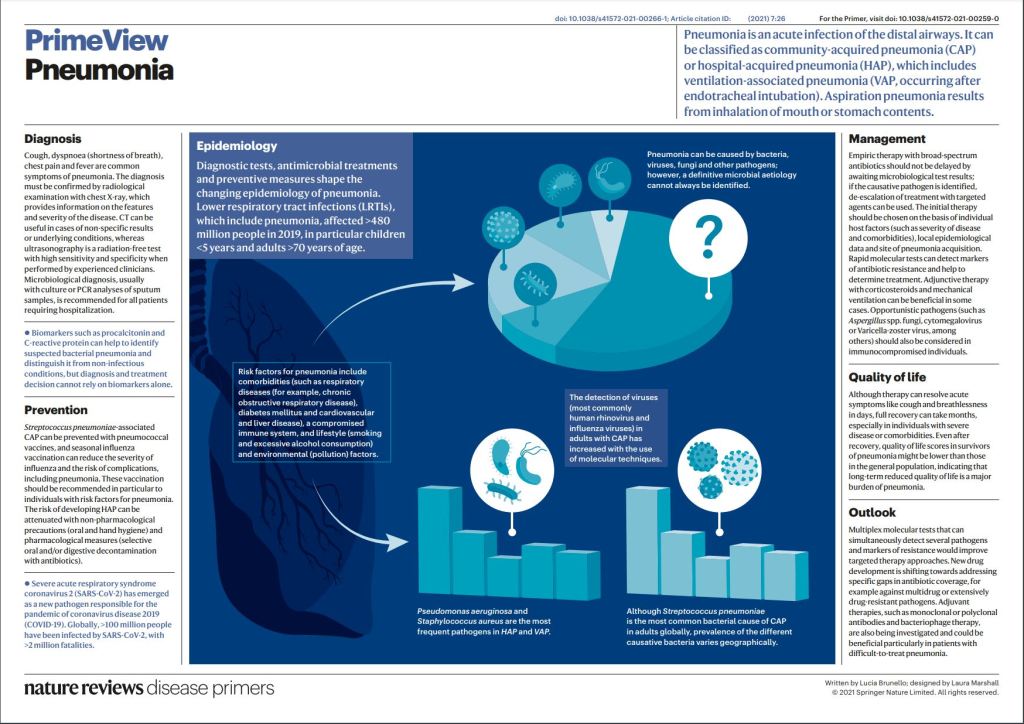
Pneumonia is a common acute respiratory infection that affects the alveoli and distal airways; it is a major health problem and associated with high morbidity and short-term and long-term mortality in all age groups worldwide. Pneumonia is broadly divided into community-acquired pneumonia or hospital-acquired pneumonia.
A large variety of microorganisms can cause pneumonia, including bacteria, respiratory viruses and fungi, and there are great geographical variations in their prevalence. Pneumonia occurs more commonly in susceptible individuals, including children of <5 years of age and older adults with prior chronic conditions. Development of the disease largely depends on the host immune response, with pathogen characteristics having a less prominent role. Individuals with pneumonia often present with respiratory and systemic symptoms, and diagnosis is based on both clinical presentation and radiological findings.
It is crucial to identify the causative pathogens, as delayed and inadequate antimicrobial therapy can lead to poor outcomes. New antibiotic and non-antibiotic therapies, in addition to rapid and accurate diagnostic tests that can detect pathogens and antibiotic resistance will improve the management of pneumonia.
Tuberculosis is an ancient killer, and is one of the few diseases that has been traced back to Ancient Egypt and beyond. TB has ravaged humanity for millennia, and was commonly called consumption due to its tendency to produce weight loss.
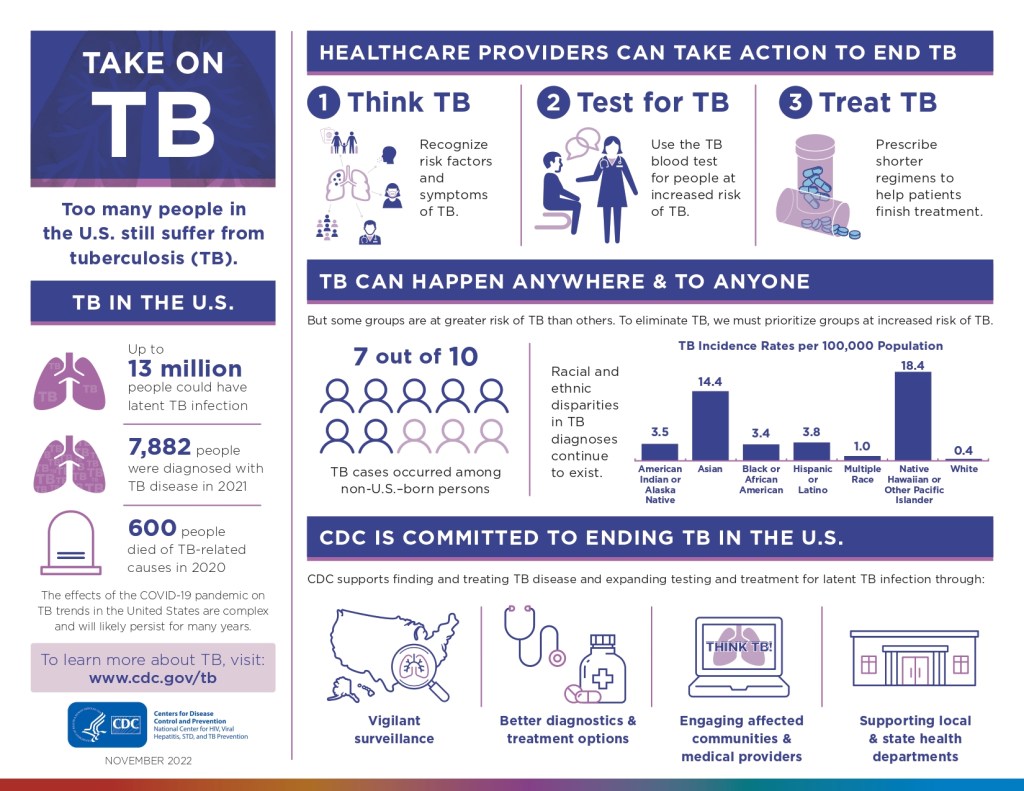
Once thought to be under control, TB has received a new lease on life with the emergence of AIDS. All countries except North America, western Europe, and Australia have a problem with tuberculosis, which kills more than 1 million people each year.
The tuberculosis germ is unusual in that It has a cell wall high in the lipid, mycolic acid. This protects the germ when it is engulfed by first responders such as macrophages. The infected cell Is surrounded by other macrophages, lymphocytes and Fibroblasts to form a granuloma. This creates a standoff, where the tuberculosis germ is still alive, but walled off, and becomes an inactive or “latent” case of tuberculosis, a small percentage of which become active each year.
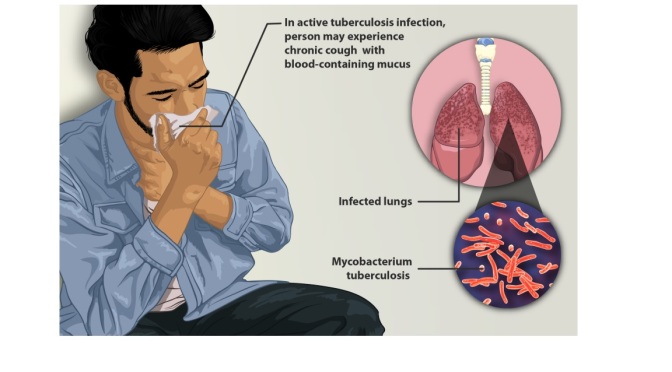
Active tuberculosis produces the usual infectious symptoms of fever, chills, and cough, often productive with blood. The tuberculosis germ multipliesu much more slowly than most other bacteria and the symptoms are long and drawn out; a cough lasting for more than a month, especially if accompanied by weight loss, should raise the suspicion of TB.
TB can spread to infect bones, kidneys, liver, and brain, but prefers the lung.
A spot on the Lung, confirmed by a Tuberculin test, or a blood test called a T-spot, will confirm the diagnosis.
The slow multipication of the tuberculosis Germ requires much longer treatment, and the combination with AIDS has caused a rapid development of resistant organisms. Fortunately, there are several drugs available.
Only one immunization is currently available, namely BCG. This has been used a lot in Europe and other countries . BCG produces a weekly positive tuberculin test.
A large number of conditions which reduce immunity, such as cigarette smoking, drug use, and immunosuppressive treatments associated with organ transplants and cancer will predispose a person to catching tuberculosis. TV is transmitted in the tiny droplets from sneezing, coughing, or talking such as we were accustomed to thinking about during Covid. The same preventative measures, such as masks and avoiding close contact with infected individuals should be practiced to prevent spread from an infected person.
If you follow a healthy lifestyle and are careful when traveling, you will most likely have no trouble with this nasty infection. Please check with the following reference or more complete information.
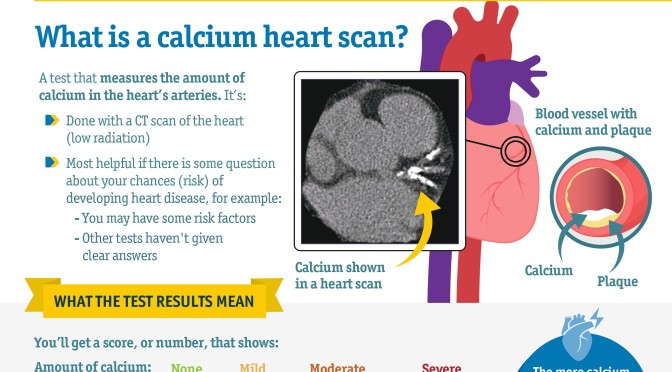
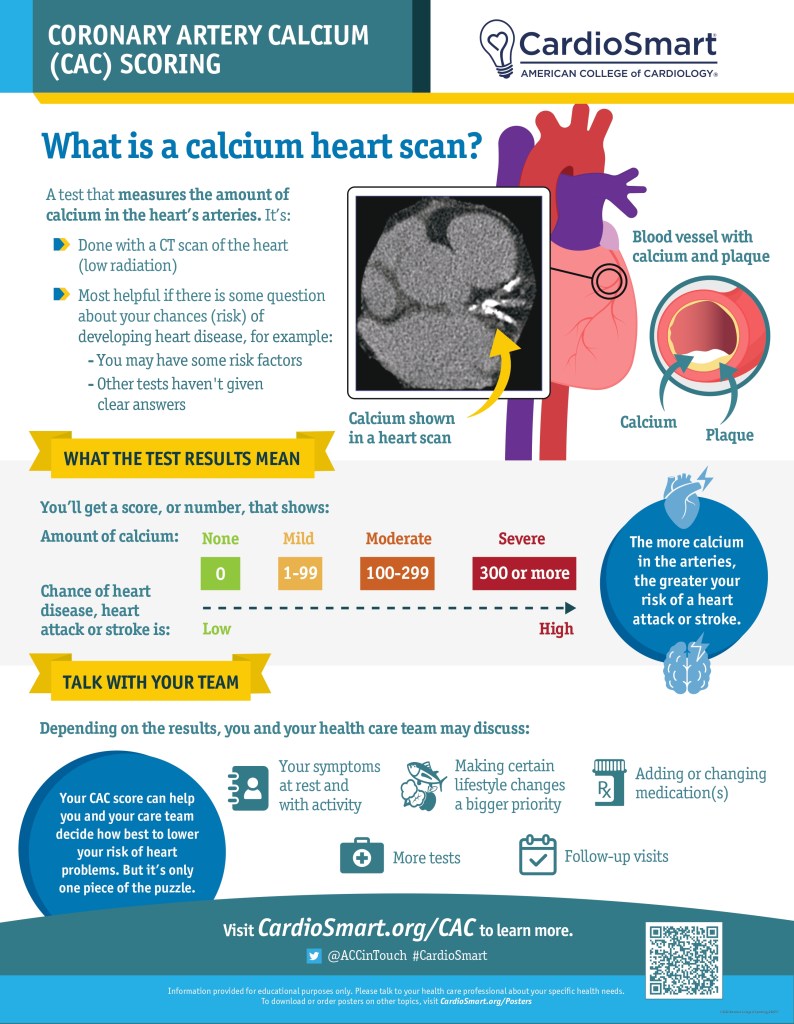
A CT scan of the heart measures the amount of calcium in the heart’s arteries. The more calcium in the arteries, the greater your risk of a heart attack or stroke.
Knowing your coronary artery calcium (CAC) score can help you and your care team decide how best to lower your risk of heart problems. But it’s only once piece of the puzzle.
If you’ve had a heart attack or stroke: Taking a low-dose aspirin a day is an important part of your treatment. It can help you prevent another heart attack or stroke.
If you haven’t had a heart attack or stroke: Taking an aspirin a day may prevent heart attack or stroke, but it can also cause bleeding. Talk with your health care team about the risks and benefits of aspirin for you. In general, don’t take a daily aspirin if you are 60 or older and don’t have heart disease.
The body is complicated! While organs in your body each have a specific job to do to keep you healthy, they still rely on each other to function well. When one organ isn’t working the way it should, it can put stress on other organs, causing them to stop working properly as well.
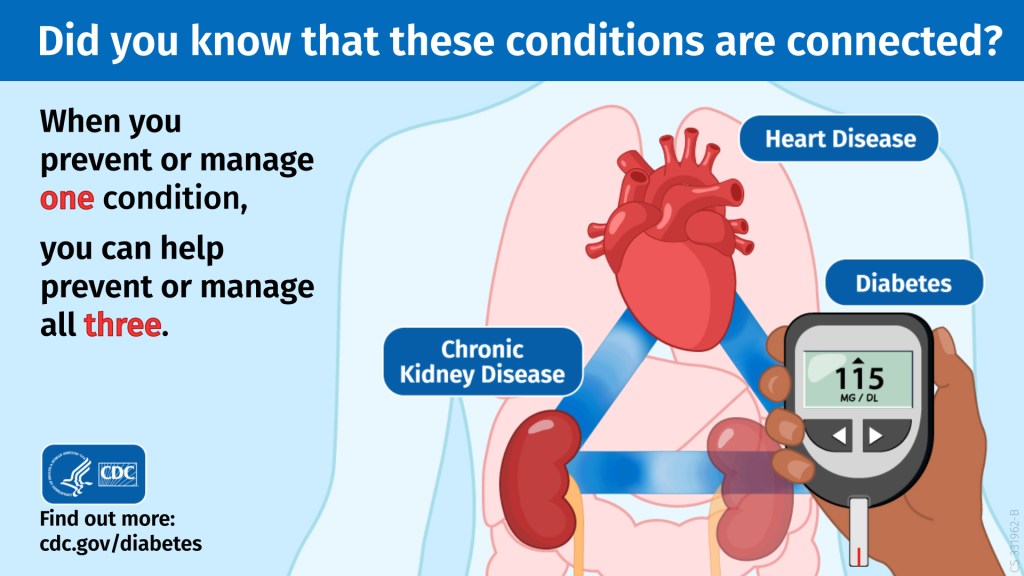
The relationship between chronic kidney disease (CKD), diabetes, and heart disease is one example of the ways our organs are connected.
The body uses a hormone called insulin to get blood sugar into the body’s cells to be used as energy. If someone has diabetes, their pancreas either doesn’t make enough insulin or can’t use the insulin it makes as well as it should.
If someone has CKD, their kidneys are not able to filter out toxins and waste from their blood as well as they should.
Heart disease refers to several types of heart conditions. The most common condition, coronary artery disease, leads to changes in blood flow to the heart, which can cause a heart attack.
Make the Connection
So how are these three conditions connected? Risk factors for each condition are similar and include high blood sugar, high blood pressure, family history, obesity, unhealthy diet, and physical inactivity.
High blood sugar can slowly damage the kidneys, and, over time, they can stop filtering blood as well as they should, leading to CKD. Approximately 1 in 3 adults with diabetes has CKD.
When the kidneys don’t work well, more stress is put on the heart. When someone has CKD, their heart needs to pump harder to get blood to the kidneys. This can lead to heart disease, the leading cause of death in the United States. Change in blood pressure is also a CKD complication that can lead to heart disease.
Luckily, preventing or managing one condition can help you prevent and manage the others and lower the risk for more complications.
A transient ischemic attack (TIA) is sometimes called a “mini-stroke.” It is different from the major types of stroke, because blood flow to the brain is blocked for only a short time—usually no more than 5 minutes.1
Ischemic stroke
Most strokes are ischemic strokes.2 An ischemic stroke occurs when blood clots or other particles block the blood vessels to the brain.
Fatty deposits called plaque can also cause blockages by building up in the blood vessels.
Hemorrhagic stroke
A hemorrhagic stroke happens when an artery in the brain leaks blood or ruptures (breaks open). The leaked blood puts too much pressure on brain cells, which damages them.
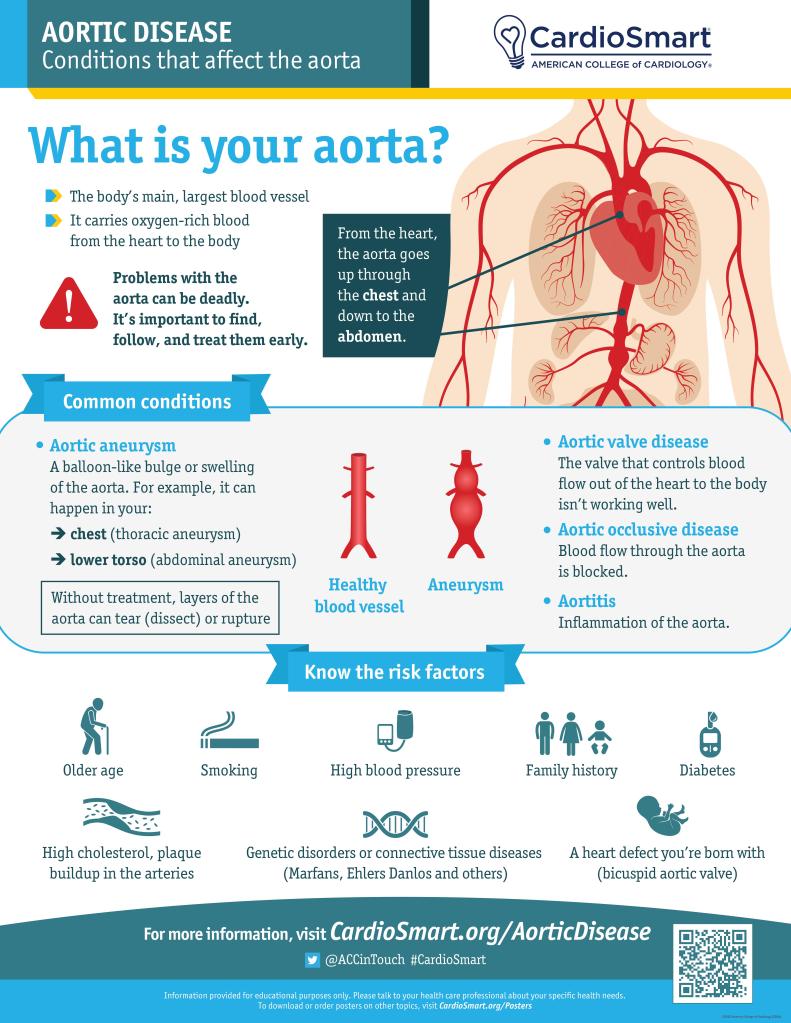
High blood pressure and aneurysms—balloon-like bulges in an artery that can stretch and burst—are examples of conditions that can cause a hemorrhagic stroke.
Transient ischemic attack (TIA or “mini-stroke”)
For Blanche Teal-Cruise, a smoker for 40 years who also had high blood pressure, the transient ischemic attack (sometimes called a mini-stroke) she had on the way to work was a wake-up call. Read Blanche’s story.
TIAs are sometimes known as “warning strokes.” It is important to know that
A TIA is a warning sign of a future stroke.
A TIA is a medical emergency, just like a major stroke.
Strokes and TIAs require emergency care. Call 9-1-1 right away if you feel signs of a stroke or see symptoms in someone around you.
There is no way to know in the beginning whether symptoms are from a TIA or from a major type of stroke.
Like ischemic strokes, blood clots often cause TIAs.
More than a third of people who have a TIA and don’t get treatment have a major stroke within 1 year. As many as 10% to 15% of people will have a major stroke within 3 months of a TIA.1
Recognizing and treating TIAs can lower the risk of a major stroke. If you have a TIA, your health care team can find the cause and take steps to prevent a major stroke.
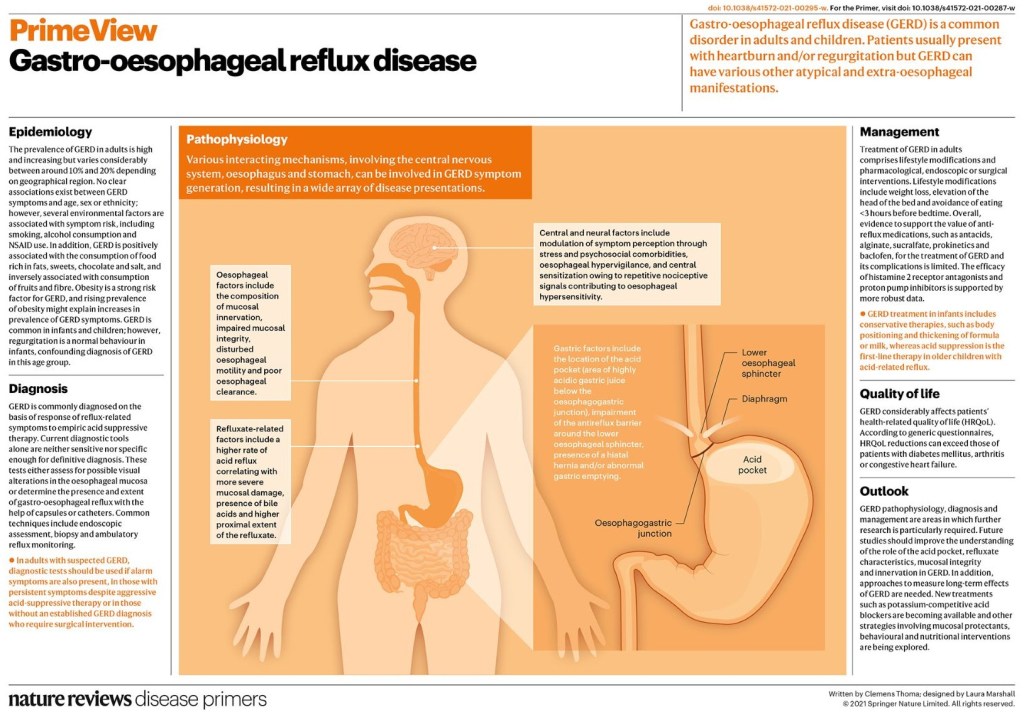
Gastro-oesophageal reflux disease (GERD) is a common disorder in adults and children. The global prevalence of GERD is high and increasing. Non-erosive reflux disease is the most common phenotype of GERD. Heartburn and regurgitation are considered classic symptoms but GERD may present with various atypical and extra-oesophageal manifestations. The pathophysiology of GERD is multifactorial and different mechanisms may result in GERD symptoms, including gastric composition and motility, anti-reflux barrier, refluxate characteristics, clearance mechanisms, mucosal integrity and symptom perception.
In clinical practice, the diagnosis of GERD is commonly established on the basis of response to anti-reflux treatment; however, a more accurate diagnosis requires testing that includes upper gastrointestinal tract endoscopy and reflux monitoring. New techniques and new reflux testing parameters help to better phenotype the condition. In children, the diagnosis of GERD is primarily based on history and physical examination and treatment vary with age.
Treatment in adults includes a combination of lifestyle modifications with pharmacological, endoscopic or surgical intervention. In refractory GERD, optimization of proton-pump inhibitor treatment should be attempted before a series of diagnostic tests to assess the patient’s phenotype.
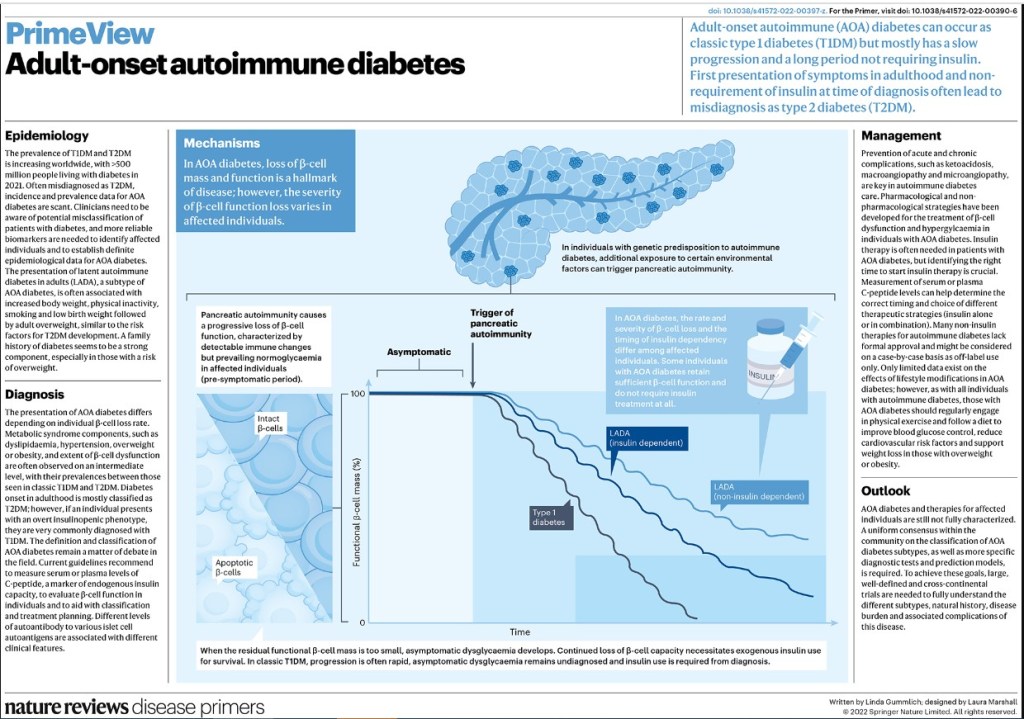
Adult-onset autoimmune diabetes encompasses a wide spectrum of heterogeneous genotypes and phenotypes, ranging from classic adult-onset type 1 diabetes mellitus to latent autoimmune diabetes in adults (LADA)
The heterogeneity of LADA arises from its definition as being present in any adult with diabetes who does not require insulin and who is positive for any islet autoantibody, regardless of titre, number or epitope specificity
The heterogeneity of LADA manifests in different clinical phenotypes, ranging from prevalent insulin resistance to prevalent insulin deficiency, each of which might be associated with different autoimmune and metabolic markers
Although patients with LADA are leaner and have healthier lipid and blood pressure profiles, evidence shows that there is no difference in cardiovascular outcomes between these patients and those with type 2 diabetes mellitus
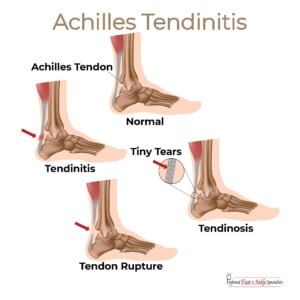
The Achilles tendon, or “heel cord”, connects your calf muscle to the heel. Overuse can inflame the tendon, or even tear or rupture it, causing a lot of pain.
Sudden increases in intensity of exercise can be a cause. It is more common in men, and as you get older. Running a lot in the soft sand of the beach has caused problems in many of my friends. Achilles tendinitis can be caused by certain antibiotics, such as fluoroquinolones.
Varying your type of exercise, or cross training, distributes the strain you put on your body and decreases the likelihood of Achilles tendinitis. Swimming comes to mind with any disturbance of your lower extremities. The pool in which I swim three days a week is disparagingly called the “injured reserve pool” in my community Stretching before exercising is always a good idea. Pick a routine and stick with it, particularly as you get older. If you have flat feet, getting a slight lift for the heel may help to take tension off the Heel cord, and orthotics may help. Getting expert advice is always advisable.
Prevention is always far better than treatment.
If a short period of rest doesn’t get rid of the pain, check with your Doctor, who might examine the tendon, take x-rays, or order ultrasounds to check the extent of the difficulty.