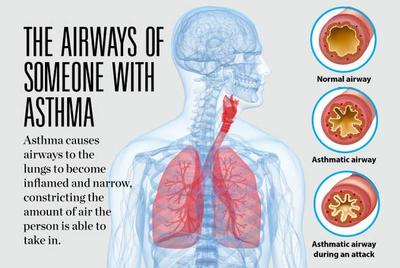
COPD is the brother of asthma. Both can cause shortness of breath and wheezing. Asthma is the more Treatable of the two, and is due to muscle spasm around the airways which narrow those airways making it more difficult to breathe in and especially out.
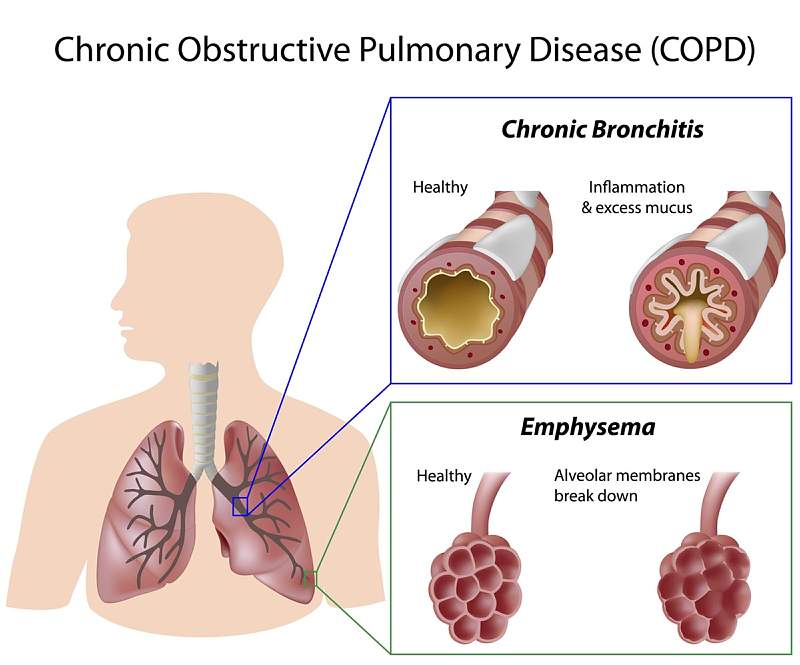
COPD comes in 2 general forms, Chronic bronchitis and emphysema.
Chronic bronchitis is an inflammation of the airways, which differs from the usual allergic asthmatic TH2 type of inflammation. The inflammation of chronic bronchitis is the more common TH1 inflammation that comes from the likes of bacteria and viruses.
The second type of COPD is usually caused by cigarette smoke or other fumes which lead to the destruction of the air sacs and associated elastic tissue, allowing a check valve type of obstruction to occur on breathing out.
COPD is rarely a pure type of chronic bronchitis or emphysema, and is usually an admixture of the two. In fact there can be an “asthmatic element” mixed into COPD, which allows for a better response to the myriads of medication that we now have for asthma.
The symptoms of COPD include shortness of breath, wheezing, chest tightness and chronic cough with production of sputum. Coughing up a significant volume of phlegm from your chest suggests chronic bronchitis rather than emphysema.
The symptoms of COPD come on rather slowly and are usually not noticed until the problem is severe. After all, the cigarette smoker is EXPECTED to cough isn’t he?
As COPD becomes very advanced, fatigue, lack of energy, and unintended weight loss may occur. Swelling of the legs may be a problem and could indicate involvement of a heart; with COPD the right side of the heart has a hard time moving blood through the diseased lungs.
We’ve all seen people pushing around a cart with an oxygen tank. These people most often are smokers who developed COPD. One particularly disgusting advertisement against cigarette smoking showed a person with a hole in the windpipe (tracheostomy) through which he was smoking his cigarette.
Pulmonary function testing it’s often helpful in diagnosing asthma and COPD. In pulmonary function testing, the amount of air in the lungs and the rapidity with which it can be expelled from the Lungs is measured and graphed. it is the rate of flow on exhalation that is diminished in COPD and asthma, the slower the rate the worse the blockage.
In the case of asthma the test is repeated after a bronchodilating adrenaline type medication has been given. The REVERSIBILITY of the airway obstruction is shown by comparing the airway function before and after treatment With no improvement, usually COPD is usually the culprit.
In both asthma and COPD, respiratory infection is a big problem. The compromised lung is usually very vulnerable to these inflammatory reactions. There are a score of medications that are commonly used in asthma which also benefit COPD to a certain degree. Doctors have a large armamentarium for respiratory disease these days.
As mentioned, asthma is more treatable. However if it is poorly treated or neglected, a condition known as REMODELING can occur which will render treatment less effectual.
Please check with the Mayo clinic article on COPD for more information.