

A new recipe for patterning cells on a surface holds promise for spinal cord injuries. Video by the Office of Communications
Yearly Archives: 2020

DR. C’S PODCAST: WEEKLY MEDICAL NEWS (OCT 25)
DR. C REVIEWS MAJOR HEALTH AND TELEMEDICAL NEWS FOR THE WEEK ENDING OCTOBER 25, 2020.

COVID-19 INFOGRAPHIC: ‘THE JOURNEY OF A VACCINE’ (NIH)


COVID-19 INFOGRAPHIC: ‘EXERCISE IS MEDICINE’ (BMJ)
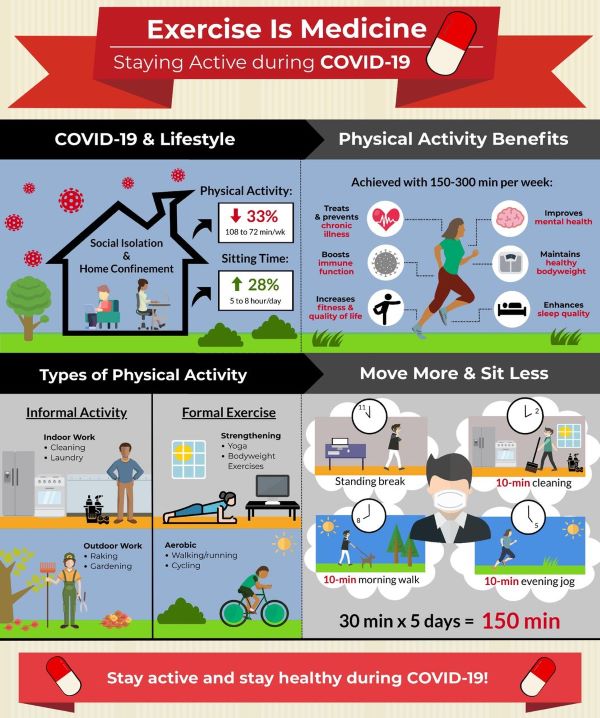
There are over 35,000,000 reported cases of COVID-19 disease and 1 000 000 deaths across more than 200 countries worldwide.1 With cases continuing to rise and a robust vaccine not yet available for safe and widespread delivery, lifestyle adaptations will be needed for the foreseeable future. As we try to contain the spread of the virus, adults are spending more time at home. Recent evidence2 suggests that physical activity levels have decreased by ~30% and sitting time has increased by ~30%. This is a major concern as physical inactivity and sedentary behaviour are risk factors3 for cardiovascular disease, obesity, cancer, diabetes, hypertension, bone and joint disease, depression and premature death.
To date, more than 130 authors from across the world have provided COVID-19-related commentary on these concerns. Many experts4 have emphasised the importance of increasing healthy living behaviours and others5 have indicated that we are now simultaneously fighting not one but two pandemics (ie, COVID-19, physical inactivity). Physical inactivity alone results in over 3 million deaths per year5 and a global burden of US$50 billion.6 Immediate action is required to facilitate physical activity during the COVID-19 pandemic because it is an effective form of medicine3 to promote good health, prevent disease and bolster immune function. Accordingly, widespread messaging to keep adults physically active is of paramount importance.
Several organisations including the WHO, American Heart Association and American College of Sports Medicine have offered initial suggestions and resources for engaging in physical activity during the COVID-19 pandemic. Expanding on these resources, our infographic aims to present a comprehensive illustration for promoting daily physical activity to the lay audience during the COVID-19 pandemic (figure 1). As illustrated, adults are spending more time at home, moving less and sitting more. Physical activity provides numerous health benefits, some of which may even help directly combat the effects of COVID-19. For substantial health benefits, adults should engage in 150–300 min of moderate-to-vigorous intensity physical activity each week and limit the time spent sitting. The recommended levels of physical activity are safely attainable even at home. Using a combination of both formal and informal activities, 150 min can be reached during the week with frequent sessions of physical activity spread throughout the day. Sedentary behaviour can be further reduced by breaking up prolonged sitting with short active breaks. In summary, this infographic offers as an evidence-based tool for public health officials, clinicians, educators and policymakers to communicate the importance of engaging in physical activity during the COVID-19 pandemic.

Covid-19: ‘Why Doctors & You Should Wear Masks’
Learn more about the Yale School of Medicine and #YaleMedicine‘s response to COVID-19, visit: https://covid.yale.edu.

THE DOCTORS 101 CHRONIC SYMPTOMS & CONDITIONS #20: KIDNEY FAILURE (ESRD)
Our Kidneys and Liver have a lot in common. They are not dramatic, take-care-of-me-now organs like our Hearts and Brain, but usually do their job quietly until they lose almost all of their function. They have lots of reserve; you can donate one of your kidneys or a piece of your liver and notice no change. They are both vital organs, and you will die without them.
Since they both help clear wastes and toxins from the bloodstream and produce hormones, they SHARE SYMPTOMS such as nausea, vomiting, fatigue, and mental changes.Their performance can be checked by blood tests. Healthy habits will protect their -and your- survival.
Certain Drugs impair their operation. They are both composed of many identical functional units, the nephron in the kidney, and the hepatic lobule in the liver.
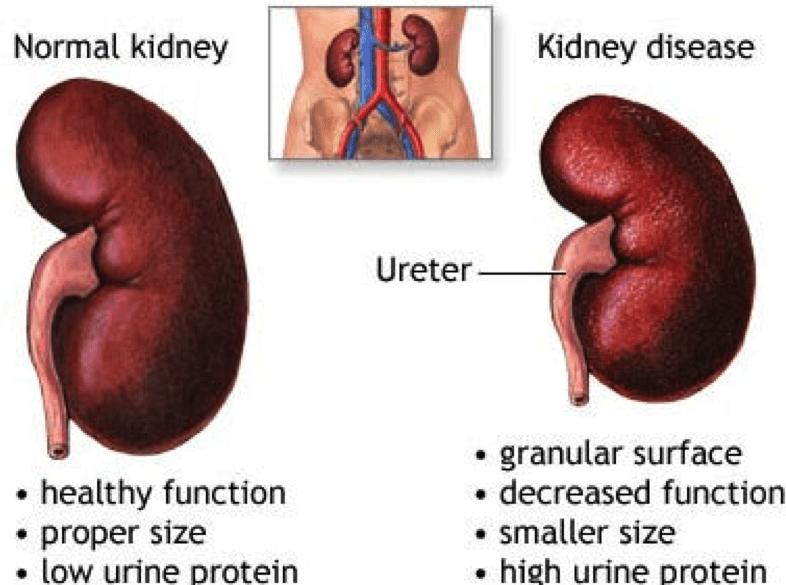
The GLOMERULUS of the Nephron is a tuft or ball of capillaries and associated kidney cells that allow the fluid and dissolved molecules of the blood to come through, while restraining the larger proteins and cells of the blood, keeping them in the vascular system. The smaller molecules of sodium, potassium, urea and other waste products leak through the glomerulus.
This filtered liquid travels through the long, folded kidney tubules, where the RIGHT AMOUNT of salt and water are REABSORBED. This keeps the vascular fluids, the internal environment, the MILIEU INTERIOR, perfectly well adjusted for proper cell function. It is when the chemical environment of the body falls out of adjustment, when the kidneys FAIL to do their job, that the cells of the body cannot function properly, and Symptoms-fatigue, lethargy etc. – develop.
BLOOD PRESSURE is intimately involved with the KIDNEYS, which has an Endocrine function. The Renin( Renal=kidneys) Angiotensin system is a major regulator of blood pressure.
You may have heard of the ACE-2 receptor as the binding site of th COVID Virus. This Angiotensin Converting Enzyme receptor is on the surface of cells all over the body and normally functions to control blood pressure.
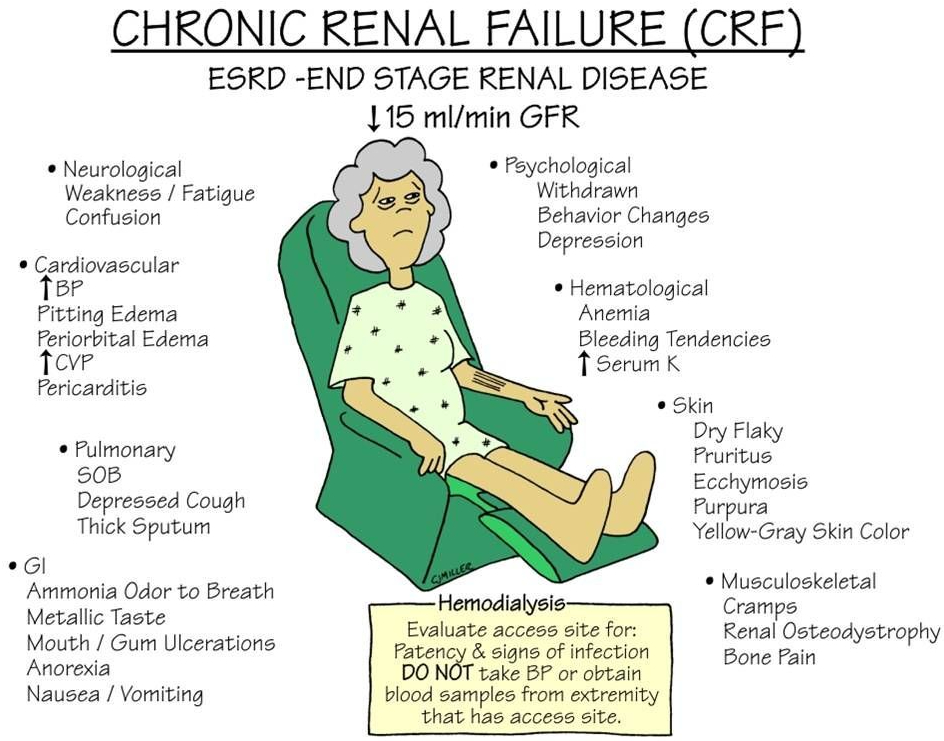
DIABETES is the most common cause of end stage renal disease (ESRD), bringing our healthy triad of SLEEP DIET and EXERCISE to our attention once again.
POLYCYSTIC KIDNEY DISEASE is an inherited condition where many nephrons fail to hook up to the urine collecting system, and the fluid builds up into cysts, which then eventually replace the rest of the kidney. Pressure from urine blockage by an enlarged prostate, or even lack of ureteral valves can also back up into the kidneys and eventually cause ESRD.
Infections and autoimmune diseases can result in ESRD. Treatment of ESRD is usually a Kidney transplant or Dialysis. There is a waiting list for the former and the latter is life-altering. You can’t beat a healthy lifestyle.
–Dr. C.
THE DOCTORS 101 CHRONIC SYMPTOMS & CONDITIONS #19: DIVERTICULOSIS
Your large bowel, or colon, is at the end of the Gastrointestinal tract. It starts on the right side of your abdomen, where the small intestine empties into the caecum. This is also where the Appendix bulges down, looking like a little finger coming from the caecum. The 5 foot long large intestine is the final processing area of your food, after the nutrients have been absorbed.
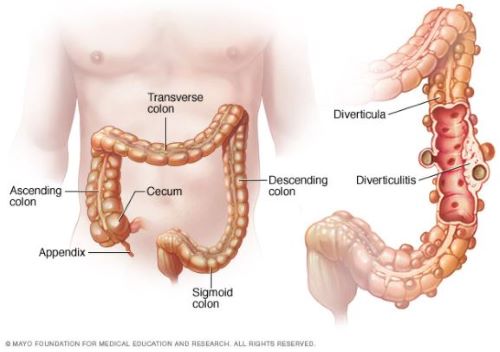
The Colon contains virtually all of the microbiome, reduces the volume of the fecal matter, and propels it to its final destination. The propelling muscles are an inner circular ring, and 3 outer longitudinal strips. These outer strips of muscle do not completely encircle the Colon, allowing for protuberances of lining membrane and circular muscle to balloon out into prominences called Taenia.
It is in these weakened areas, especially where blood vessels penetrate that little herniations form over the years. Diverticulosis occurs in 50% of people more than 60 years of age, and in almost everybody more than 80 years.
Diverticulosis is a condition where pressures up to 120 mm or mercury, generated by the colonic muscles gradually push out little pouches of lining membrane called diverticula. Nobody knows why some people get an INFLAMMED diverticulum.
Age, of course, is a factor, as are Obesity, diabetes, smoking and poor diet; a tendency toward inflammation is common in all of these risk factors. Comparing diverticulitis with Appendicitis is an interesting exercise. The symptoms are mirror images of each other. Appendicitis occurs on the right side.
Diverticulitis usually occurs on the left side, except in asian people. The asian DIET seems to favor diverticula on the right side. When asians immigrate to the U.S. and start eating more Red meat and fewer vegetables, the diverticula shift to the left side.
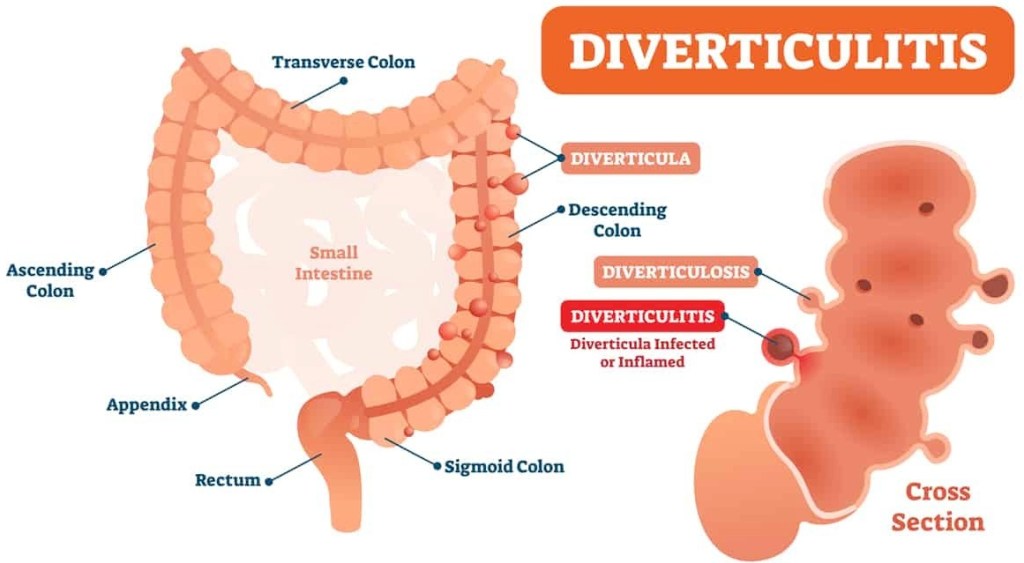
Signs of Diverticulitis include gastrointestinal symptoms, such as pain, tenderness,nausea, cramps, constipation, and Fever. Rectal bleeding can sometimes occur. Treatment includes antibiotics.
If the condition worsens, serious complications, such as abcess may develop and require surgery. As usual, Prevention, including diet and exercise, is better than Treatment. A HIGH FIBER DIET is the best prevention.
–Dr. C.
Article #1 to read – Diverticular disease of the colon: New perspectives in symptom development and treatment
Article #2 to read – Management of Colonic Diverticulitis | Effective Health Care Program

HEALTH: ‘DIABETES AND CHRONIC KIDNEY DISEASE’ – NEW GUIDELINES (OCT 2020)
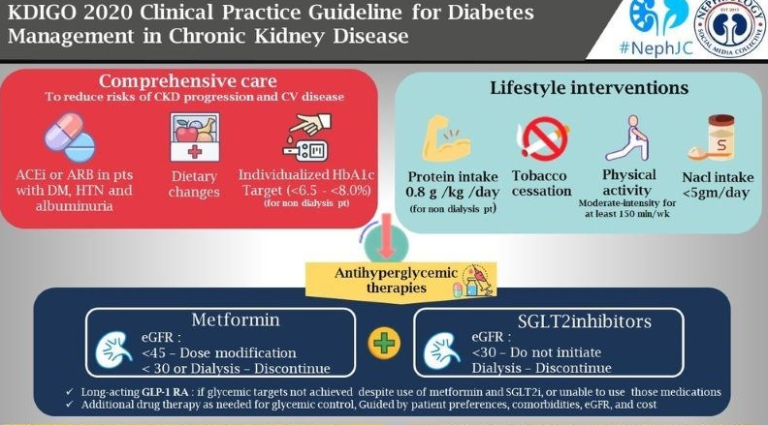

Comprehensive care in patients with diabetes and CKD
Management of CKD in diabetes can be challenging and complex, and a multidisciplinary team should be involved (doctors, nurses, dietitians, educators, etc). Patient participation is important for self-management and to participate in shared decision-making regarding the management plan. (Practice point).
We recommend that treatment with an angiotensin-converting enzyme inhibitor (ACEi) or an angiotensin II receptor blocker (ARB) be initiated in patients with diabetes, hypertension, and albuminuria, and that these medications be titrated to the highest approved dose that is tolerated (1B).
Lifestyle interventions in patients with diabetes and CKD
We suggest maintaining a protein intake of 0.8 g protein/kg)/d for those with diabetes and CKD not treated with dialysis (2C).
On the amount of proteins recommended in these guidelines, they suggest (‘recommend’ becomes a ‘suggest’ at this level of evidence) a very precise intake of 0.8g/kg/d in patients with diabetes and CKD. Lower dietary protein intake has been hypothesized but never proven to reduce glomerular hyperfiltration and slow progression of CKD, however in patients with diabetes, limiting protein intake below 0.8g/kg/d can be translated into a decreased caloric content, significant weight loss and quality of life. Malnutrition from protein and calorie deficit is possible.
Physical activity
We recommend that patients with diabetes and CKD be advised to undertake moderate-intensity physical activity for a cumulative duration of at least 150 minutes per week, or to a level compatible with their cardiovascular and physical tolerance (1D).

INFOGRAPHIC: ‘WHAT IS HERD IMMUNITY?’ – ACHIEVING IT WITH COVID-19 (JAMA)
What Is Herd Immunity?
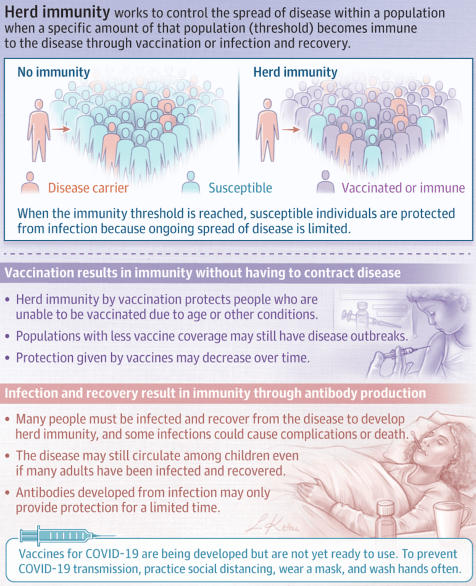
Herd immunity occurs when a significant portion of a population becomes immune to an infectious disease, limiting further disease spread.
Disease spread occurs when some proportion of a population is susceptible to the disease. Herd immunity occurs when a significant portion of a population becomes immune to an infectious disease and the risk of spread from person to person decreases; those who are not immune are indirectly protected because ongoing disease spread is very small.
The proportion of a population who must be immune to achieve herd immunity varies by disease. For example, a disease that is very contagious, such as measles, requires more than 95% of the population to be immune to stop sustained disease transmission and achieve herd immunity.
How Is Herd Immunity Achieved?
Herd immunity may be achieved either through infection and recovery or by vaccination. Vaccination creates immunity without having to contract a disease. Herd immunity also protects those who are unable to be vaccinated, such as newborns and immunocompromised people, because the disease spread within the population is very limited. Communities with lower vaccine coverage may have outbreaks of vaccine-preventable diseases because the proportion of people who are vaccinated is below the necessary herd immunity threshold. In addition, the protection offered by vaccines may wane over time, requiring repeat vaccination.
Achieving herd immunity through infection relies on enough people being infected with the disease and recovering from it, during which they develop antibodies against future infection. In some situations, even if a large proportion of adults have developed immunity after prior infection, the disease may still circulate among children. In addition, antibodies from a prior infection may only provide protection for a limited duration.
People who do not have immunity to a disease may still contract an infectious disease and have severe consequences of that disease even when herd immunity is very high. Herd immunity reduces the risk of getting a disease but does not prevent it for nonimmune people.
Herd Immunity and COVID-19
There is no effective vaccine against coronavirus disease 2019 (COVID-19) yet, although several are currently in development. It is not yet known if having this disease confers immunity to future infection, and if so, for how long. A large proportion of people would likely need to be infected and recover to achieve herd immunity; however, this situation could overwhelm the health care system and lead to many deaths and complications. To prevent disease transmission, keep distance between yourself and others, wash your hands often with soap and water or sanitizer that contains at least 60% alcohol, and wear a face covering in public spaces where it is difficult to avoid close contact with others.
DR. C’S PODCAST: WEEKLY MEDICAL NEWS (OCT 18)
DR. C REVIEWS MAJOR HEALTH AND TELEMEDICAL NEWS FOR THE WEEK ENDING OCTOBER 18, 2020.
