

The Idea that lack of certain nutritional factors could cause disease predates the germ theory by hundreds of years. British sailors could be saved from the ravages of SCURVY by a little sour fruit, and were called LIMEYS. Just before the first World War, a “milk factor” was found to be contained in butterfat, and was called Vitamin A.
The factor in “rice polishings”, known for decades to prevent disease caused by a diet exclusively of white, or “polished”rice was called Vitamin B.
Thus the Lettering system of vitamin-naming began. It wasn’t known until just before the Second World War that “vitamin B” was in fact several different substances (B1. B2. etc.), and later yet until these factors were found to be small, non-protein molecules that were “cofactors” in important enzymatic reactions essential in the body.
The metabolic pathways of our Hunter-gatherer ancestors could depend on the DIVERSE FOOD sources of Paleolithic man to supply these vital substances. Therefore, the body did not need to synthesize them, saving energy, but paving the way for future problems.
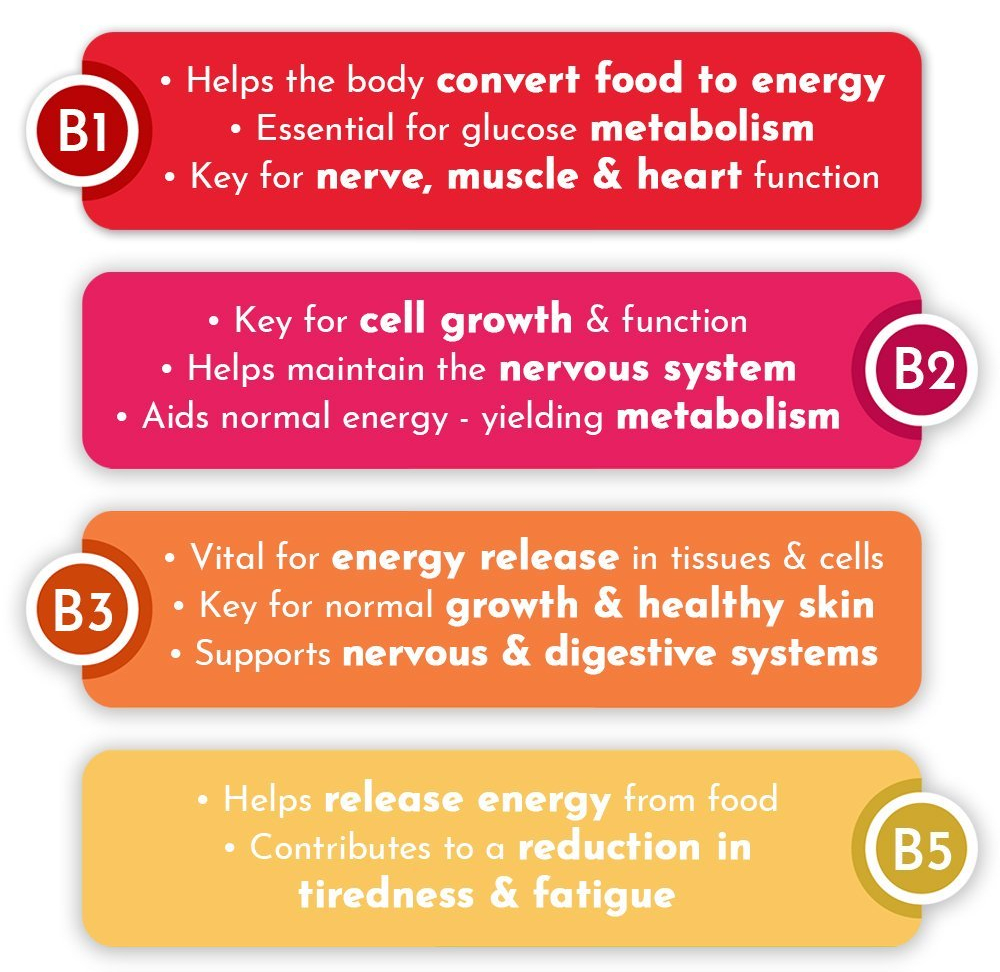
As a group, B vitamins produce energy from nutrients, support immune function, regulate cell growth, maintain Myelin, and maintain RBCs, among other crucially important things.
Some substances used to be considered B Vitamins, were later found to be synthesized in our bodies: these include Choline, Carnitine, Lipoic acid and PABA.
The latter is essential to Bacteria, leading to the development of the Sulfa Drugs, which Block PABA synthesis. Another pair of substances are so widely present in foods as to be rarely deficient: B5, Pantothenic acid, and B7, Biotin.
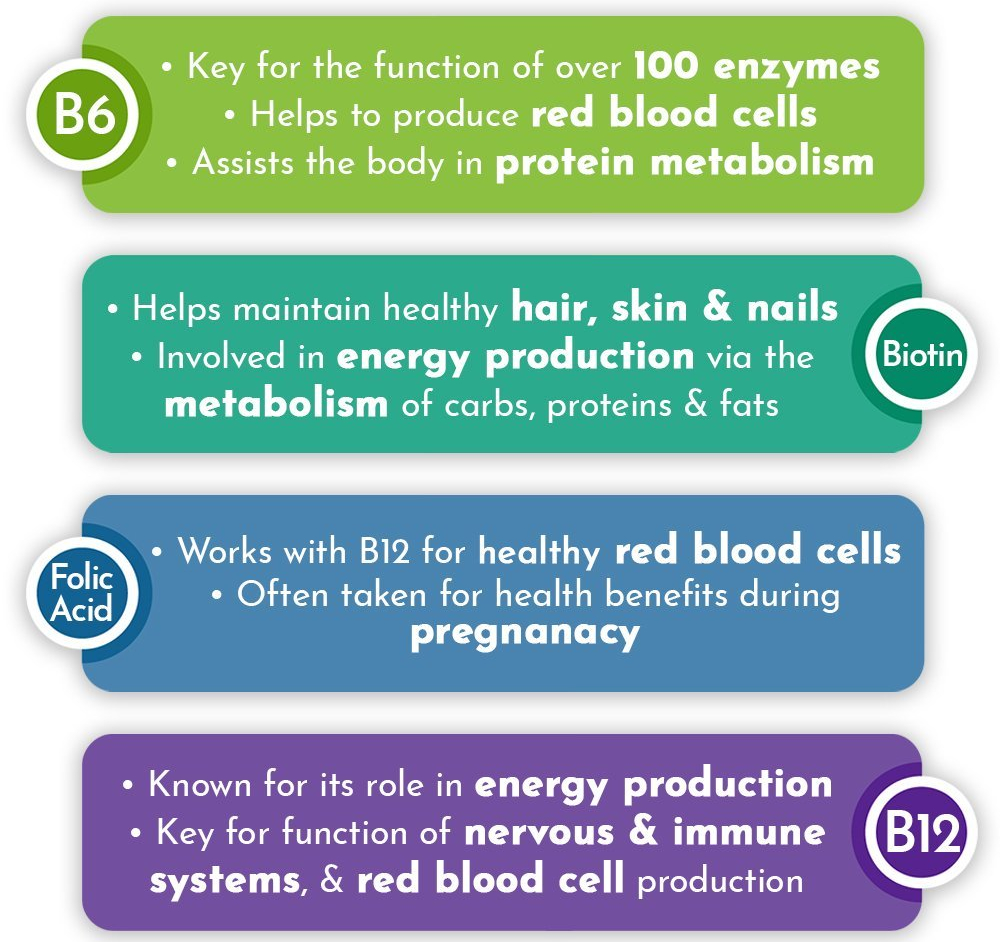
Three important, essential B Vitamins, B6, Pyridoxine, B9, Folic acid, and B12, Cyanocobalamin are so intertwined in their effects, they are best considered a unit. For instance, if B9 is supplemented while B12 is deficient, severe neurological problems arise. B6,9 and 12 must be kept balanced.
That leaves B1,B2, and B3, Thiamine, Riboflavin, and Niacin. Thiamine and Niacin deficiencies used to be common, especially when white rice and white flour replaced the more common brown variety, and led to Beri-Beri and Pellagra respectively.
My own Medicine Cabinet used to have the enriched B-vitamins, called B50 and B100 at Trader Joes. To cut down on pills, I switched to a multivitamin rich in most B vitamins. With the additional 4 mg. of Folic acid, I now take 1000% of the MDR of B6, B9 and B12, which I explained in a previous post to be driven by my elevated Homocysteine.
The Medical establishment and much research demeans the “health food nuts” as doing little more than making their toilets healthier. Indeed, research on Vitamin E supplementation has shown to cause cancer, Vitamin D supplementation to be useless, and folic acid supplementation to be potentially bad. Vitamin C supplementation does nothing but increase the likelihood of Kidney stones, etc.
The experiments are performed, and MDRs calculated on GROUPS of people, however, and with the INDIVIDUAL VARIATION in metabolism, with AGING of the human body (research on nutrients rarely includes the Elderly), and the lousy fast foods of the modern diet, I will continue with my supplementation.
In 2 of the vitamins, D and folic acid, B9, I am on firm ground, having blood levels of 25 hydroxy Vitamin D, and Homocysteine respectively to give me a frame of reference.
The truth is that the medical profession is poorly educated in nutrition, has little incentive to improve their knowledge, and has scant spare time to take dietary histories even if they knew more.
Even in the 60s when I routinely had my Patients keep a “diet diary” so I knew what they were eating, most doctors did not think this worth the time.
Educate yourself on SLEEP, DIET and EXERCISE, resolve to practice what you learn, and leave the medical profession to do what they are best at, and paid for: give medicines and perform procedures and surgery.
