You know you need to get enough sleep, but the question remains: How much is enough? Sleep scientist Matt Walker tells us the recommended amount for adults and explains why it’s necessary for your long-term health. Sleeping with Science, a TED original series, uncovers the facts and secrets behind our nightly slumber. (Made possible with the support of Beautyrest)
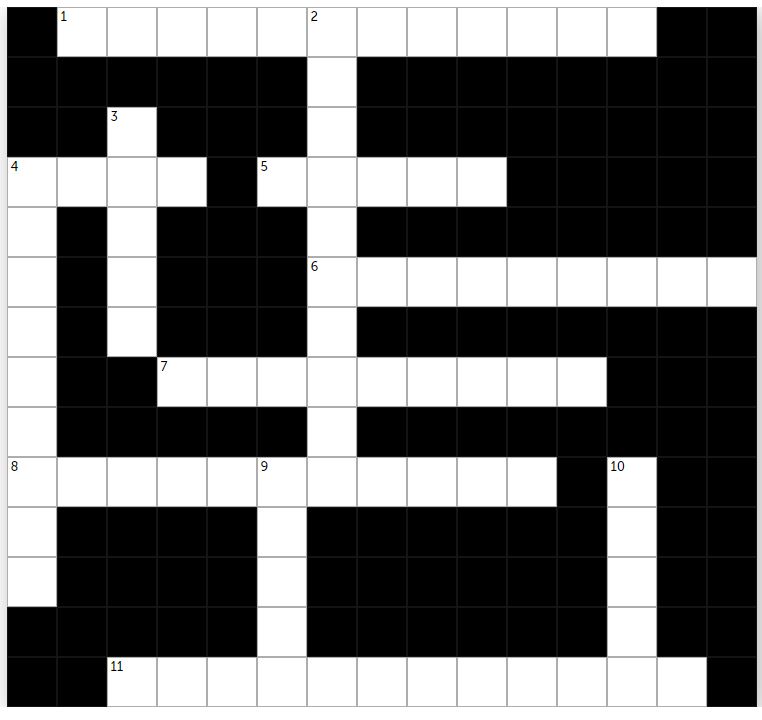
According to a recent study, obesity increases the risk of dying of Covid-19 by nearly 50%. Governments around the world are now hoping to encourage their citizens to lose weight. But with so much complex and often contradictory diet advice, as well as endless food fads, it can be hard to know what healthy eating actually looks like.
How many pieces of fruit and vegetables should you eat a day? Will cutting out carbs help you lose weight? Is breakfast really the most important meal of the day? Speaking to Tim Spector, professor of genetic epidemiology at King’s College London about his new book Spoon-Fed, Madeleine Finlay asks why we’re still getting food science wrong, and explores the current scientific evidence on snacking, supplements and calorie labels.
Tim Spector is a Professor of Genetic Epidemiology and Director of the TwinsUK Registry at Kings College, London and has recently been elected to the prestigious Fellowship of the Academy of Medical Sciences. He trained originally in rheumatology and epidemiology. In 1992 he moved into genetic epidemiology and founded the UK Twins Registry, of 13,000 twins, which is the richest collection of genotypic and phenotypic information worldwide. He is past President of the International Society of Twin Studies, directs the European Twin Registry Consortium (Discotwin) and collaborates with over 120 centres worldwide. He has demonstrated the genetic basis of a wide range of common complex traits, many previously thought to be mainly due to ageing and environment. Through genetic association studies (GWAS), his group have found over 500 novel gene loci in over 50 disease areas. He has published over 800 research articles and is ranked as being in the top 1% of the world’s most cited scientists by Thomson-Reuters. He held a prestigious European Research Council senior investigator award in epigenetics and is a NIHR Senior Investigator. His current work focuses on omics and the microbiome and directs the crowdfunded British Gut microbiome project. Together with an international team of leading scientists including researchers from King’s College London, Massachusetts General Hospital, Tufts University, Stanford University and nutritional science company ZOE he is conducting the largest scientific nutrition research project, showing that individual responses to the same foods are unique, even between identical twins. You can find more on https://joinzoe.com/ He is a prolific writer with several popular science books and a regular blog, focusing on genetics, epigenetics and most recently microbiome and diet (The Diet Myth). He is in demand as a public speaker and features regularly in the media.
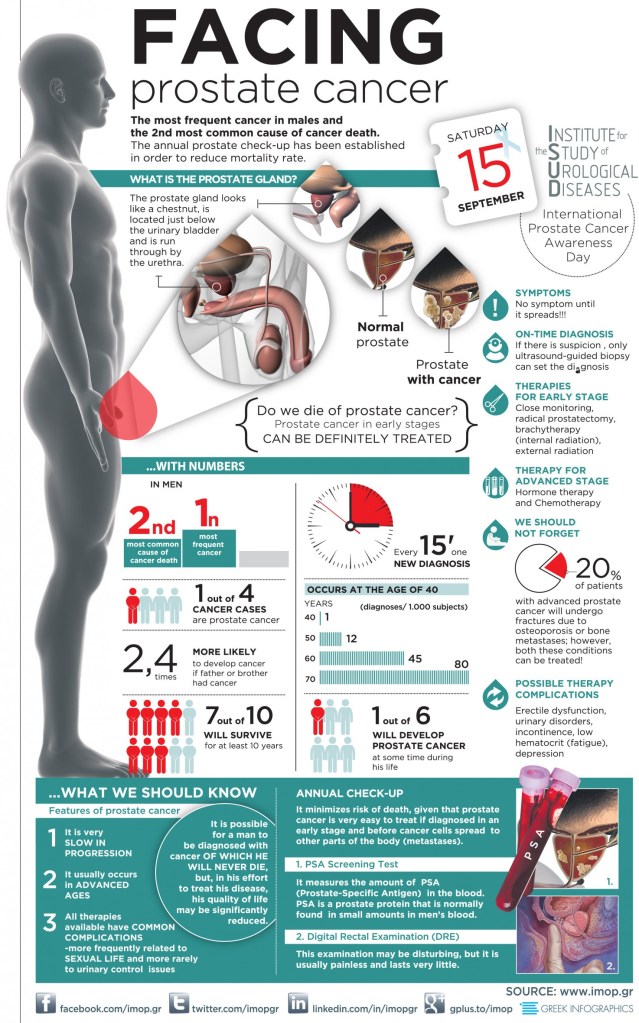
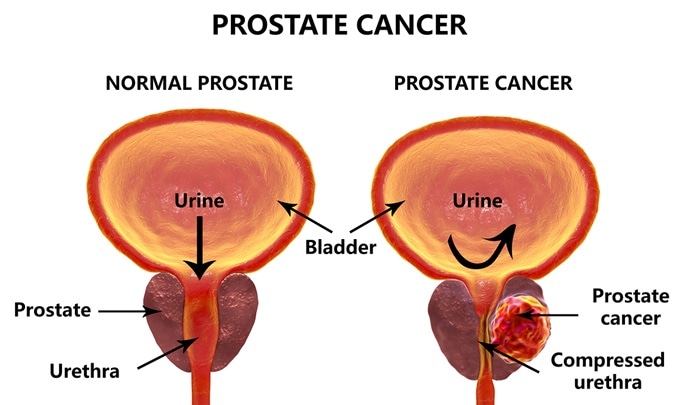
Prostate cancer is perhaps the most common cancer in men. It increases in incidence with age, and if you live long enough, most men will contract prostate cancer. A family history of cancer and obesity are also risk factors. But many times the cancer is so slow growing that it will not kill you. In the age of modern, aggressive medicine, the treatment has often been worse than the disease.
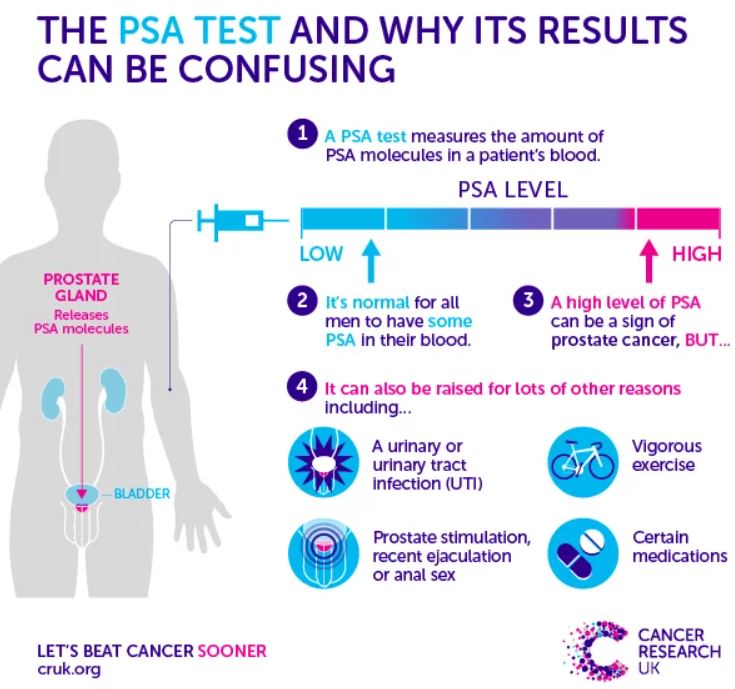
Treating Cancer EARLY is much more successful. The PSA test was one of the first really sensitive blood tests for cancer, and it was once performed routinely, on a yearly basis, usually at the time of your annual physical.
The PSA (Prostate-Specific Antigen) test is VERY sensitive,however. In responding to an elevated PSA, very slow growing tumors would often be treated aggressively, creating more morbidity than the untreated tumor would have caused.
The treatment seemed to be worse than the disease. Many physicians stopped doing the PSA test altogether, relying on symptoms, or detecting an abnormality on RECTAL EXAM to trigger an investigation. Some years ago, a physician friend of mine elected to stop PSA testing, and two years later was discovered to have METASTATIC Prostate cancer. It had already spread to his bones, and he eventually died of that cancer.
This encouraged me to continue with PSA screening, though it is still considered optional. Very recently, a test has been developed which I think tips the scales back toward annual PSA testing. EXOSOMES are little (10-120 nm.) particles that effuse from many cells, especially cancer cells.
They contain a variety of DNA, RNA, proteins and lipids which allow the cells to communicate with one another. Recently, a company, ExoDx, was created to take commercial advantage of Exosomes in the diagnosis of various diseases, by testing body fluids.
Their test, ExoRx Prostate EPI test of urine, has been shown to be helpful in distinguishing AGGRESSIVE prostate cancer from the slower growing kind, when the PSA test is in the “grey zone” between 2 and 10 ng/ml. PSA test results above 10 ng. were always acted on, especially if the numbers were increasing. I would be surprised if the PSA did not reenter the annual testing protocol.
The annual digital rectal exam in men older than 50 years will continue to be done, although it is not very sensitive, and is often not abnormal until the cancer is more advanced. Pain in the prostate area, blood in the urine or semen, and trouble urinating are symptoms worth investigating, but if cancer is detected, it may well be advanced and harder to treat. With abnormal tests,
Risk factors or suspicious symptoms, further testing is often done. Ultrasound or biopsy may be indicated. Sometimes the biopsy is guided by MRI, to increase the likelihood that the cancer, if small, is included in the tissue sample taken. Examining the cells of the biopsy sample will yield a “gleason score” which grades the aggressiveness of the cancer.
This in turn dictates the treatment, which may include different extents of surgical removal, radiation, hormonal or chemotherapy treatment. None of this is pleasant, and you are better off, of course with prevention.
Our old friends, DIET AND EXERCISE are thought to be helpful. Although not proven, eating lots of fruits and vegetables, and maintaining a healthy weight are recommended.
–DR. C
Finasteride, one of the drugs in my medicine cabinet is mentioned as a possible aid. I will be discussing this later. I suggest that you press the green box with the magnifying glass, and type the name of the drug to see if i have discussed it. –Dr. C.
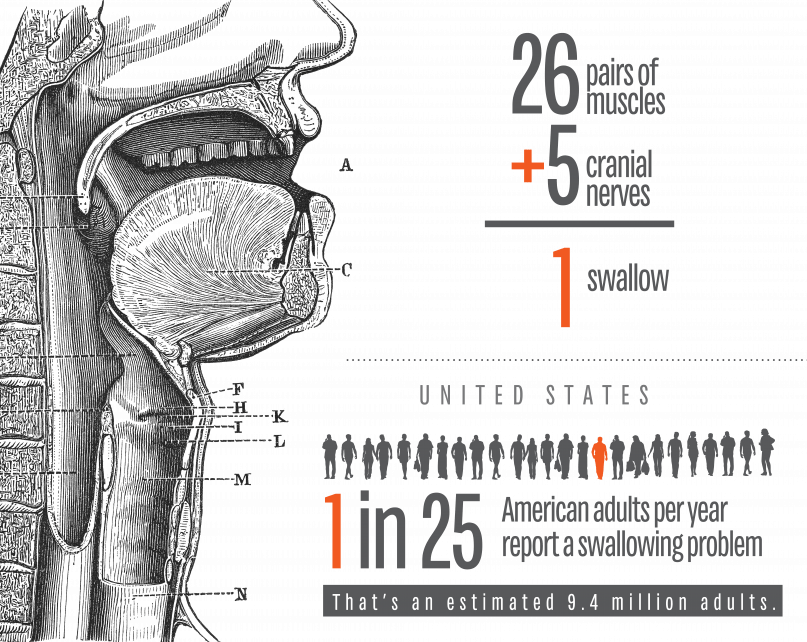
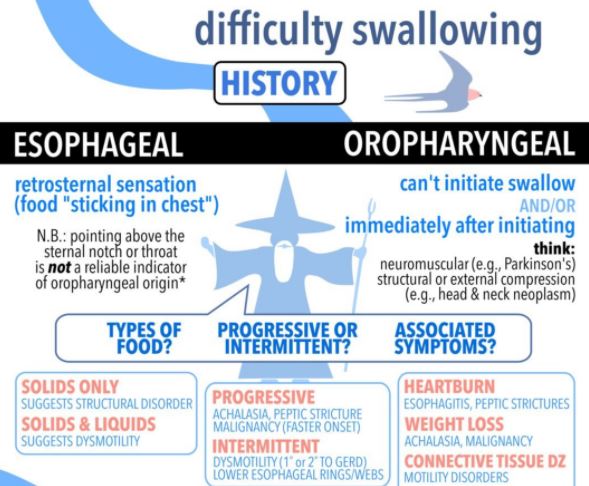
I am defining SWALLOWING TROUBLE as the difficulty in transport of food to the stomach, once clear of the throat. Problems with the initiation of the swallowing process are discussed separately.
PAIN in the mid-chest ON SWALLOWING is a worrisome symptom which can be due to inflammation of the lining of the esophagus from a variety of causes. An esophageal yeast infection, which can also involve the throat (called ‘“thrush”), often warns of immune deficiency and can be a sign of AIDS, or be caused by immune suppressing medication. If persistent, pain on swallowing can be a warning sign of CANCER.
If in the presence of GERD, it can be a sign of chronic inflammation or ulceration. In-coordination of the normally smooth muscular propulsive wave can cause a cramping, muscular pain.
Normal “peristalsis” is so efficient, that food can be swallowed without the help of gravity, when UPSIDE DOWN. I wouldn’t recommend trying this, even to cure hiccoughs. There is a muscular “gate” at the bottom of the esophagus, just as it enters the stomach. This gate is often too relaxed, and allows for the reflux of acid and food from the stomach, or GERD. It can also Fail to open, called achalasia, and hold up the food in its journey to the stomach.
The area can be scarred by repeated acid reflux, and become NARROWED; this is called a STRICTURE, and can cause a blockage in swallowing. One of my Doctor friends had to go to the Emergency room when some Steak got stuck in the esophagus.
The ER Doctor removed the steak with a fiberoptic Scope, and then proceeded to DILATE the stricture with a “bougie”, an instrument of a precisely calibrated size designed to STRETCH the constricted area. This uncomfortable procedure had to be done repeatedly, a caution to those who would wait too long before getting such a problem evaluated and corrected.
EOSINOPHILIC ESOPHAGITIS has been diagnosed with increasing frequency, and can cause Pain in the middle of the chest, trouble swallowing, and even regurgitation of food. This special type of inflammation is more common in allergic patients, and can be caused by certain foods.
So as you can see, swallowing trouble, if persistent, is nothing to fool around with, and should be checked out by a competent doctor. Don’t wait too long.
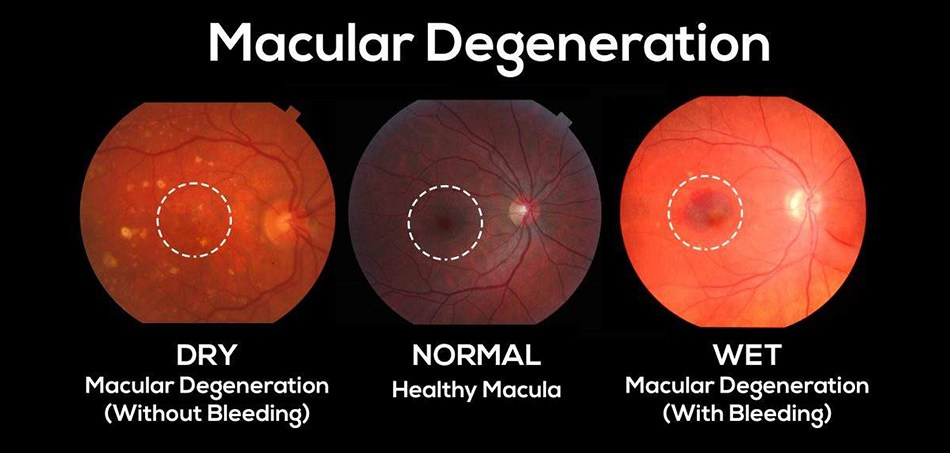
Macular Degeneration is the most common cause of blindness in the western world.as you get older, it becomes increasingly common, and almost 20% of people older than 85 years have this disease.
It comes in 2 types, dry and wet. Mostly it starts as the milder dry type, which develops slowly and has no definite treatment. The dry type can develop into the more rapidly progressive wet variety, however, and is important to notice and report to your ophthalmologist.
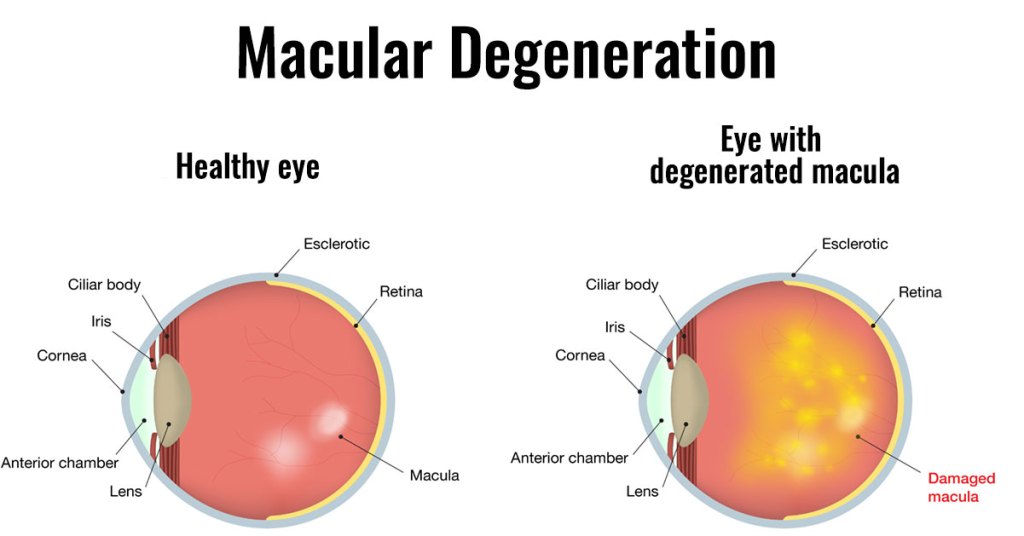
The MACULA is the center of the visual field, and has by far the most photoreceptors. It yields the sharpest vision, and is essential for reading, and even recognizing faces.
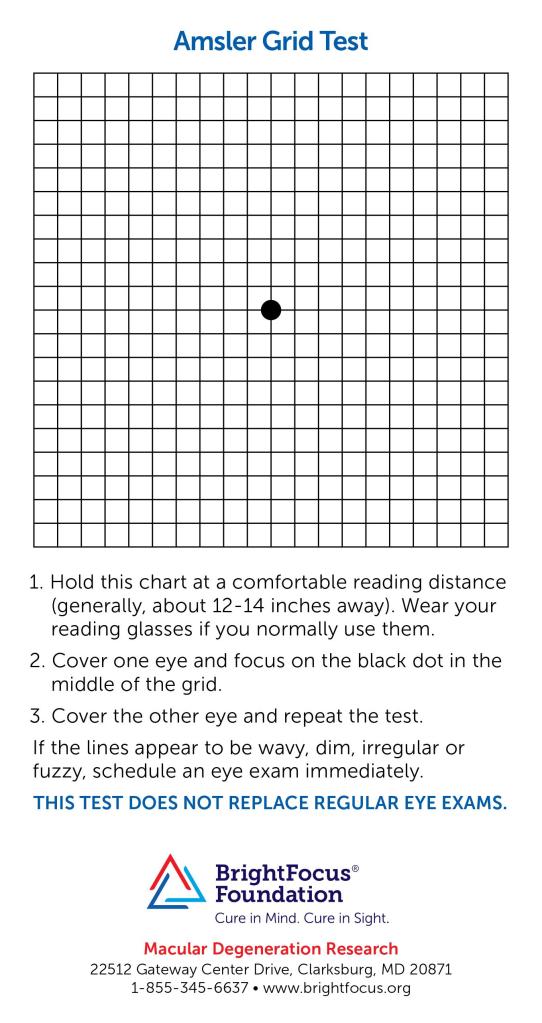
LOSS OF VISION is the commonest symptom, but is hard to notice in a slowly developing condition. A neurologist friend of mine alerted me to the AMSLER GRID, which helps in picking up the subtle distortions of this sneaky problem.
Checking your vision every few days-it takes only a few seconds- is a good idea as you age. You might be healthy in every other way, but if you are blind, the quality of life in your final years will suffer. The mechanics of the wavy lines generated by macular degeneration are deposits beneath the macula, raising it up.
The deposits are fatty in the case of the dry, and fluid in the case of the wet macular degeneration; and fluid from the abnormal blood vessels in the wet MD can collect very rapidly indeed.
Even though the cause of MD is unknown, prevention is by the same old healthy habits tiresomely mentioned in all my other postings: DIET and EXERCISE. I’m sure that good sleep doesn’t hurt either, No cigarette smoking of course, and there are some vitamins and minerals mentioned, such as lutein, zeaxanthin, zinc, and copper.
The wet MD does have a treatment to slow down the disease. Since blood vessel growth is important in causation, antibodies to VEGF, vascular endothelial growth factor, are injected into the macular area. I’m sure that more help is on the way. Some treatments to support the protective pigmented layer of the retina are currently in progress.





 Finasteride, one of the drugs in my medicine cabinet is mentioned as a possible aid. I will be discussing this later. I suggest that you press the green box with the magnifying glass, and type the name of the drug to see if i have discussed it. –Dr. C.
Finasteride, one of the drugs in my medicine cabinet is mentioned as a possible aid. I will be discussing this later. I suggest that you press the green box with the magnifying glass, and type the name of the drug to see if i have discussed it. –Dr. C.