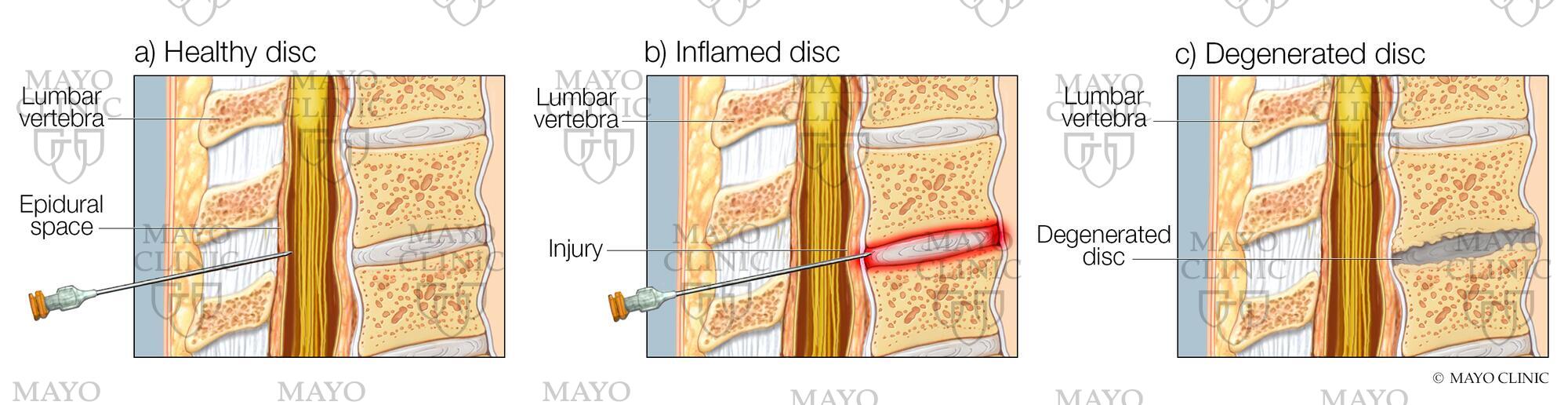
#DegenerativeDiskDisease is a common disorder linked to aging and years of wear and tear on the spine. Long-term therapies have so far eluded medical science.
LAMINECTOMY
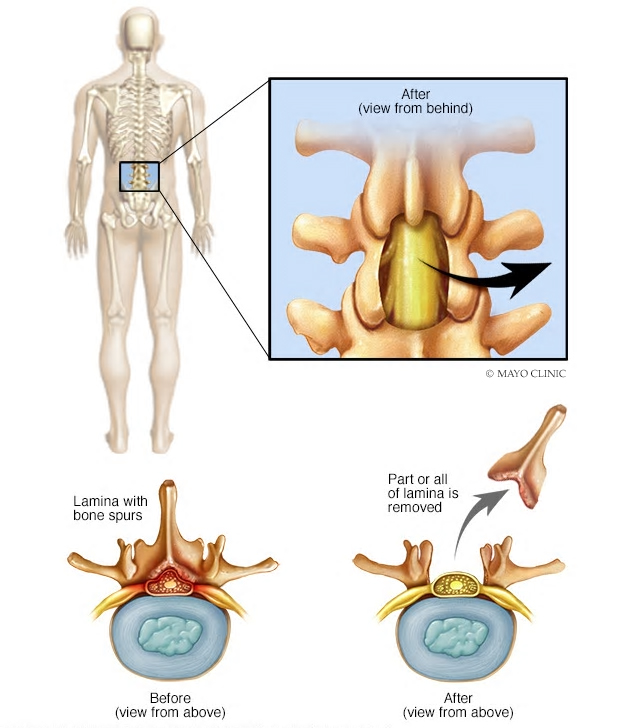
Laminectomy is surgery that creates space by removing the lamina — the back part of a vertebra that covers your spinal canal. Also known as decompression surgery, laminectomy enlarges your spinal canal to relieve pressure on the spinal cord or nerves.
This pressure most commonly is caused by bony overgrowths within the spinal canal, which can occur if you have arthritis in your spine. These overgrowths sometimes are referred to as bone spurs, but they’re a normal side effect of the aging process in some people.
Some patients are able to have a same-day laminectomy, which means they do not need to stay in the hospital following surgery and are able to go home to recover. The procedure is performed using minimally invasive techniques resulting in smaller incisions, lower risk of infection and, for many people, a quicker recovery.
SPINAL FUSION
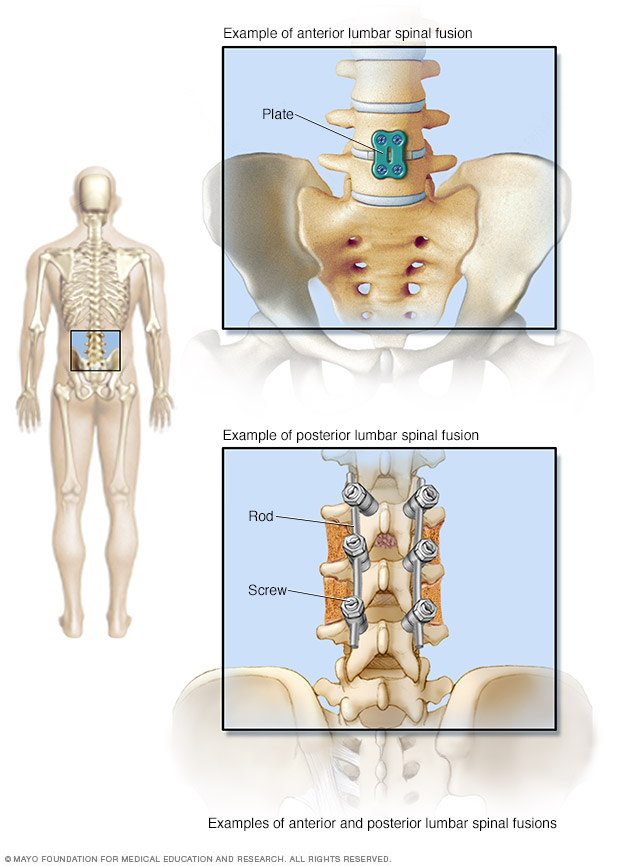
Spinal fusion is surgery to permanently connect two or more vertebrae in your spine, eliminating motion between them. Spinal fusion involves techniques designed to mimic the normal healing process of broken bones. During spinal fusion, your surgeon places bone or a bone-like material within the space between two spinal vertebrae. Metal plates, screws and rods may be used to hold the vertebrae together, so they can heal into one solid unit.
Because spinal fusion surgery immobilizes parts of your spine, it changes the way your spine can move. This places additional stress and strain on the vertebrae above and below the fused portion, and may increase the rate at which those areas of your spine degenerate.