Total knee replacement(arthroplasty) is one of the most successful orthopedic operations. Satisfaction rate varies between 75 and 90%. Even so, almost 10% of operated individuals will have anterior knee pain, the most common complication, 1 year after TKR.
I had an even greater appreciation of the knee after reading the following article, which explain the causes of knee pain more adequately than I can, and would be good to read.
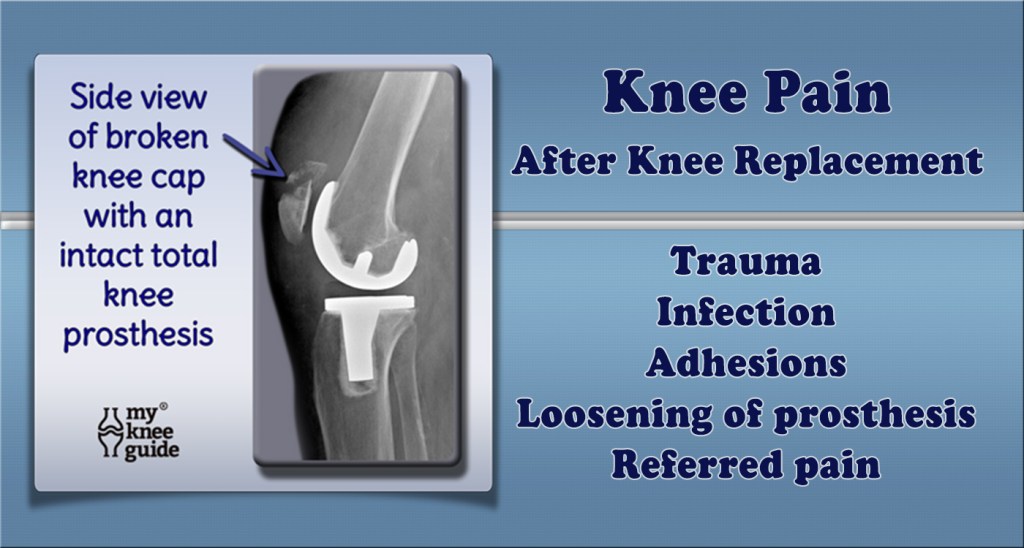
With knee replacement surgery, a great deal depends on the technical expertise and precision of the operating surgeon. A rotational error more than a degree or two can be critical, so important is proper tracking of the kneecap in the trochlea, or groove in the leg bone(femur). An imbalance in the pull of muscles, or a knock knee, (Valgus) angulation of the knee, hip rotation, spinal problems, all can be important in generating pain as you get older.
There are psychological factors too. The knee pain after TKR average is only 1/3 of that suffered before the operation, on average. However if you expect that discomfort will disappear completely, or if your pain threshold is low, or if you have anxiety or depression, you may have more postoperative pain, and be disappointed with the surgery.
My immediate reason to write this article was the anterior knee pain developing in a friend of mine, 15 years after surgery, at the age of 89. She had polio in childhood, and her right leg was severely affected. This caused her to overuse her left leg, resulting in a TKR 15 years ago. Just recently, she started developing anterior knee pain in the left knee. A thallium scan showed a lot of signal on the inside of the kneecap, most likely indicative of inflammation. She is not enthused about having another operation because of her age., and wondered about other things she might do.
An orthopedic friend of mine suggested that injections of a viscous lubricant might help, if the initial operation did not include resurfacing of the kneecap (patella). I would imagine that eventually the resurfacing of the patella with advanced materials, or perhaps stem cells might help.
I also thought of a special brace with a motor assist for her right leg, but the orthopedist said that this did not work very well in polio patients, who have a weak nerve signal.
Although my friends polio made her TKR almost inevitable, there are things that you can do, or avoid doing, that could help avoid TKR. Activities to reduce include squatting, deep lunging, running (particularly in deep sand), high impact sports, repetitive jumping, and running up stairs. Basketball, football, and volleyball come to mind as regular sports that are risky. Maintaining a healthy weight, controlling blood sugar, stoppage of smoking, avoidance of injury, and regular exercise, particularly walking and swimming ,are things that might help.
Remember that your knees are your wheels and are jewels to protect as you get older.