regenerative medicine takes advantage of stem cells derived from diverse sources. An embryo, an umbilical cord, or your bone marrow contains stem cells. Even one of your mature connective tissue cells that has been dedifferentiated, or sent back along the pathway that originated from the single cell from which you came, can be induced to form a stem cell (iSC).
If the stem cell originates from your own tissues, it is accepted by your body, as one of its own.
I have an wealthy acquaintance whose Parkinson’s disease is being treated by one of his own cells induced to form a dopamine containing neuronal stem cell.
The article posted previously regarding rotator cuff surgery apparently used stem cells to shorten the recovery time.
I have heard about the use of stem cells in heart failure, osteoarthritis, and other joint problems, and I’m sure we will hear about this increasingly as time passes. However, there are hurdles to be overcome, moral, legal and medical. The possibility (small) of induced stem cells to evolve into cancer is one medical hurdle, and if the Stem Sell originates from another individual, immunosuppressive treatment must be used in the recipient to allow the stem cells to work. Also, the use of the other individual’s stem cells may involve some moral, legal and possibly religious objections.
Please refer to the following Mayo clinic article for more information.
In the video above, Alexander Stockton, a producer on the Opinion Video team, explores two of the main reasons the number of Covid cases is soaring once again in the United States: vaccine hesitancy and refusal.
“It’s hard to watch the pandemic drag on as Americans refuse the vaccine in the name of freedom,” he says. Seeking understanding, Mr. Stockton travels to Mountain Home, Ark., in the Ozarks, a region with galloping contagion and — not unrelated — abysmal vaccination rates. He finds that a range of feelings and beliefs underpins the low rates — including fear, skepticism and a libertarian strain of defiance.
This doubt even extends to the staff at a regional hospital, where about half of the medical personnel are not vaccinated — even while the intensive care unit is crowded with unvaccinated Covid patients fighting for their lives. Mountain Home — like the United States as a whole — is caught in a tug of war between private liberty and public health. But Mr. Stockton suggests that unless government upholds its duty to protect Americans, keeping the common good in mind, this may be a battle with no end.
I am a Doctor Who has studied the miracle of MRNA Covid vaccine, and who knows that it cannot get into the nucleus of any of my cells or long remain in my body.
I have studied the transmission and pathogenesis of Covid, and know how it works. The knowledge that it could affect my thinking, memory, my very essence, and the fact that it could last indefinitely after the initial illness has certainly made me a believer.
There is an element of truth in the concerns of anti-vaxers and anti-maskers. Unfortunately the problem is not black and white. No vaccine is 100% safe, although the mRNA vaccines come close. There is some worry about clotting problems with a few people, particularly the young. This risk is measured in terms of problems per million people getting the vaccine, and is vanishingly small compared to the alternative of exposing yourself to the ravages of Covid.
An intelligent friend of mine who is a nurse has auto immune disease, and vaccines tend to hit her hard. Unfortunately the fact that she is a nurse and is exposed a lot to the public make her more likely to get Covid, and her auto immunity would render her much more likely to have complications, should she get it. She has received her first injection of Covid vaccine, and had a lot of fatigue, headaches and symptoms that were relatively self-limited.
Masks are mainly useful in protecting other people from the mask-wearer and only slightly helpful in protecting the mask wearer from other people. Also, I have read a long article about some subtle disadvantages of forcing children to wear masks although I think it’s still a good idea, particularly when Covid is common in the community.
The main problem is that Americans have freedom of choice without the knowledge to weigh the benefits and hazards of receiving the vaccine, versus the hazards of getting the disease.
There are times when we should unload the making of such statistical decisions on people who know more about the vagaries of disease.
In my opinion, the states which allow hospitals to require their healthcare workers to receive vaccination, and allow schools to require their students and teachers to receive vaccination are in the right. Currently, there are less problems in those states.
Covid is certainly a nasty disease, and even doubly vaccinated people can be spreaders. As an elderly vaccinated person, I still treat everybody as if they are infected, and require masks when visitors come. When inside, I sit by an open door, with a fan behind me blowing air in the other direction.
At the age of 89, I cannot afford to get Covid-19.
Total knee replacement(arthroplasty) is one of the most successful orthopedic operations. Satisfaction rate varies between 75 and 90%. Even so, almost 10% of operated individuals will have anterior knee pain, the most common complication, 1 year after TKR.
I had an even greater appreciation of the knee after reading the following article, which explain the causes of knee pain more adequately than I can, and would be good to read.
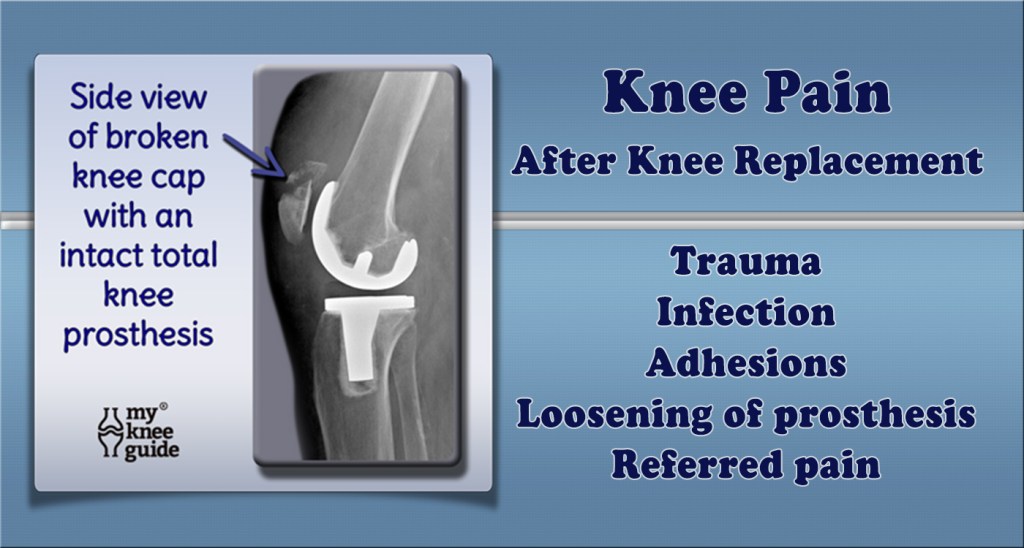
With knee replacement surgery, a great deal depends on the technical expertise and precision of the operating surgeon. A rotational error more than a degree or two can be critical, so important is proper tracking of the kneecap in the trochlea, or groove in the leg bone(femur). An imbalance in the pull of muscles, or a knock knee, (Valgus) angulation of the knee, hip rotation, spinal problems, all can be important in generating pain as you get older.
There are psychological factors too. The knee pain after TKR average is only 1/3 of that suffered before the operation, on average. However if you expect that discomfort will disappear completely, or if your pain threshold is low, or if you have anxiety or depression, you may have more postoperative pain, and be disappointed with the surgery.
My immediate reason to write this article was the anterior knee pain developing in a friend of mine, 15 years after surgery, at the age of 89. She had polio in childhood, and her right leg was severely affected. This caused her to overuse her left leg, resulting in a TKR 15 years ago. Just recently, she started developing anterior knee pain in the left knee. A thallium scan showed a lot of signal on the inside of the kneecap, most likely indicative of inflammation. She is not enthused about having another operation because of her age., and wondered about other things she might do.
An orthopedic friend of mine suggested that injections of a viscous lubricant might help, if the initial operation did not include resurfacing of the kneecap (patella). I would imagine that eventually the resurfacing of the patella with advanced materials, or perhaps stem cells might help.
I also thought of a special brace with a motor assist for her right leg, but the orthopedist said that this did not work very well in polio patients, who have a weak nerve signal.
Although my friends polio made her TKR almost inevitable, there are things that you can do, or avoid doing, that could help avoid TKR. Activities to reduce include squatting, deep lunging, running (particularly in deep sand), high impact sports, repetitive jumping, and running up stairs. Basketball, football, and volleyball come to mind as regular sports that are risky. Maintaining a healthy weight, controlling blood sugar, stoppage of smoking, avoidance of injury, and regular exercise, particularly walking and swimming ,are things that might help.
Remember that your knees are your wheels and are jewels to protect as you get older.









