Mild cognitive impairment (MCI) is a condition in which people have more memory or thinking problems than other people their age. The symptoms of MCI are not as severe as those of Alzheimer’s disease or a related dementia. People with MCI can usually take care of themselves and carry out their normal daily activities.
People with MCI are at a greater risk of developing Alzheimer’s disease or a related dementia. Estimates vary as to how many people who have MCI will develop dementia. Roughly one to two out of 10 people age 65 or older with MCI are estimated to develop dementia over a one-year period. However, in many cases, the symptoms of MCI stay the same or even improve.
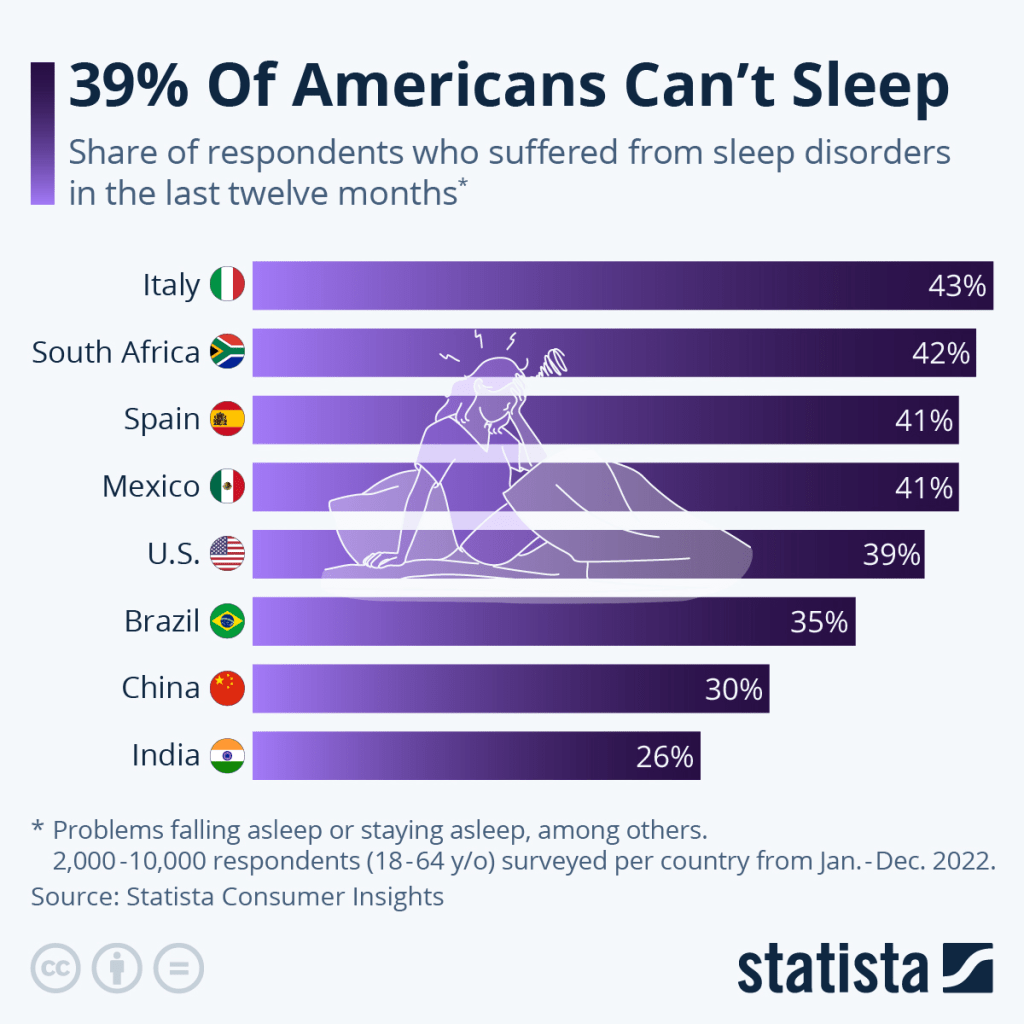
This Friday, March 17, is World Sleep Day, an annual event that aims to raise awareness of the importance of getting a good night’s sleep. This year’s campaign tagline is “Sleep is essential for health.” According to a study by the American College of Cardiology, up to 8 percent of deaths from any cause could be attributed to “poor sleep patterns”, while those with healthier sleep habits are less likely to die prematurely.
Data from Statista Consumer Insights shows that in the United States, 39 percent of respondents said they had suffered from a sleep disorder (problems falling asleep or staying asleep, insomnia, etc.) in the 12 months prior to the survey. Italians were among the worst sleepers in the survey at 48 percent reporting a sleep disorder, while India registered a higher share of good sleepers, with only 26 percent suffering from poor sleep.
“A psoriatic arthritis flare-up is a temporary worsening of symptoms of arthritis, which includes swelling, pain and stiffness in your joints,” explains Dr. Sapkota. “It can also include swelling of the whole toes or fingers due to the swelling of the ligaments around the joint. And sometimes, psoriasis, a skin rash, can worsen at the same time as your joints.”
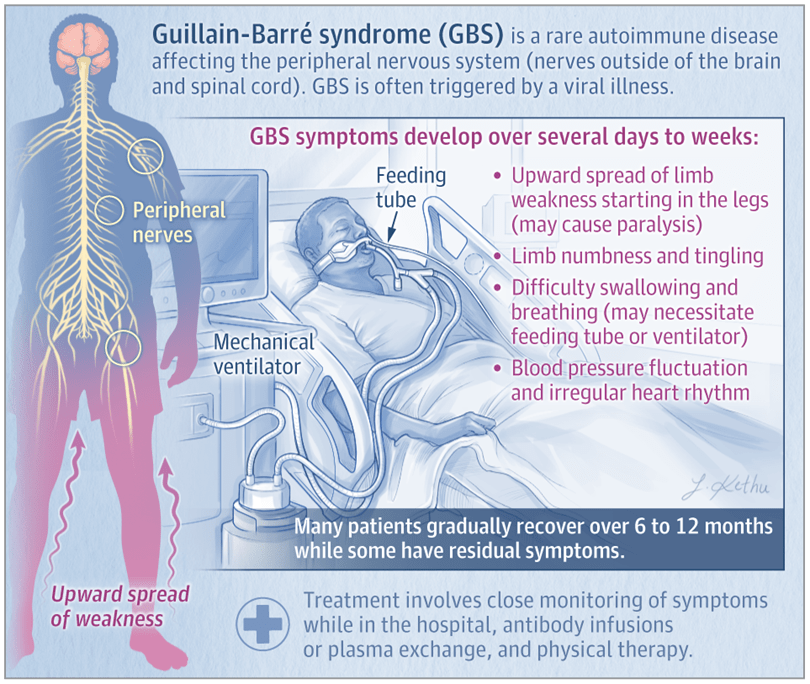
Guillain-Barré syndrome is an autoimmune disease that affects the nerves outside the brain and spinal cord (the peripheral nerves) and develops over several days to weeks. GBS can cause severe muscle weakness, and death occurs in about 5% of patients. The most common subtypes are acute inflammatory demyelinating polyradiculoneuropathy (AIDP) and acute motor axonal neuropathy (AMAN). Approximately 90% of people with GBS in North America and Europe have AIDP.
Signs and Symptoms of GBS
Patients with the AIDP subtype of GBS typically have weakness that starts in the legs and spreads to the arms, as well as decreased or absent reflexes. In more than 50% of these patients, nerves that originate in the brain stem (cranial nerves) are affected, which may cause facial weakness, difficulty swallowing, and eye muscle weakness or paralysis. Approximately 25% to 30% of patients develop severe weakness or paralysis of the muscles used to breathe. GBS commonly causes symptoms of low back pain and limb numbness and tingling, and fluctuations in blood pressure or an irregular heart rhythm can also occur.
Risk Factors and Conditions Associated With GBS
GBS affects people worldwide, and the lifetime risk of GBS is estimated at 1 in 1000. Although individuals of any age can develop GBS, the incidence increases with age, and males are slightly more likely to develop GBS than females.
Approximately two-thirds of patients have a diarrheal or respiratory illness within 4 to 6 weeks prior to the onset of GBS symptoms. Other, less common events or conditions that may trigger GBS include recent surgery, pregnancy, and immunosuppression. Although rare sporadic cases of GBS have been reported after vaccinations, the risk of developing postvaccination GBS is much lower than the risk of developing GBS after an infection.
Diagnosis and Treatment of GBS
Diagnosis of GBS is made based on symptoms and physical examination findings. Neurological testing often includes electromyography and nerve conduction studies to assess nerve and muscle function. Results of a spinal tap (lumbar puncture) may support the diagnosis of GBS and can rule out other neurological diseases.
Individuals with suspected GBS should be admitted to the hospital. All patients with GBS need close monitoring of their breathing, heart rate, and blood pressure. Individuals who develop severe respiratory muscle weakness or paralysis are supported with mechanical ventilation. Patients who have difficulty swallowing may receive nutrition through a feeding tube.
Current recommended treatments for GBS are intravenous immune globulin (IVIG), an infusion of antibodies, or plasma exchange, which involves removal and replacement of the liquid component of blood. About 40% to 50% of patients with GBS do not improve within 4 weeks after IVIG or plasma exchange and need prolonged supportive care. Physical, occupational, and speech therapy are important to help patients regain strength and function.
What Is the Prognosis of GBS?
Most patients with GBS gradually improve and can have a complete recovery over 6 to 12 months. However, some patients have residual symptoms, including fatigue, pain, numbness, tingling, and muscle weakness. Some factors associated with a higher risk of death due to GBS include older age, more severe disease, and need for mechanical ventilation.
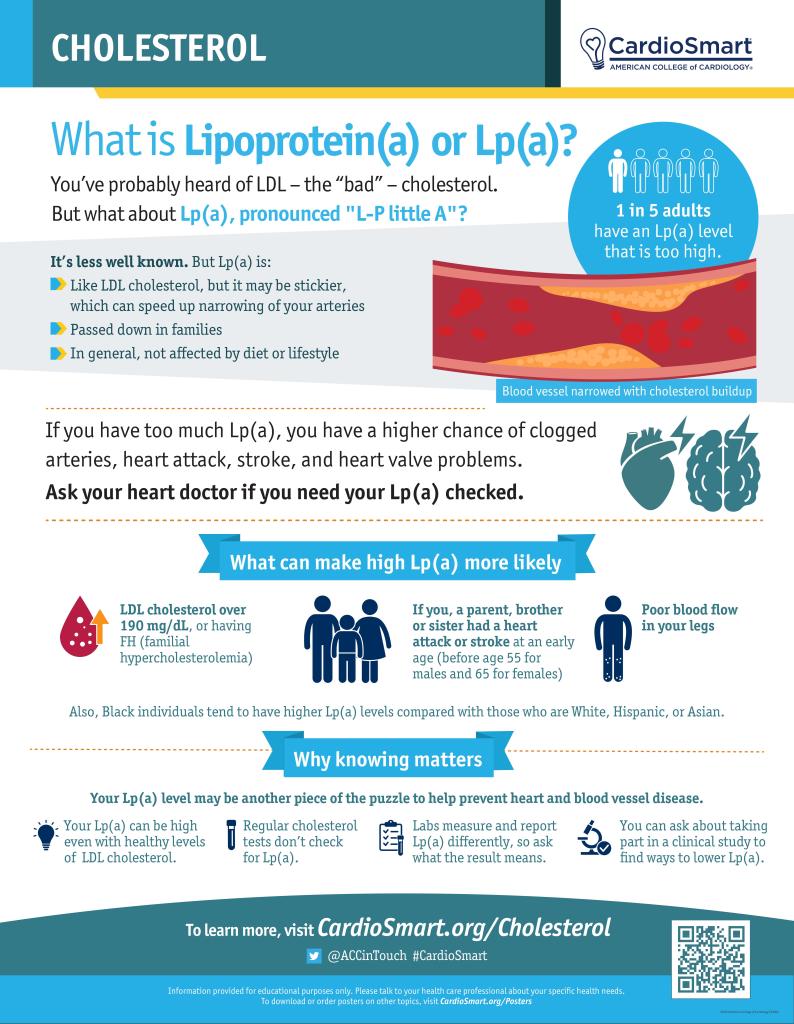
Lp(a), pronounced “L-P little A” is like LDL cholesterol, but stickier, which can speed up narrowing of your arteries. If you have too much Lp(a), you have a higher chance of clogged arteries, heart attack, stroke, and heart valve problems.
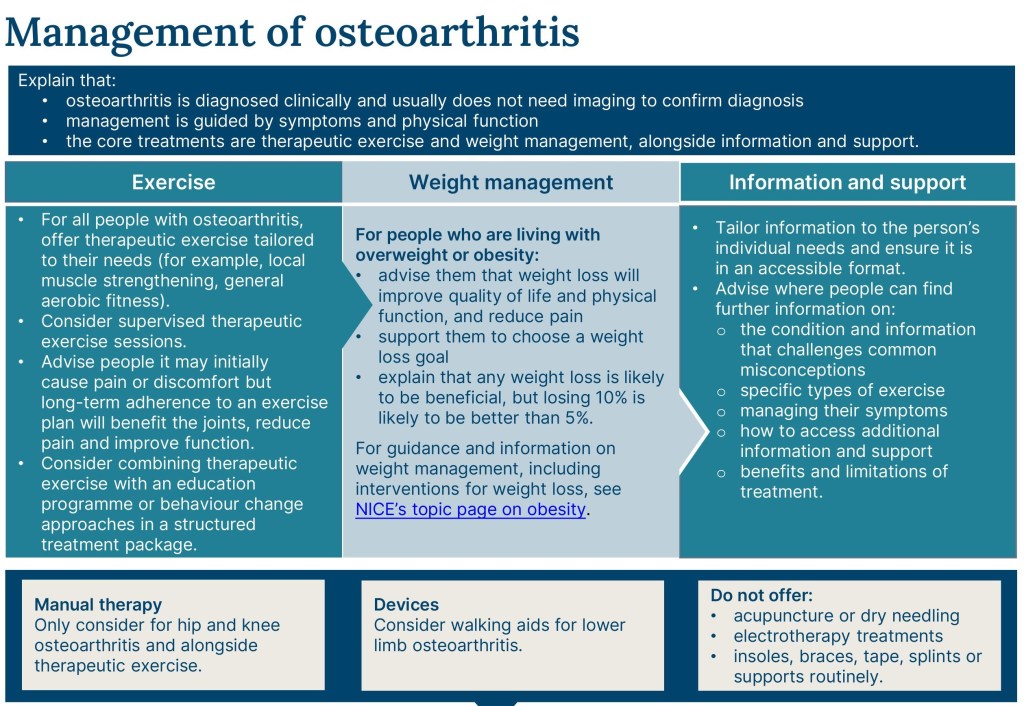
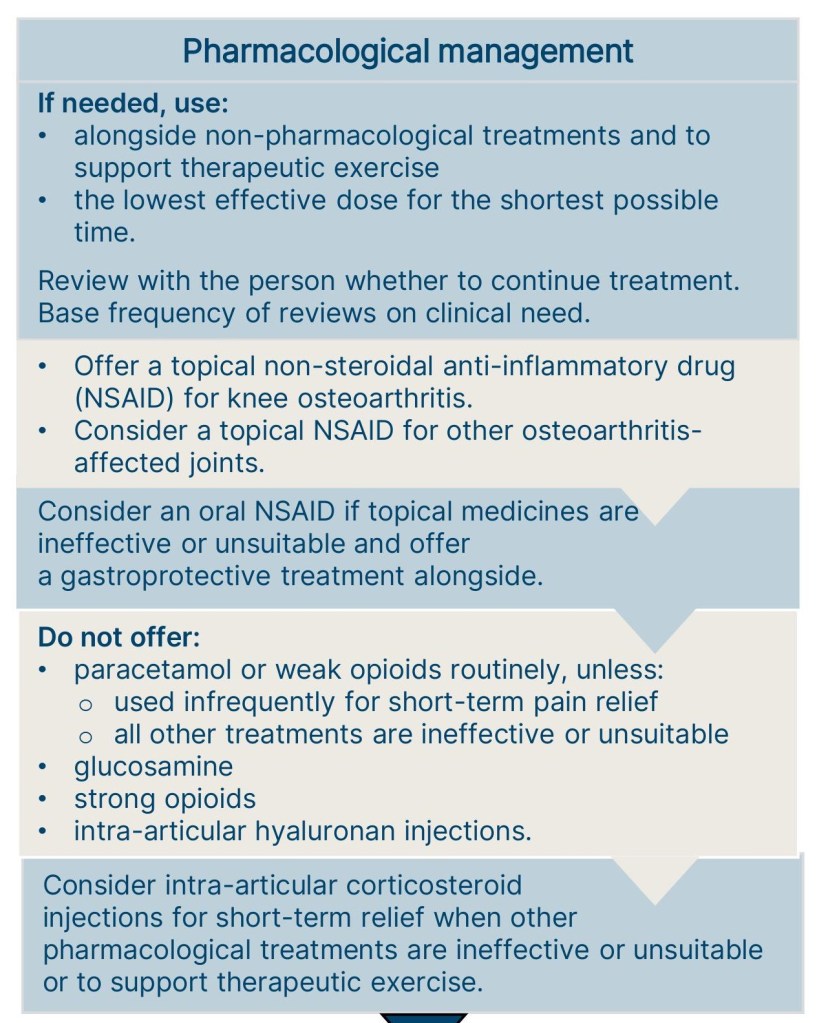
Osteoarthritis (OA) is the most common form of arthritis. Some people call it degenerative joint disease or “wear and tear” arthritis. It occurs most frequently in the hands, hips, and knees. With OA, the cartilage within a joint begins to break down and the underlying bone begins to change.
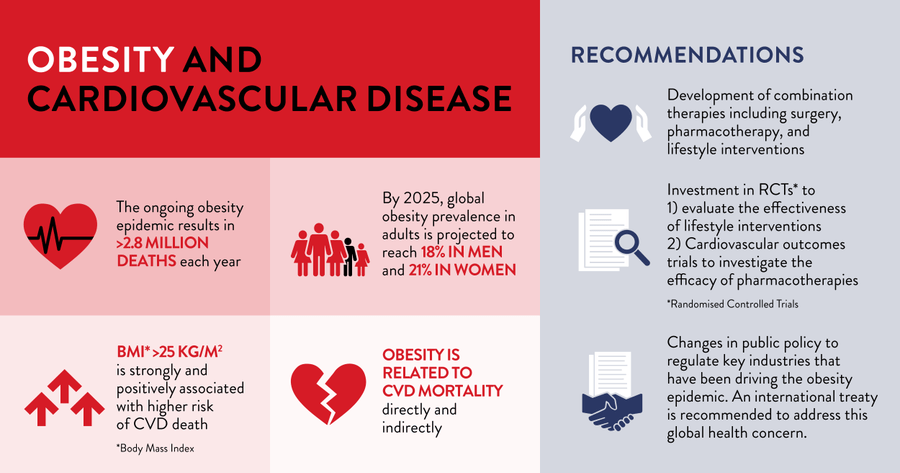
Our new position paper with @worldheartfed summarises the relationship between obesity and cardiovascular disease (#CVD) mortality.
World Obesity Federation (January 2023) – The ongoing obesity epidemic represents a global public health crisis that contributes to poor health outcomes, reduced quality of life, and >2.8 million deaths each year. Obesity is relapsing, progressive, and heterogeneous. It is considered a chronic disease by the World Obesity Federation (WOF) and a chronic condition by the World Heart Federation (WHF).
People living with overweight/obesity are at greater risk for cardiovascular (CV) morbidity and mortality. Increased adiposity (body fat), particularly visceral/abdominal fat, is linked to CV risk and CV disease (CVD) via multiple direct and indirect pathophysiological mechanisms. The development of CVD is driven, in part, by obesity-related metabolic, endocrinologic, immunologic, structural, humoral, haemodynamic, and functional alterations.
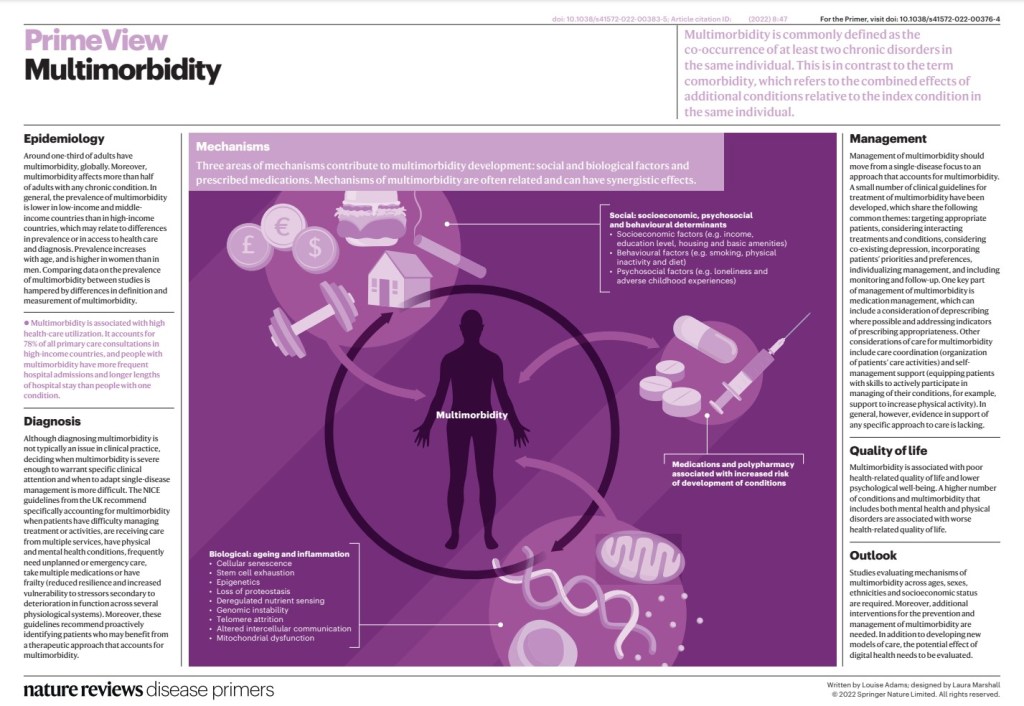
People with multimorbidity (two or more coexisting conditions in an individual) are more likely to die prematurely, be admitted to hospital and have an increased length of stay than people with a single chronic condition.
Multimorbidity is also associated with poorer function and health-related quality of life (HRQOL), depression and intake of multiple drugs (polypharmacy) and greater socioeconomic costs. Most health care is designed to treat individual conditions rather than providing comprehensive, person-centreed care, which often leads to fragmented and sometimes contradictory care for people with multimorbidity and increases their treatment burden. Moreover, treating one condition at a time is inefficient and unsatisfactory for both people with multimorbidity and their health-care providers.
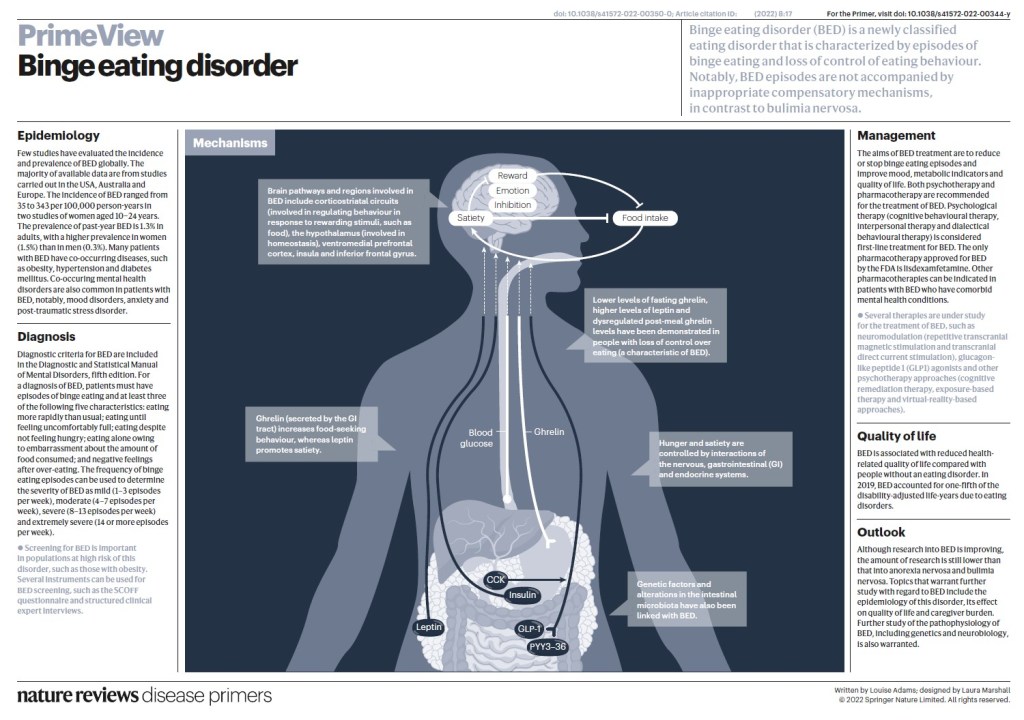
Most people with binge-eating disorder are overweight or obese, but you may be at a normal weight. Behavioral and emotional signs and symptoms of binge-eating disorder include:
Eating unusually large amounts of food in a specific amount of time, such as over a two-hour period
Feeling that your eating behavior is out of control
Eating even when you’re full or not hungry
Eating rapidly during binge episodes
Eating until you’re uncomfortably full
Frequently eating alone or in secret
Feeling depressed, disgusted, ashamed, guilty or upset about your eating